
Abstract
Tackling malnutrition in cancer patients remains one of the most challenging tasks in clinical practice. Even though robust evidence exists stressing the role of nutritional status in relation to treatment outcome, its appropriate consideration in clinical practice is often lacking.
In this review, we discuss the significance of nutritional status and of malnutrition for the cancer patient. Drawn from experience and from current recommendations of the European Society for Clinical Nutrition and Metabolism (ESPEN), we propose concrete and manageable steps to routinely incorporate nutritional aspects in today’s oncological clinical practice.
Highlights
Malnutrition, the result of a poor nutritional status, has a well-documented negative effect on treatment outcome in cancer patients.
(1) Although high-quality randomized controlled trial (RCT)-based evidence is still scarce, data exist showing that timely intervention can lead to improved treatment outcomes.
(2) Comprehensive therapies should include strategies for cancer treatment while maintaining the nutritional status of the patient.
(3) Measures and tools proposed in this article can help to determine the nutritional status and detect and treat malnutrition in a timely manner.
Cancer: an unparalleled challenge for treating physicians
Today, malignant disorders represent the second leading cause of death worldwide. 1 Progressively aging populations, especially in western countries, together with an anticipated global increase of cancer incidence 2 pose new challenges to screening procedures, as well as to diagnosis, treatment, monitoring, and reimbursement.
Recent therapeutic advances have profoundly changed cancer treatment options and outcomes for the better. 3 New substance classes target immune cells, reactivating anticancer-directed immune activities, as well as tumor cells, reducing their burden and leading to increased survival rates. 3 However, tolerability of treatment regimes and outcome of therapy depend on several aspects, one of the most important being the nutritional status of the patient. In this review, we have summarized the current knowledge of nutritional status in oncology in an attempt to provide oncologists involved in the care of patients with cancer with a roadmap for nutritional therapy in their everyday clinical practice.
Based on the recent guidelines from the European Society for Clinical Nutrition and Metabolism (ESPEN) we propose possible nutritional interventions, from diagnosis to treatment and monitoring.
Nutritional status in cancer treatment: current understandings, future challenges
Among hospitalized patients, cancer patients present with the highest prevalence of malnutrition, with 30–50% of hospitalized cancer patients found to be malnourished or at risk of malnutrition, in large European surveys.4–7 Weight loss arises early in the course of disease and may develop at any time throughout the patient’s cancer journey. 8 A recent study in 22 medical oncology centers in Italy with almost 2000 patients showed that 51% had nutritional impairment and 9% were overtly malnourished. 7 Furthermore, the authors found a clear correlation between severity of malnutrition and stages of cancer. 7 A French study evaluating the prevalence of malnutrition in cancer patients (n = 1903) in 154 French hospital wards found that 39% of patients were malnourished. This study also reported that 42.5% of the patients identified as malnourished did not receive any nutritional support. 4 Patient groups at particular high risk of malnutrition include those with head-and-neck cancer and esophageal cancer, undergoing esophageal resection.9,10 It has been reported that malnutrition develops in ~80% patients with esophageal cancer, with dysphagia and weight loss frequently being already present at the time of diagnosis. 11 In patients with pancreatic cancer, both the disease-related impairment of exocrine and endocrine pancreatic function and anticancer treatment effects contribute to the development of malnutrition. 12 More than 80% of patients with pancreatic cancer suffer from significant weight loss already by the time of diagnosis. 13
Malnutrition has a negative impact on clinical outcome and mortality in cancer patients,8,14–17 with adverse consequences, including impaired quality of life, 18 higher rates of complications and worse postoperative outcomes, 19 longer duration of hospitalization, 20 and poorer anticancer treatment tolerance due to increased toxicity, poorer compliance and decreased response.21,22 Severity of malnutrition is an independent predictor of shorter survival. 23
Therefore, the need for adequate nutritional interventions in cancer has been stressed for decades.24,25 In the oncologist’s clinical practice, however, awareness for the nutritional status in cancer patients remains scarce, demonstrated by the fact that it is not regularly assessed in hospitals or ambulatory oncology services as part of standard procedures.26–29
This is even more surprising, since the negative impact of malnutrition on oncological patients’ outcomes has been extensively demonstrated. The pathogenesis of malnutrition in cancer patients is multifactorial in origin. 30 Causes can be both disease or therapy related; for example, anorexia, oral ulceration, intestinal obstruction, xerostomia, diarrhea, nausea, vomiting, cramping, or bloating.8,31–36
Cancer-related loss of skeletal muscle mass, often referred to as sarcopenia,30,37,38 driven by enhanced intramuscular proteolytic systems and triggered by the complex interaction between reduced food intake, possible increased energy expenditure, systemic inflammation, tumor growth, but also through targeted therapies, 39 leads to further deterioration of the patient’s clinical and functional status and to poorer overall prognosis. 30 General consequences of muscle loss in cancer can be physical impairment, as well as increased postoperative complications and elevated chemotherapeutic toxicity.8,37,38,40–44 Loss of muscle mass is a hallmark of cancer cachexia, a cancer comorbidity which has been defined as ‘a multifactorial syndrome characterized by an ongoing loss of skeletal muscle mass (with or without loss of fat mass) that cannot be fully reversed by conventional nutritional support and leads to progressive functional impairment.’ 45 Since cancer cachexia syndrome can develop progressively through various stages, it can be classified, according to its severity (i.e. degree of depletion of energy stores and body protein), into precachexia, cachexia and refractory cachexia. 45 While patients with refractory cachexia are less likely to respond to nutritional therapy, 45 the stages of precachexia and cachexia represent unique and unmissable windows of opportunity for nutritional intervention,8,30 with measurable impact on clinical outcomes, including survival. Indeed, consolidated evidence suggests increased mortality rates associated with cancer cachexia.8,30,46–48
Under-recognition of cancer-related nutritional impairment: a matter of terminology?
