
Abstract
Nivolumab is an immune checkpoint inhibitor that is used to treat various advanced cancers, including metastatic non-small cell lung cancer (NSCLC). Nivolumab treatment has different side effects. For this patient with advanced NSCLC, pericardial effusion was considered to be an immune-related adverse event after immunotherapy. It was characterized by deterioration of symptoms and considered to be pseudo-progression. The pericardial effusion gradually disappeared as nivolumab treatment continued during intensive follow-up monitoring. After chemotherapy and disease progression, the patient was treated with oral targeted therapy based on genes that were detected. After the re-imaging to assess the targeted therapy progress, immunotherapy was used. During immunotherapy, the patient showed increased pericardial effusion, and he underwent one pericardial puncture, in which 200 mL of pericardial effusion was drained. The pericardial effusion after puncture was not diagnosed as malignant by pathology, and the pericardial effusion remained. Shortness of breath continually improved during immunotherapy, and immunotherapy was continued with close observation. After 11 cycles, pericardial effusion had resolved. This case suggested that NSCLC pericardial effusion that was caused by an immune-related adverse event after immunotherapy might be considered to be pseudo-progression.
Keywords
Introduction
Nivolumab is an all human immunoglobulin G4 monoclonal antibody that is also directed at programmed cell death 1 (PD-1). 1 PD-1 ligands (PD-L1 and PD-L2) can be blocked, and blocking the activation of PD-L1, which is over expressed in some cancer cells, and PD-L2, which is mainly expressed in antigen-presenting cells, enhances the activation of T cells and the cell-mediated anti-tumor immune response. Nivolumab inhibits the interaction between the PD-1 receptor and its ligands (PD-L1 and PD-L2), and restores antitumor immunity. 2
Any drug treating a disease will always have adverse reactions. The adverse response to immunotherapy is unique, such as rashes, itching, diarrhea, interstitial pneumonia, and even myocarditis. Here, we present the case of a 59-year-old patient with metastatic squamous cell carcinoma of the lung, who had disease progression after first-line chemotherapy and second-line targeted therapy, and who subsequently received third-line treatment with nivolumab.
Case presentation
A 59-year-old male presented with a history of cigarette smoking (24 packs per year) and shortness of breath for 1 month.
History of the present illness
After treatment with carboplatin and pemetrexed for two cycles, the lesions on the right pulmonary portal system increased in size compared with before treatment. The patient’s genetic test showed TP53, KRAS, and MET mutations. Then, based on the disease progression, the patient received crizoltinib and was evaluated for its efficacy after 2 months. A small amount of pericardial effusion was detected before treatment with nivolumab.
Physical examination upon admission
The patient attended our hospital and was admitted. The patient provided consent to publish the details of his case. His temperature was 36.4°C, heart rate was 65 beats/minute, respiratory rate was 15 breaths/minute, blood pressure was 120/85 mmHg, and indoor air oxygen saturation was 99% upon admission. There was hypoventilation in auscultation.
Laboratory examinations
Blood routine, urine sediment, stool routine, occult blood, and blood biochemistry test results as well as infection indexes were all normal. No epidermal growth factor receptor (EGFR) mutation or ALK gene rearrangement was detected. The tumor mutation burden (TMB) value in plasma and tissue was 13.9 Muts/Mb and 9.9 Muts/Mb, respectively.
Imaging examination
Before immunotherapy, the computed tomography (CT) imaging (cT4N3M1a, stage IVA) of the patient’s chest suggested that the right lung tumor blocked the right lung lower bronchial tube and that middle bronchial tube mediastinal invasion and mediastinal multiple lymph node metastasis were present, combined with obstructive pulmonary dysplasia in the lower right lung (Figures 1a–1d). For N3, where was a right supraclavicular lymph node metastasis and for M1, there was malignant pleural effusion. Fluorodeoxyglucose (18F-FDG)-positron emission tomography (PET)/CT showed no metastasis in the head, bone, liver, and adrenal glands before nivolumab treatment.
