
Abstract
Background:
Knowledge about cancer-related malnutrition and the use of clinical nutrition (CN) in the real-world setting are lacking. We investigated diagnosis and treatment frequency of malnutrition in a multinational survey to identify unmet needs in cancer patients’ care.
Methods:
Retrospective analyses were conducted on data from three administrative healthcare datasets from France (n = 570,727), Germany (n = 4642) and Italy (n = 58,468). Data from France described frequency and timing of malnutrition diagnosis in hospitalized gastrointestinal cancer patients. The German data detailed home parenteral nutrition (HPN) use in cancer patients with stage III/IV cancers. The Italian data analysed three cohorts: metastatic with CN, metastatic without CN, and patients without metastatic disease.
Results:
In France, malnutrition diagnosis at first hospitalization occurred in 10% of patients, 13% were subsequently diagnosed, and 77% had no malnutrition diagnosis. In Germany, 16% of patients received HPN. Patients started HPN around 3 months before death. In Italy, 8.4% of metastatic cancer patients received CN; average time between metastasis diagnosis and first CN prescription was 6.6 months. Average time between first CN prescription and death was 3.5 months.
Conclusions:
These data indicate that in the real-world clinical practice, cancer-related malnutrition is under-recognized and undertreated. CN often appears to be prescribed as an end-of-life intervention or is not prescribed at all.
Appropriate CN use remains challenging, and current practice may not allow optimal oncologic outcomes for patients at nutritional risk. Improving awareness of malnutrition and generating further evidence on clinical and economic benefits of CN are critical priorities in oncology.
Introduction
Cancer has been reported among the leading causes of morbidity and mortality worldwide, with the number of cases expected to continue to rise. 1 Although treatment efficacy is improving, the development of malnutrition, induced by the tumour or treatment side effects, remains a frequent and important barrier to achieving the best possible outcomes. 2 Depending on the cancer diagnosis and stage, malnutrition has been estimated occurring in approximately 30–60% of cancer patients,3–8 and is associated with increased morbidity and mortality. 9 Malnutrition in cancer patients can be referred to as cachexia, which is considered a result of complex interplay between underlying disease, disease-related metabolic alterations and, in some cases, the reduced availability of nutrients (due to reduced intake, impaired absorption or increased losses, or a combination of these). Malnutrition is a state of nutrition in which a deficiency or excess (or imbalance) of energy, protein, and other nutrients causes measurable adverse effects on tissue/body form (body shape, size, and composition) and function, and clinical outcomes. Reduced nutrient availability, however, may be a component of, and play a role in, the pathogenesis of cachexia. Notably, cachexia is not always present in all malnourished patients, whereas all cachectic patients suffer from malnutrition. 10 Research suggests that around 20–30% of cancer patients may die due to consequences of malnutrition, rather than cancer itself. 9
The European Society for Clinical Nutrition and Metabolism (ESPEN) has published guidelines and a position paper recommending nutritional screening in all cancer patients. 11 In addition, countries such as Scotland and the Netherlands have established mandatory screening for malnutrition in cancer patients. 2 More recently, the Italian Ministry of Health published the official guidelines for the nutritional pathways for cancer patients, in collaboration with the joint Working Group by the Italian Association of Medical Oncology, the Italian Society of Artificial Nutrition and metabolism, and the Italian Federation of Volunteer-based Cancer Organizations. 12
Despite all these recommendations, malnutrition often remains overlooked 13 and even if diagnosed, is untreated in about 50% of cases.4,14 Importantly, there is increasing evidence supporting how clinical nutrition (CN) intervention can be associated with decreased therapy toxicity, improved relative-dose intensity (RDI), with fewer treatment delays and dose modifications.15,16 As a result, especially when it is initiated at the time of diagnosis or as soon as nutritional risk is detected, CN offers the potential to improve cancer patients’ outcomes, such as quality of life and overall survival. 17 Despite the increasing awareness of the negative impact of malnutrition on clinical outcomes in cancer patients, the understanding of malnutrition rates, as well as the use of CN in the real-world setting, is lacking. Our overall objective in this research investigation was to describe the management of malnutrition among cancer patients in current clinical practice, using real-world data from large administrative healthcare datasets from three European countries. Several analytical methodologies were applied to characterize and demonstrate meaningful insights into different aspects of cancer patients’ care. Specifically, (a) diagnosis, frequency, and rates of malnutrition, and (b) the use of CN in hospitalized cancer patients and in the homecare setting were examined.