One possible obstacle in the daily prevention, recognition, and treatment of cancer-associated malnutrition and cachexia is the current lack of consistent nomenclature (Box 1).

BMI, body mass index.
Malnutrition (synonym ‘undernutrition’) is defined as ‘. . .a state resulting from lack of intake or uptake of nutrition that leads to altered body composition (decreased fat-free mass) and body cell mass leading to diminished physical and mental function and impaired clinical outcome from disease.’ 49 When malnutrition is caused by an underlying disease, be it acute or chronic, it is classified as disease-related malnutrition (DRM). 49 Systemic inflammation plays a major role in the pathogenesis of DRM, but DRM may also occur in the absence of a clinically significant inflammatory response (DRM without inflammation). 49 In this light, cancer cachexia may be considered a form of DRM with inflammation, 49 brought about by a complex and peculiar pathophysiology. 30
Despite the recognized negative impact of DRM on patients’ prognosis and healthcare costs, during recent decades, there has been a fundamental lack of consensus on diagnostic criteria for malnutrition to be applied in clinical settings. As a consequence, DRM remains frequently unrecognized, underdiagnosed and untreated, with its prevalence being extremely variable, depending on the assessment method used.7,49
A combined task force commissioned by four major international clinical nutrition societies (ESPEN, the American Society for Parenteral and Enteral Nutrition, the Parenteral and Enteral Nutrition Society of Asia, and Federación Latino Americana de Terapia Nutricional, Nutrición, Clínica y Metabolismo) has recently proposed a consensus scheme for diagnosing malnutrition in adults in clinical settings, on a global scale. 51 Briefly, the panel of experts has suggested that diagnosis of malnutrition is based on three phenotypic criteria [unintentional weight loss, low body mass index (BMI), and reduced muscle mass] and two etiologic criteria (reduced food intake or assimilation, and inflammation or disease burden). To diagnose malnutrition, at least one phenotypic criterion and one etiologic criterion should be present. Severity of malnutrition may also be assessed based on the degree of deviation of these criteria from normality. 51
Lastly, inconsistencies also exist regarding sarcopenia. The term sarcopenia is commonly and still largely used to define the loss of skeletal muscle mass and function associated with aging. More recently, the European Working Group on Sarcopenia in Older People has defined sarcopenia as ‘primary’ (or age related) and ‘secondary’ (when other causes other than, or in addition to, aging are present, such as chronic diseases; reviewed in the work of Muscaritoli and colleagues 52 ). However, the term sarcopenia is being increasingly used in cancer clinical practice to indicate decreased muscularity as assessed by computed tomography (CT) scan,30,37,38 irrespective of the loss of muscle function. Consensus concerning meaning and use of different terms is warranted in order to harmonize terminology, as well as diagnosis and treatment algorithms of sarcopenia. 53
Effectiveness of nutritional therapy in oncology: where is the evidence?