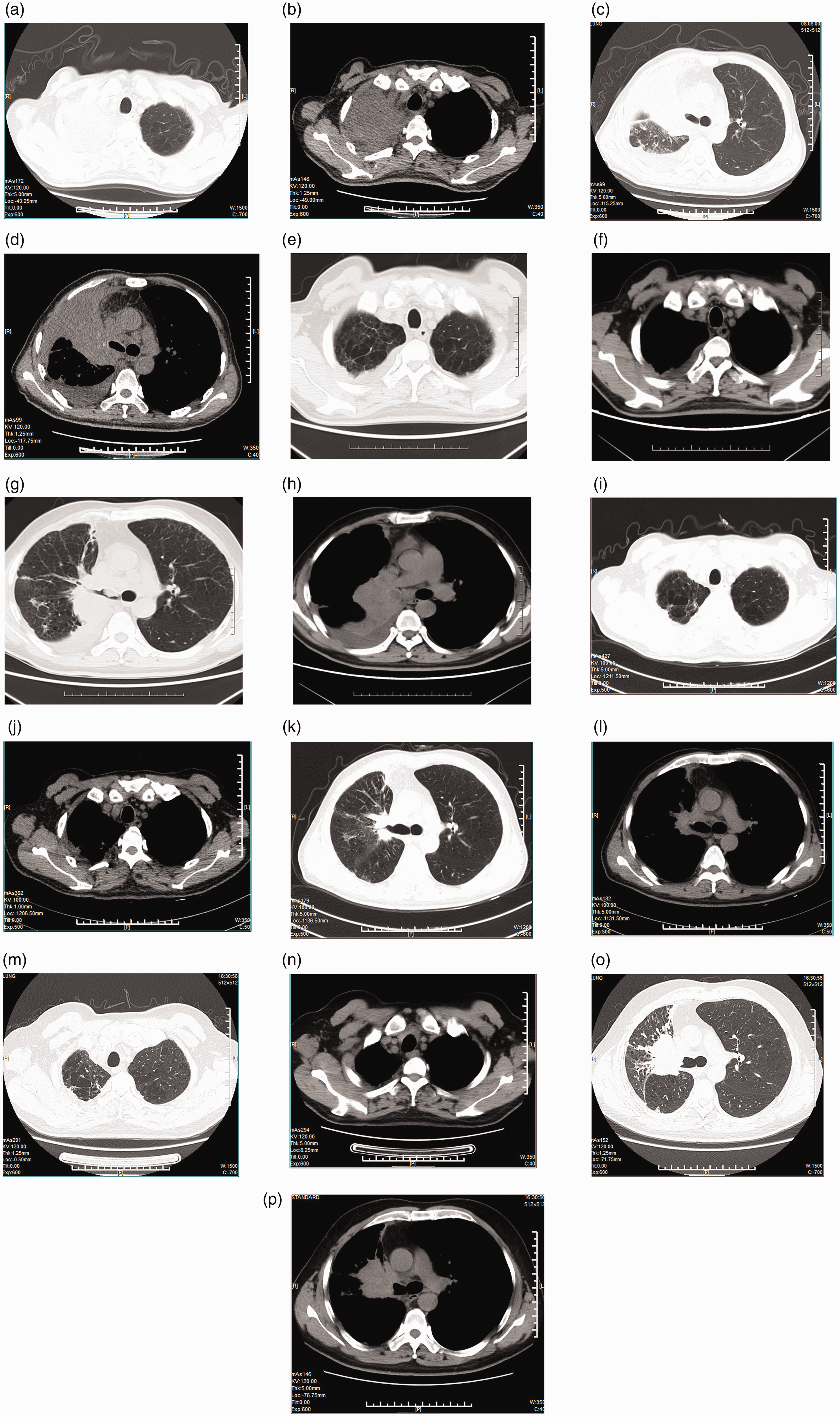
(a–d) Lung and mediastinal areas on computed tomography (CT) before nivolumab treatment showed a right pulmonary portal mass and right pulmonary dissection. (e–h) The CT results after two cycles of nivolumab treatment showed tumor reduction. (i–l) The CT results after four cycles of nivolumab treatment showed significant reduction of tumor and mediastinal lymph nodes. (m–p) One year after nivolumab treatment, reexamination of CT showed that the lesion was 50% larger compared with the previous CT scan.