Methodology and data analysis
The original research investigations were conducted separately for each country. The methodology and data analysis for each study in each country are described separately.
France
Malnutrition diagnosis frequency and timing were investigated, based on data from the French Hospital database PMSI (Program for the Medicalization of Information Systems), and Medicine, Surgery (Chirurgie), Obstetrics. The database contained information on reported diagnosis, procedures and included mean values for drugs used in each diagnosis group. 18 The study period ranged from 1 January 2013 to 31 December 2016 and inclusion criteria were: a first gastrointestinal (GI; colon–rectal–anal, liver/biliary tract, pancreas, stomach, and esophagus) cancer-related hospital stay, as defined by the algorithm for attribution of hospitalizations related to cancer developed jointly by the Hospital Information Technology Agency, the National Cancer Institute (INCA) and representatives of public and private hospitals from the INCA during the study period 2013–2016. The index date was defined as the date of the first cancer-related hospitalization. All patients without any GI-cancer-related hospitalization were included in the 2 years preindex date (Table 1). Multiple hospitalizations were possible for each patient. Malnourished patients were required to have an International Statistical Classification of Diseases and Related Health Problems (ICD)-10 malnutrition diagnosis code and an accompanying diagnosis code of at least moderate or severe malnutrition in the PMSI database [as defined by the French Health Authorities recommendations (HAS 2007) and the associate diagnosis codes (DAS) for moderate (E440) and severe (E43) malnutrition]. Patients were grouped into three diagnosis categories: (0) no malnutrition diagnosis in the study period; (1) malnutrition diagnosis at first GI-cancer-related hospitalization (early diagnosis); and (2) malnutrition diagnosis after first GI-cancer-related hospitalization (late diagnosis). The frequency of the diagnosis in each category was also assessed.Germany
Main characteristics for each study.

ATC, Anatomical Therapeutic Chemical Classification; ATIH, Hospital Information Technology Agency; CM, clinical modification; CN, clinical nutrition; CRC, colorectal cancer; GI, gastrointestinal; H&N, head and neck; HPN, home parenteral nutrition; ICD, International Classification of Diseases and Related Health Problems; INCA, National Cancer Institute; i.v., intravenous; LHU, Local Health Units; PMSI, Program for the Medicalization of Information Systems; SHI, Statutory Health Insurance.
Data from over 4 million insured individuals from approximately 70 Statutory Health Insurance organizations, including information on services, prescriptions, and procedures were used to select patients who died in the study period from 1 January 2010 to 31 December 2016 and had a diagnosis of head and neck (H&N), colorectal (CRC), ovarian, pancreatic, and gastric cancers. The study population included deceased patients with locally advanced carcinoma stage III or metastatic stage IV cancers. The index date was defined as the date of an initial prescription of guideline-recommended pharmacotherapy or the first PN prescription administered at home (home parenteral nutrition, HPN). A 3-year preindex observation period was required before the first prescription (Table 1). The study described the frequency and timing of HPN use stratified by cancer type. Furthermore, the study identified the proportion of patients with cachexia (as defined by ICD-10 diagnosis codes) among patients who received HPN compared with those who did not receive HPN.
Italy
The use of CN, defined as enteral nutrition (EN) with or without parenteral nutrition (PN) in oncology patients was assessed, based on an integrated administrative database using data from 10 Italian Local Health Units (LHUs). The administrative database for healthcare resource use included information from a pharmaceutical database, a hospitalization database, laboratory tests, diagnostic tests and specialist visits database. The database covers 5.9 million people from various regions in the northern, central and southern Italy, representing around 10% of the total Italian population.