Another barrier preventing the implementation of structured clinical nutrition pathways in oncology is the lack of high-quality RCT-based evidence of nutritional therapy efficacy. 54 This has considerably weakened the interest of oncologists toward clinical nutrition. Indeed, it must be acknowledged that while the negative impact of cancer-related malnutrition and cachexia is striking, the results on the effects of nutrition on patients’ overall prognosis are weak or inconsistent. Nutritional care and therapy in cancer patients encompass dietician-aided dietary counseling (aimed at improving patients’ spontaneous food intake), oral supplementation with industry-prepared oral nutritional supplements (ONS), enteral nutrition (EN) and parenteral nutrition (PN). 49 The term ‘nutritional therapy’ is used when active interventions are implemented with ONS, EN or PN. ‘Medical nutrition’ utilizes ONS, EN and PN to prevent or correct DRM, depending on the clinical indications and patient’s clinical condition. 49
Growing evidence supports active nutritional interventions in the oncological patient. In cancer patients who were malnourished or at risk of malnutrition, oral nutritional support or dietary counseling were shown to improve energy intake and body weight55,56 but had no effect on clinical outcomes of oncological relevance, such as survival and treatment toxicity. In patients with colorectal cancer undergoing radiotherapy, individual dietary counseling and ONS improved nutritional status and reduced early and late radiotherapy-induced toxicity. 57 The long-term follow up of this study showed the longest survival rates in patients with intensified nutritional counseling compared with usual diet plus supplements and usual diet alone. 58
Nutritional interventions in head-and-neck cancer patients yielded more consistent results. Early nutritional intervention ranging from counseling (for patients with low nutritional risk) to ONS or EN via tube (for those with higher nutritional risk) reduced weight loss, frequency and duration of treatment interruptions, as well as rehospitalizations.59,60 In high-risk patients, for example, with hypopharyngeal primary site, T4 tumor, female sex, or receiving combined radiochemotherapy, prophylactic percutaneous endoscopy gastrostomy (PEG) was associated with fewer malnourished patients over time and higher quality of life.61,62 Early nutritional intervention with either counseling ONS or EN was associated with reduction of treatment interruption and duration of hospitalization. 63