Diagnosis and treatment
The patient was diagnosed with adenocarcinoma of the right lung (cT4N3M1a, stage IVA). Nivolumab therapy was initiated for the patient (3 mg/kg every 2 weeks) as a third-line therapy.
Outcome and follow-up
The amount of pericardial effusion was decreased after the first cycle of nivolumab immunotherapy (Figures 2a and 2b). After four cycles of immunotherapy, the patient had dyspnea, and a heart color ultrasound showed a large amount of pericardial effusion (Figure 2c). However, the symptoms resolved after immediate cardiac puncture to drain the effusion. During the subsequent treatment, the median pericardial effusion was reviewed twice (Figures 2d and 2e). The patient had no obvious symptoms such as dyspnea, and echocardiography showed no separate liquid region in pericardial cavity. Thus, we suggest that the patient’s quality of life had been improved compared with pre-nivolumab treatment. To date, the patient has been treated with nivolumab for 15 months, and the latest follow-up showed that the tumor size had increased (Figures 1m–1p).

(a) Echocardiography indicated less pericardial effusion before nivolumab administration. (b) A small amount of pericardial effusion was detected after one cycle of nivolumab administration. (c) A large amount of pericardial effusion was observed after four cycles of nivolumab administration. (d) Medium pericardial effusion was observed after 2 months of treatment with nivolumab. (e) Medium pericardial effusion was observed after 3 months of treatment with nivolumab. (f) Echocardiography showed no separate liquid region in pericardial cavity after 4 months of therapy. (g) No pericardial effusion was detected by echocardiography after 1 year of nivolumab treatment. (h) No pericardial effusion occurred after 15 months of nivolumab treatment.
Discussion
Previous studies indicated that NSCLC patients with TP53 or KRAS mutation might be sensitive to nivolumab treatment. 3 This case may support their conclusion. The patient described in our case report had TP53-PV172F and KRAS-G12C mutations and abnormal c-MET gene abundance,4–10 and these mutations and TMB11,12 might be related to the sensitivity to nivolumab treatment.
In this study, a small amount of pericardial effusion was detected before treatment with nivolumab. After two cycles of treatment, the amount of pericardial effusion was not significantly changed compared with that before treatment. After four cycles of treatment, a large amount of pericardial effusion appeared. Our patient underwent pericardial effusion drainage once, and continued nivolumab for seven additional cycles, but without hormone treatment. The patient’s pericardial effusion was observed to decrease and it disappeared after 40 days. Unfortunately, in our case, we did not detect the main indicator of inflammatory cell infiltration in pericardial effusion (including lymphocytic pericardial effusion) because the patient did not agree to undergo the procedure. Taking our findings and previously published findings into account,2,13–15 we suggest that pericardial effusion was caused by pseudo-progression. However, this requires further study to confirm our results.
Conclusions
We believe that in similar cases, identifying pericardial effusion that is caused by possible pseudo-progression may improve the prognosis in NSCLC patients by allowing the continuation of nivolumab treatment. Additionally, advanced NSCLC patients with TP53, KRAS, and MET mutations might benefit from additional nivolumab treatment. However, the requirement for continuous treatment is strict observation and follow-up.
Footnotes
Author contributions
ZC and YY conceived of the study and drafted the manuscript. ZC collected the data. YY participated in writing and editing as well as data collection. YY edited the manuscript. All authors read and approved the final manuscript.
CARE Checklist (2016) statement
The manuscript was prepared and revised according to the CARE Checklist (2016).
Declaration of conflicting interest
The authors declare that there is no conflict of interest.
Funding
This work was supported by grants from the CSCO Lizhu Cancer Research Fund for Traditional Chinese Medicine (Grant no. Y-L2019-01) and the Technology Million Project of Inner Mongolia Medical University (Grant no. YKD2018KJBW(LH)060).
Informed consent statement
Informed consent was obtained from the patient to publish the details of his case in this case report.
Supplemental material
Supplemental material for this article is available online.