The study period was from 1 January 2009 to 31 December 2015. All patients with a diagnosis of H&N, gastrointestinal, respiratory, genitourinary, or haematologic malignancies defined by ICD-9-CM during the study period and a 12-month, available, pre- and postindex observation period were included. ICD-9 disease classification codes were used in Italy because the observation period started in January 2009. The new ICD-10 CM coding system took effect from October 2015. The index date was defined as the date of the first metastasis diagnosis or the first prescription of CN after diagnosis. Selected Anatomical Therapeutic Chemical Classification (ATC) codes {A11BA: oral multivitamins, plain; B05BA: solutions for parenteral nutrition [glucose at low concentrations (<20%) were excluded]; B05XB: amino acids [intravenous (i.v.) solution additives]; B05XC: vitamins (i.v. solution additives)} in combination with ICD-9-CM procedural codes for enteral/parenteral infusion of concentrated nutritional substances (ICD-9-CM 96.6; ICD-9-CM 99.15) and at-home nutritional product prescriptions were used to define CN (Table 1). Patients were divided into three cohorts: metastatic with CN, metastatic without CN, and patients without metastatic disease. The proportion of nonmetastatic and metastatic patients receiving CN was assessed. In addition, the time from metastasis diagnosis to the initiation of CN intervention and the time from initiation of CN to death were further investigated.
Statistical analysis
High-dimensional statistically relevant propensity-score matching (PSM)-based analysis was used to match patients by age, sex, and comorbidities, and were used as variables in the regression analysis. PSM had to show significant differences in cancer patients with and without CN. PSM reduces the bias due to confounding variables and achieves better comparability between the matched groups.
Descriptive statistical analysis of correlations was based on individual level data. Statistical parameters included: mean, standard deviation, median, minimum/maximum, with 95% confidence interval (CI), and p value < 0.05 was considered statistically significant. All statistical analyses were performed using STATA SE, R (statistical software, StataCorp LLC, College Station, TX, U.S.), and the Microsoft Excel application.
Results
The results are presented separately for each study.
France
The study population identified 570,727 GI cancer patients with a first related hospital stay between 2013 and 2016. The distribution of patients by cancer types is shown in Figure 1.

Distribution of GI cancer patients by type of cancer.
Malnutrition diagnosis at first hospitalization was reported in the PMSI database for 10% of patients with GI cancer, 13% were diagnosed after the first hospitalization and 77% had no diagnosis of malnutrition during the study period. The proportion of patients for whom malnutrition was reported ranged from 14% in CRC cancer patients to 38% in patients with pancreatic cancer. For all types of cancer, the 2016 PMSI data reports about 1.2 million cancer patients in France, of which one third are reported with a malnutrition code (as defined by ICD-10 criteria), which is substantially lower than previous prevalence estimates in the available literature 4 (Figure 2).