In selected cancer patient populations, mainly in those whose gastrointestinal function is partially or totally impaired, PN may play an essential role in maintaining nutritional status. In patients with advanced pancreatic cancer, supplemental parenteral nutrition improved nutritional status.64,65 Two studies focusing on the impact of home parenteral nutrition (HPN) in cancer patients could show that HPN is associated with an improvement in nutritional status, as well as quality of life.66,67 In summary, the available studies addressing the effects of nutrition care or therapy on cancer patients’ outcomes is still insufficient or inconsistent. Further high-quality RCT-based evidence is needed to better identify the categories of cancer patients in whom nutritional therapy may be cost effective in impacting outcomes of oncological relevance.
Simultaneously targeting the tumor and nutritional and metabolic derangements: the oncological parallel pathway
Because of their high incidence and prognostic relevance, screening for and assessment, treatment and follow-up evaluations of nutritional deficits should be implemented as a standard second pillar in cancer therapy (Figure 1). The nutritional and metabolic (e.g. inflammation-driven impaired glucose tolerance, muscle hypercatabolism, anabolic resistance) changes should be attended to in parallel to all oncological treatments and during all stages of a patient in cancer disease. Thus, the aim is to start nutritional management early in the course of the disease, beginning with the assessment of nutritional status at the time of diagnosis, and starting nutritional interventions in parallel with cancer therapies. 68 Nutritional strategies should be adapted to different cancer stages and treatments, and all options of nutritional therapy should be explored, including ONS, EN or PN, as appropriate, in patients who are not able to fully meet their nutritional requirements by the oral route,8,68 according to existing clinical practice guidelines and recommendations on nutrition in cancer patients. 8
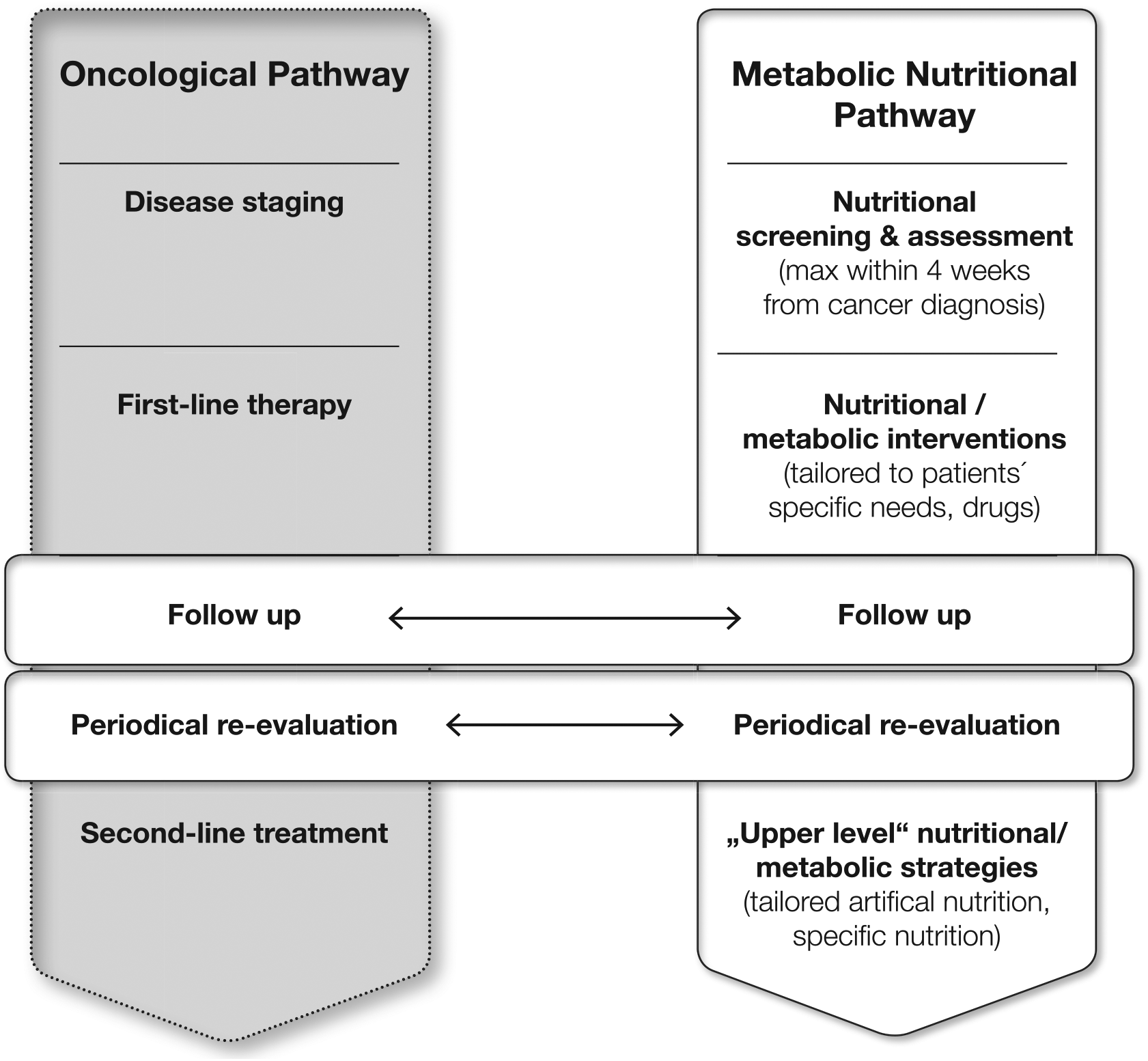
Continuum of care for the cancer patient: the parallel pathway in oncology (developed from Muscaritoli et al. 68 ).
Multifactorial patient needs require a multidisciplinary team approach: the role of the oncologist
Cancer treatment represents a continuum of care, from diagnosis to treatment and follow up. Addressing stage- and condition-dependent patient needs should be at the center of all treatment decisions. To be optimized, such individualized approaches cannot be shouldered by the treating oncologist alone, but should best be performed by a closely collaborating multidisciplinary team, led by the hematologist/oncologist and including other medical (e.g. surgeon, gastroenterologist, pain expert, supportive and palliative care expert) and allied specialists (e.g. nurses, dieticians/nutritional therapists, psychologists, and physiotherapists; Figure 2). A comprehensive treatment plan should be designed by the treatment team and regularly reviewed for necessary modifications.
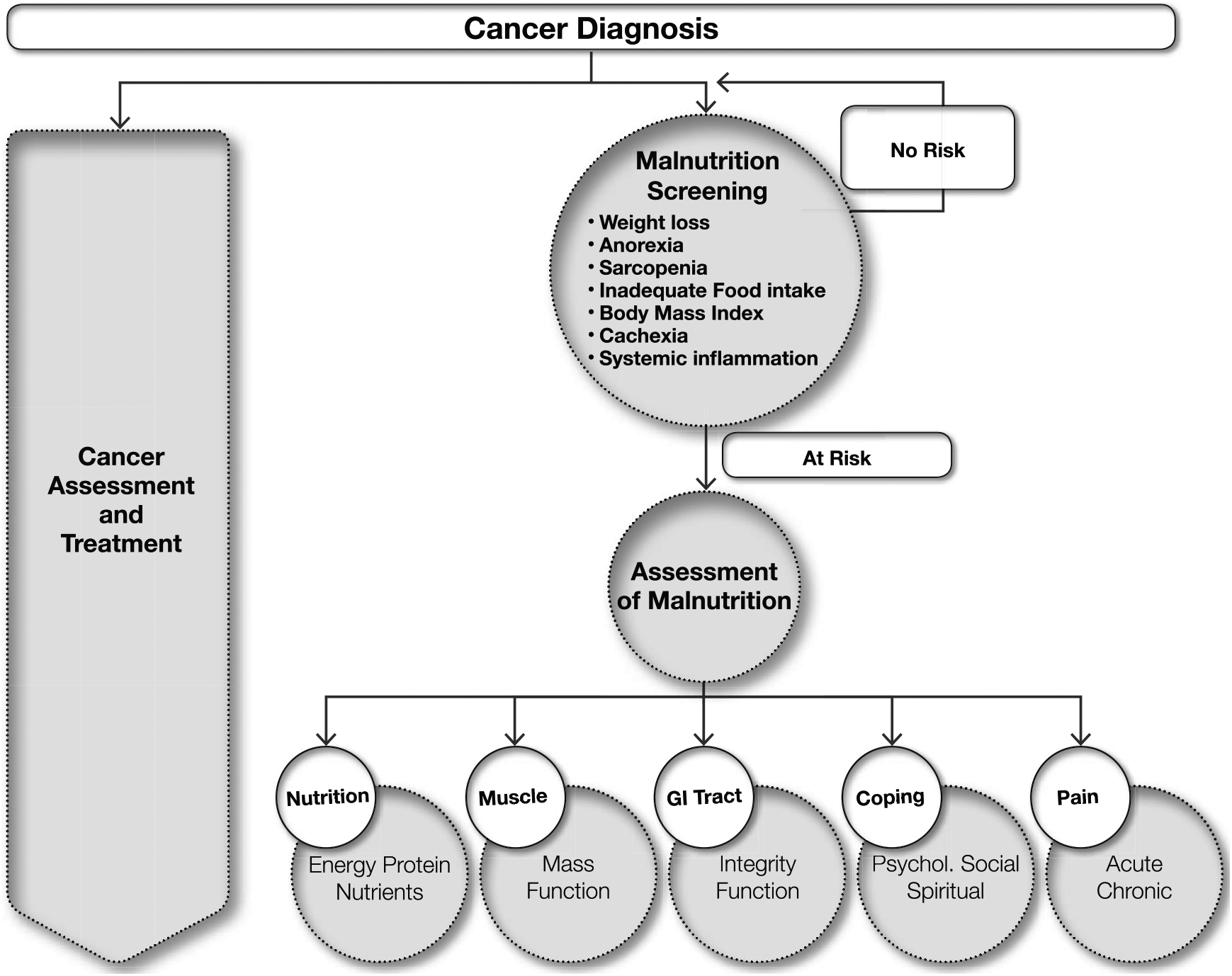
Tackling malnutrition in oncology as a multidisciplinary team approach.
Cancer diagnosis and treatment should be accompanied by a comprehensive screening for and assessment of possible malnutrition. The plan should consider key aspects (e.g. nutritional status, pain management, and coping strategies) to be adapted throughout the patient’s cancer journey by a team consisting of different professions, for example, oncologists, surgeons, psychologists, nutritional therapists, nurses, and physiotherapists.
Translating clinical knowledge into practice: recommendations of the ESPEN board
Since 1997, ESPEN publishes guidelines and position papers in the field of clinical nutrition. Recent ESPEN guidelines for nutritional care in cancer offer a comprehensive overview and recommendations authored by 22 experts from 13 countries. 8 The guidelines are based on evidence of clinical practice, as well as on personal experience of the experts in the field and provide a set of recommendations for screening, assessment, treatment, and monitoring of malnutrition in oncological patients. In the following sections, the most important guideline recommendations and their implementation into clinical practice are presented.
Integration of nutritional management into cancer care: the role of early screening and assessment
Historically, nutritional intervention in cancer has often been associated mainly with the setting of advanced cancer stages as part of a palliative treatment regimen. This has been, and still frequently is, due to a low awareness for nutritional and metabolic problems in clinical oncology and has resulted in underdiagnosing the gradual development of malnutrition of patients during anticancer treatment.
However, nutritional therapy, if applied in a timely fashion, can contribute to maintaining or regaining a normal nutritional and functional status of the patient, which is associated with better tolerability of anticancer treatment and better clinical outcome.8,16,17,25,26,37,38,40–44
Therefore, timely screening (Figure 2, Table 1) of the nutritional status should be seen as a hallmark of care for the patient, and as good clinical practice. Early detection of nutritional needs and appropriate intervention programs are critical in cancer treatment (Figure 2). Key drivers for later complications like malnutrition and cachexia can be detected and treated at an early stage, thus helping to prevent treatment interruptions caused by impaired physical status. Such timely screening of the nutritional status can lead to better tolerability of therapy, higher completion rates of treatment cycles and an optimized treatment outcome. A number of screening tools are available; ESPEN 8 suggests using validated nutrition screening tools, for example, Nutrition Risk Screening 2002, the Malnutrition Universal Screening Tool, the Malnutrition Screening Tool, or the Mini Nutritional Assessment Short Form Revised. 69 The Patient-Generated Subjective Global Assessment has been highly recommended due to its high sensitivity, specificity and predictive value in the oncological setting,70–72 but also other validated tools may be used.