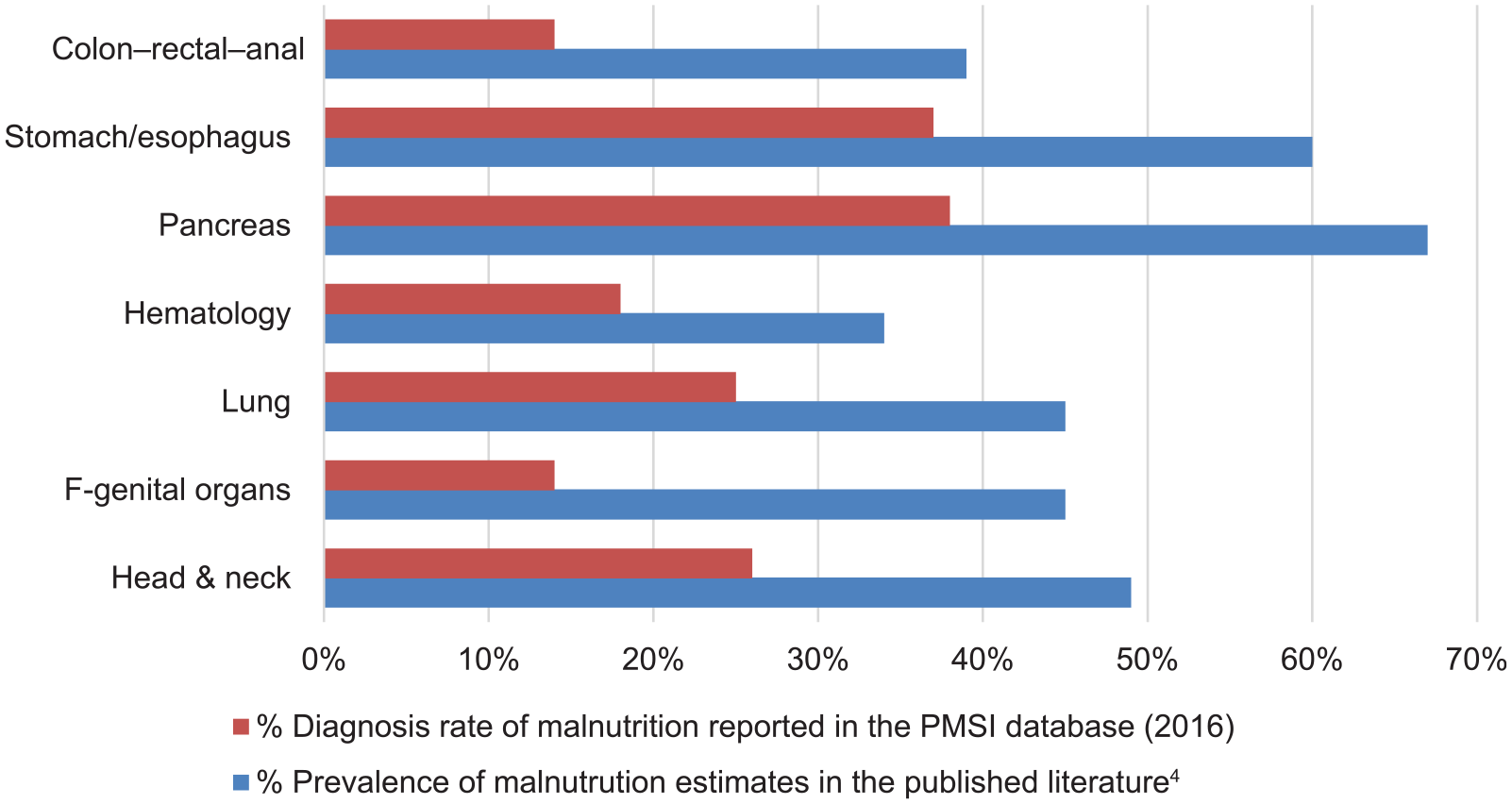
Comparison between prevalence estimates of malnutrition previously reported in the literature and frequencies found in the French Program for the Medicalization of Information Systems database.
Germany
The study population included 4642 patients [most patients were male (59%); age, mean (95% CI): 67 (62.9–71.6) years] with late stage III or IV cancer. A total of 343 had H&N, 1966 CRC, 327 ovarian, 1406 pancreatic, and 600 gastric cancer (Table 2). Across five cancer types, the proportion of patients who received HPN was 16%, on average, with the lowest rates in H&N (12.5%), followed by CRC and pancreatic cancer (14.8% and 14.9%, respectively), ovarian cancer (18.9%), and the highest rates in gastric cancer with 25.5% (Table 2). The time from initiation of cancer treatment to initiation of HPN varied widely by type of cancer, with approximately 6 months for gastric and more than 2 years for ovarian cancer, with an average of 337 days delay across five cancer types (Table 2). The data suggest that patients who received HPN survived longer (range: +29 days for CRC and up to +118 days in gastric cancer) than those patients who did not receive HPN (Table 2).