Screening for (risk of) malnutrition.

ESPEN, European Society for Clinical Nutrition and Metabolism.
Prior to chemotherapy, patients should undergo an intensive risk assessment, including disease staging, medical condition of the patient, as well as specific examination of pre-existing cachexia or further metabolic disturbances. Valid methods for determination are depicted in Table 2. CT-aided examination already used for cancer screening can be applied to identify body composition and muscle mass.30,37,38,44
Quantitative or semiquantitative assessment of relevant nutritional and metabolic parameters at present and as expected for the near future.

BMI, body mass index; ECOG, Eastern Cooperative Oncology Group.
Patients with abnormal screening should undergo a comprehensive assessment of nutritional imbalance. This includes nutritional intake, assessment of symptoms potentially interfering with food intake (e.g. anorexia, nausea, vomiting, dysphagia, dysgeusia), assessment of muscle mass, determination of physical performance, and degree of systemic inflammation. Key domains for this assessment should comprise dietary intake, body composition, physical activity, and underlying metabolic abnormalities (e.g. glucose intolerance, liver failure, kidney failure) in the patient (Table 2).
How to enable food intake and support metabolism
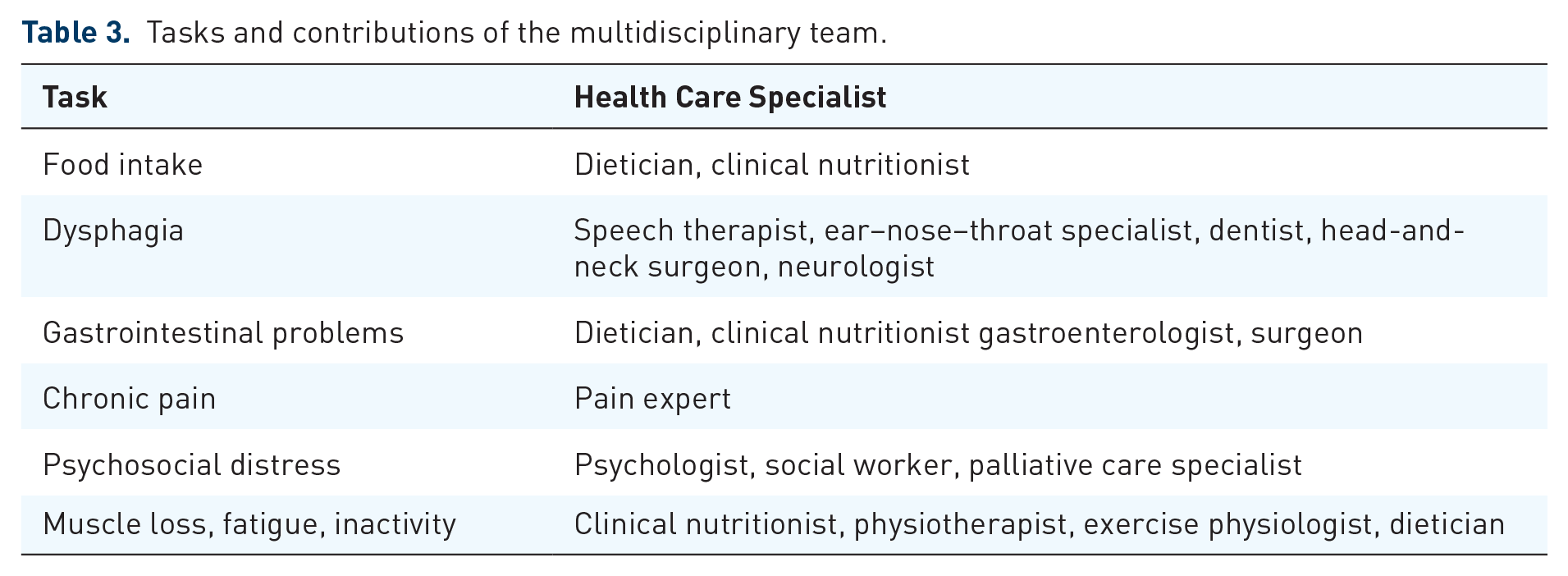
Results of the assessment procedures need to be compared with the individual aims for the patient. If the present condition deviates from these aims, interventions need to be planned to diminish or remove the observed deficits. Aims include the intake of adequate amounts of energy and nutrients, the absence of nutrition impact symptoms (e.g. nausea anorexia, dysphagia, abdominal pain, diarrhea), a functioning gastrointestinal tract, the absence of chronic pain and psychosocial distress, adequate physical activity, and the absence of systemic inflammation. Specialists of the multidisciplinary team are to be assigned to alleviating specific barriers according to their specializations (Table 3).
Tasks and contributions of the multidisciplinary team.
Nutritional goals are summarized in Table 4. In patients with malnutrition or risk of malnutrition, the use of dietary restrictions is not recommended and even considered dangerous. Theoretical arguments that nutrients would primarily benefit the tumor lack scientific evidence and thus, should not lead to interruption, decrease, or cessation of nutritional intervention in cancer patients.8,15 Energy intake should initially aim to be from 20–25 to 35 kcal/kg body weight, choosing the higher range for ambulatory, younger, underweight, and male patients, while choosing the lower range for bedridden, older, obese, and female patients. During follow up, energy provisions need to be adapted according to the nutritional status and the metabolic condition. Protein intake should be above 1 g/kg and aiming for 1.2–1.5 g/kg body weight per day.

RDA, recommended daily allowance.
Nonprotein energy may be provided by fat and carbohydrates, with each nutrient group providing a similar amount of energy. Vitamins and essential trace elements should be provided daily in doses analogous to recommended daily allowances for healthy subjects 81 either via habitual diet or in cases of inadequate food intake, as a daily oral, enteral or intravenous supplement. 8
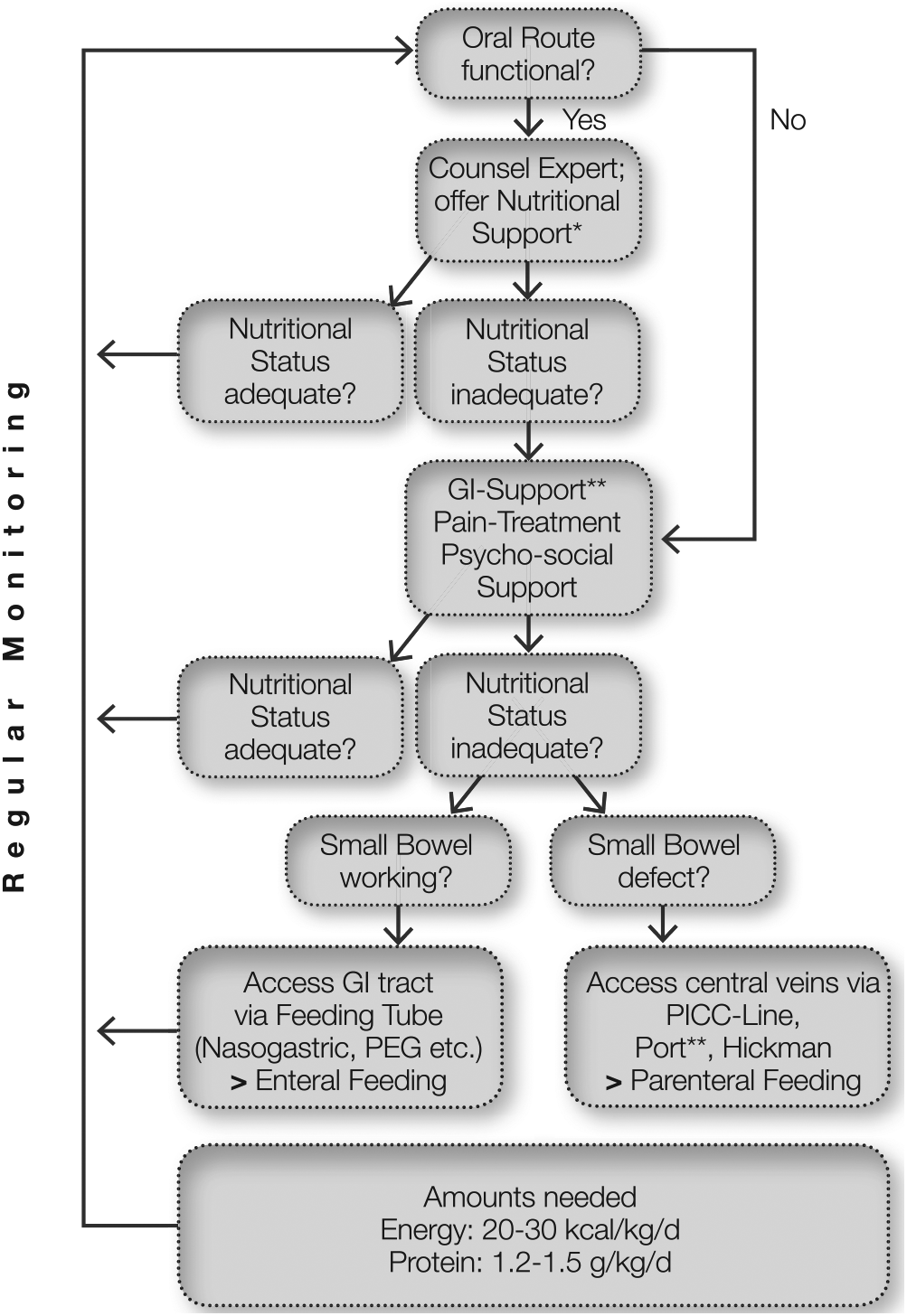
For patients with nutritional need, the route of administration should be tailored to the patient’s physical condition. Patients with inadequate food intake who are able to eat should receive adequate dietary counseling, including fortification of foods as well as ONS. If oral nutrition remains inadequate or is not feasible, EN is recommended. Should EN not be feasible or fail to improve the nutritional status of the patient, PN should be implemented, 8 either as supplemental, or, if not otherwise possible to supply adequate nutrition, as total or complete PN.