Average time delay until HPN initiation and period until death between patients who received and did not receive HPN by cancer type.

HPN, home parenteral nutrition.
Descriptive data analysis across five cancer types showed that initiation of HPN was predominantly an ‘end of life’ intervention, with time to death of approximately 3 months. To put these findings in perspective, the proportion of cachexia in patients with CRC was nearly identical between patients who received HPN (45%) and those who did not receive it (47%).
Italy
Out of 69,000 metastatic cancer patients, 8.4% received CN; among these, 89% had PN. In a subanalysis of 190,000 patients without metastasis, 3.11% received CN (Figure 3).

Use of clinical nutrition in metastatic and nonmetastatic cancer patients in the Italian cohort.
Among metastatic patients with selected cancers (H&N, gastrointestinal, respiratory, genitourinary, or haematological: n = 58,468), 8.2% received CN, of which only 11% had the diagnosis of malnutrition reported. The average time between the diagnosis of metastasis and first use of CN was 6.6 months.
Approximately 35% of patients started CN in the first month after diagnosis of metastasis (Figure 4, left panel). For approximately 18% of patients, more than 1 year passed between metastasis diagnosis and the first use of CN. The average time between the first use of CN and death was 3.5 months. Furthermore, approximately half of metastatic patients received CN just before death, and this pattern was observed across all cancer types. A total of 15% of metastatic cancer patients received CN more than 7 months before they deceased (Figure 4, right panel).
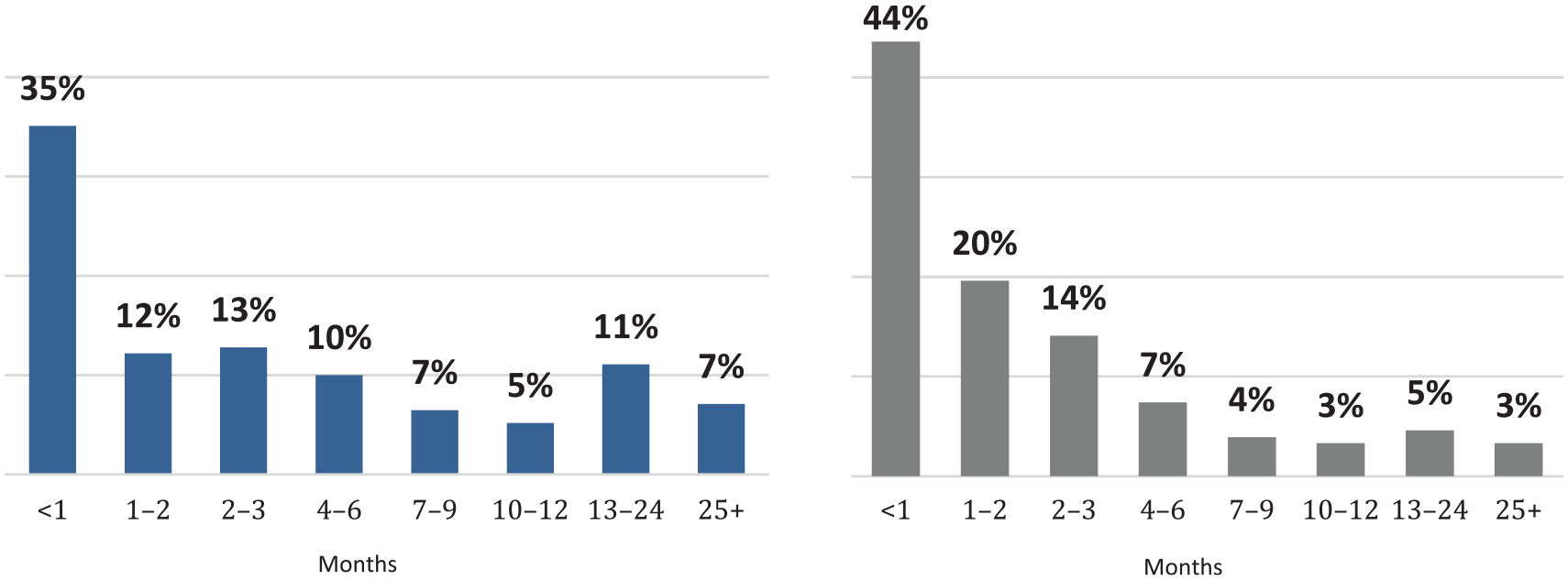
Percentage of patients by month from diagnosis of metastasis to clinical nutrition treatment (left panel) and from clinical nutrition treatment to death (right panel).