Figure 3 shows a treatment algorithm for nutritional management of malnutrition in oncological patients, including screening and assessment, as well as treatment and monitoring.
Nutritional considerations during different modes of anticancer treatments: surgery, radiotherapy, anticancer drug treatment
Nausea, anorexia, dysphagia, diarrhea and other nutritional-impact symptoms may and do occur during most anticancer treatments. Recent data show better clinical outcome in patients undergoing chemotherapy by use of standardized web-based monitoring of patient-reported symptoms. 82 Compared with usual care, the patients using the electronic symptom monitoring had a 5-month-longer survival [31.2 months (95% confidence interval (CI), 24.5–39.6) versus 26.0 months (95% CI, 22.1–30.9); p = 0.03].82,83
In all situations, the general rule is to ensure an adequate intake of energy and nutrients. This may require early placement of an enteral tube in patients with obstructing tumors of the upper gastrointestinal tract, or if radiation of the head-and-neck region or the esophagus is planned. In cases with severe dysfunction of the small bowel (e.g. mucositis induced by high-dose chemotherapy, intestinal graft versus host disease after allogeneic stem cell transplantation, short bowel syndrome after surgical resections), PN may be required and tailored to the individual need. 8 The primary goal of nutritional intervention in all these settings is to keep patients fit for, and to avoid dose reductions or interruptions of, anticancer therapy.
Role of physical activity
Muscle activity initiates essential anabolic stimuli. Increasing or maintaining muscle mass may be hampered or made impossible by inactivity. Indeed, inactivity prevents optimal incorporation and utilization of nutrients by muscle. Therefore, muscle training should accompany every nutritional intervention and should be an essential component of the parallel supportive pathway. The benefits of exercise reported in patients with cancer include increased exercise capacity, improved activity levels, and reduced fatigue,84,85 the latter of which is the most frequent and burdensome side effect of chemotherapy. Exercise has also been shown to preserve physical well-being. 86
Thus, early, continuous, and multimodal interventions with a range of approaches, including endurance training and aerobic exercises (e.g. walking, treadmill walking, stationary cycling, resistance training) is recommended, aiming at improving muscle mass and function. Oncologists should favor implementation of multimodal therapeutic approaches, including controlled physical activity for their patients, even in those complaining of asthenia and fatigue. 85
Nutrition in oncology: time for a change of perspective
Historically, treatment advances in cancer have predominantly focused on the introduction of new substances. Lately, patient-centered treatment approaches are gaining momentum, progressively including patient’s performance status, interindividual variability in drug pharmacokinetics and genetic background. This has led to an increased variety of treatment options, but results (compared with just a few years ago) in longer treatment durations for cancer patients. This may expose the patient to the prolonged risk of nutritional impairment and progressive depletion of body resources. Counteracting such depletion with nutritional interventions represents a major supportive goal in modern oncology. Still, in current clinical practice, nutritional status receives little attention. Standard evaluation focuses rather on disease-specific parameters to determine treatment procedure. Awareness is needed of how a deteriorated nutritional status or a high risk of malnutrition is an important prognostic factor for later treatment success or failure.
Incorporation of the nutritional status evaluation and monitoring should therefore be regarded as a hallmark of good clinical practice in cancer treatment. From diagnosis onward, meeting individual requirements of each cancer patient should be at the center of every treatment approach. A close collaboration of experts is the cornerstone of a state-of-the-art cancer treatment. This requires profound changes in today’s hospital infrastructure, including diagnosis and treatment criteria; however, such implementations will strongly benefit the patient, and therefore poses an ethical responsibility for treating physicians and associated clinical staff.
Footnotes
Funding
The project received funding from Fresenius Kabi Deutschland GmbH. Medical writing assistance, supported financially by Fresenius Kabi Deutschland GmbH, was provided by Medizin und Markt, a medical agency, during the preparation of this article. The sponsor had no role in the writing process of the publication. The authors are fully responsible for all content and editorial decisions, were involved at all stages of manuscript development and have compiled and approved the final version.
Conflict of interest statement
The authors declare that there is no conflict of interest.