Discussion
These studies investigated different aspects of current practices and use of CN in oncology, based on the real-world administrative datasets from three European countries (France, Germany, and Italy), using different analytical methodologies. The data provide a broad overview of different characteristics, including actual clinical practices, areas with existing clinical unmet needs, and a potential for improvement in treating cancer-related malnutrition.
In general, the study results from all three countries suggest that the diagnosis of malnutrition in clinical practice occurs later and less frequently than what is recommended according to the current clinical guidelines2,19 or what is generally reported in the literature.4,14 Late or lack of diagnosis of malnutrition can reduce the potential benefits of earlier nutritional intervention in cancer patients.15–17,20,21 More up-to-date data would be necessary to understand current adherence to the recently published ESPEN guidelines for clinical nutritional care in patients with cancer. 2 Moreover, the data showed that the diagnostic procedures of malnutrition may not be optimal in hospital and homecare settings, given that the reported proportion of patients with a diagnosis of malnutrition was found to be considerably lower than expected. The currently available literature suggest that the general prevalence of malnutrition is about 30–60% in cancer patients4–6,8,14 and can be significantly higher in specific cancers (85% in pancreatic cancers). 22 The low rates of reported malnutrition diagnosis in France, where treatment is mandatory, the low utilization of HPN in Germany, and the very low proportion of patients receiving CN in Italy indicate that malnutrition in the real-world clinical setting is underdiagnosed or totally overlooked and that, as a result, appropriate CN therapy remains underutilized. This conclusion is also supported by other published studies. 4 Diagnostic procedures for malnutrition can be considerably improved, in line with recent calls for routine screening. 23 These data support the importance for the European Society for Medical Oncology (ESMO) and the American Society of Clinical Oncology (ASCO) to include in future guidelines the proactive and standardized use of validated nutritional screening and assessment tools for all cancer patients or patients with cancer known to be at risk for malnutrition with or without weight loss.
Early intervention with nutritional supplementation has been reported to halt progression of malnutrition and may improve outcomes in some patients.15–17,20,21 However, the results from Italy and Germany showed that CN was often used as an end-of-life intervention, as it was used 3–4 months or shortly just before death. The late initiation of CN represents a lost opportunity to improve patients’ care. 24 This is also in accordance with the position paper from the European School of Oncology Task Force has highlighted that ‘early detection of malnutrition and cachexia will be increasingly important in the hope that timely intervention can improve both patient-centred and oncology outcomes.’ 25 In addition to the importance of improving cancer patients’ outcomes, it is of great relevance from an economic perspective, given that the financial impact of malnutrition has been estimated as very high.26–30
However, further studies on the patterns of CN use, specifically investigating the clinical benefits of early interventions and factors that influence the practical implementation of these aspects, are required to encourage the best practices for screening and treatment of malnutrition. Some countries have already established mandatory screening procedures for malnutrition in cancer patients. Future clinical and health economic research may include comparative studies to established current prevalence rates and treatment of malnutrition between countries with and without mandatory screening policies.
Limitations
There are several limitations that should be kept in mind when interpreting the findings from these studies in each country. The primary limitation for each study was that the data from administrative datasets were not collected specifically to be used in health-related scientific research and lacked detailed clinical information. Secondly, the data generated from the three large national databases in France, Germany, and Italy were not merged, as the datasets were not directly comparable due to different design, methodological approaches used, and only descriptive and exploratory analyses performed. Furthermore, the additional subanalyses stratified by each cancer type conducted in each country to understand the use of healthcare resources and clinical outcomes in patients receiving CN, compared with those who not receiving CN, were not included in this assessment and will be published separately. Considering these limitations, this research analysis still holds its significance with multifaceted and compelling insights derived from this first look at the real-world application of CN in oncology allowed the characterization of several interesting aspects within current clinical practice. These aspects may be fundamental to further understand the potential clinical and economic benefits of CN in oncology and may also stimulate the design of large prospective clinical nutrition trials.
Conclusion
Multiple investigations across three European countries consistently showed that in the real-world clinical practice cancer-related malnutrition is underdiagnosed, under-reported and undertreated. CN is often prescribed as an end-of-life intervention or not prescribed at all for cancer patients at nutritional risk.
Despite several international recommendations for routine and early nutritional screening, appropriate CN use remains challenging and current clinical practice may not allow the achievement of optimal oncologic outcomes for cancer patients. Improving the awareness of malnutrition and generating further evidence to evaluate clinical and economic benefits of CN as a supportive therapy are critical priorities to optimize cancer patients’ care.
Footnotes
Acknowledgements
The authors would like to thank Anne-Kathrin Fett, (IQVIA Real World Insights) for her helpful editorial assistance in preparation of this manuscript and the three anonymous reviewers for their insightful comments.
Riccardo Caccialanza: conceived and conducted the research, data analysis and interpretation, and drafted the manuscript; Francois Goldwasser: conceived and conducted the research, data analysis and interpretation, and edited the manuscript; Oliver Marschal: conceived and conducted the research, data analysis and interpretation, and edited the manuscript; Faith Ottery: reviewed the manuscript critically for intellectual clinical content; Ingolf Schiefke: conceived and conducted the research, data analysis and interpretation, and edited the manuscript; Patrick Tilleul: reviewed the manuscript critically for intellectual clinical content and edited the manuscript; Gerard Zalcman: reviewed the manuscript critically for intellectual clinical content and edited the manuscript; Paolo Pedrazzoli: conceived and conducted the research, data analysis and interpretation, and edited the manuscript
The content of this manuscript is based on three retrospective observational analyses of administrative databases conducted by the investigators in France, Germany and Italy. Presentations of the results were made and discussions held at the ESMO congress on 19–23 October 2018 in Munich, Germany, and at the International Society for Pharmacoeconomics and Outcomes Research European congress on 10–14 November 2018 in Barcelona, Spain
Three retrospective observational analyses of existing administrative databases in France, Germany and Italy were performed. Due to the nature of the studies, nonclinical anonymised aggregated data from each administrative database were acquired without identifying patients; therefore, formal approval from independent ethics committees was not required. Formal approval for data utilization was obtained from the Institutions responsible for the databases administration (French Hospital database PMSI; German Statutory Health Insurances and Italian LHUs)
Funding
The author(s) disclosed receipt of the following financial support for the research, authorship, and/or publication of this article: these original research investigations were sponsored by Baxter Healthcare AS; no other funding was used. Baxter Healthcare did not participate in the study design, data collection, analysis, interpretation, or writing of the manuscript.
Conflict of interest statement
RC reports personal fees, speakers’ honoraria, research grants, or membership on advisory boards for Akern, Baxter Healthcare, B. Braun, Eli Lilly, Fresenius Kabi, Nestlé Health Science and Nutricia. OM reports speakers’ honoraria for Baxter and Pfizer. IS reports speakers’ honoraria for AbbVie, Gilead, Baxter Healthcare, Intercept, Shire and Jansen. PP reports speakers’ honoraria and teaching for Baxter Healthcare. FO is an employee of Baxter. The other authors declare they have no conflict of interests.
Availability of data and material
The datasets generated and/or analysed during the current study are not publicly available due to legal reasons.