
Abstract
There are questions surrounding the real-world effectiveness of chemotherapeutic treatments for pancreatic ductal adenocarcinoma. This literature review compared the clinical characteristics and outcomes of available real-world evidence (RWE) for liposomal irinotecan in combination with 5-fluorouracil (5-FU) and leucovorin (LV), a treatment regimen indicated for patients with metastatic pancreatic ductal adenocarcinoma (mPDAC) who previously progressed on gemcitabine-based therapy.
A targeted literature search was conducted in the PubMed Central® and Embase® databases to identify available RWE regarding patients with mPDAC receiving liposomal irinotecan published within the last 5 years (January 2014–September 2019). Data were extracted for prior lines of therapy, performance status, overall survival (OS), progression-free survival (PFS), duration of exposure, and adverse events.
Six studies met inclusion criteria. A comparison of baseline patient characteristics and results with the included evidence reveals a clinically fragile, real-world patient population in terms of age (range: 61–68), prior lines of therapy with 34–61% of patients receiving ⩾2 lines of lines of prior therapy and performance status [49.8–100% of patients with Eastern Cooperative Oncology Group (ECOG) 0–1]. Studies observed wide OS (range: 5.3–9.4 months) and similar PFS (range: 2.3–4.1 months), with two studies measuring duration of exposure (7.3 weeks, 3.1 months). Patients analyzed by RWE studies tended to be older with significant disease progression, poor performance status, and more heavily pretreated compared with the phase III registrational trial (NAPOLI-1). Despite this, patients treated with liposomal irinotecan + 5-FU/LV therapy had similar outcomes as those in NAPOLI-1.
Background
Pancreatic ductal adenocarcinoma (PDAC), an exocrine subtype pancreatic malignancy affecting the pancreatic ductal epithelium, comprises approximately 85% of new pancreatic cancer cases in the United States (US) and is one of the most lethal cancers encountered.1–3 PDAC is characterized by diagnosis in the locally advanced or metastatic stages, with rapidly replicating cancer cells resulting in metastatic propensity and resistance to cytotoxic treatment due, in part, to a very dense stroma.1,2 PDAC tends to be diagnosed in later stages due to absence of symptomatology in the early stages. Late diagnosis generally eliminates the possibility for curative surgical intervention. The intrinsic cytotoxic resistance of the disease renders many chemotherapeutic treatments ineffective. 3
The combination of gemcitabine (gem) and nano-particle albumin bound paclitaxel (nab-pac) was approved by the US Food and Drug Administration (FDA) for first-line treatment of metastatic PDAC (mPDAC) in 2013, and other combinations, though not indicated for mPDAC, have shown comparable efficacy in clinical studies. 2 Clearly, patients with mPDAC could benefit from second line treatment options, but drug discovery has been challenging and incremental, with 12 phase III trial failures since 2015. 4 More recently, liposomal irinotecan (Onivyde®, historical names include nal-IRI, MM-398, or PEP02), an intravenous liposomal formulation that encapsulates the topoisomerase 1 inhibitor irinotecan in a lipid-bilayer vesicle, has emerged as the only second-line/post-gemcitabine treatment in mPDAC that is NCCN Category I, ASCO Preferred, and FDA-approved.5–7 On the basis of results from the NAPOLI-1 study, a pivotal phase III registrational trial, liposomal irinotecan in combination with 5-fluorouracil (5-FU) and leucovorin (LV) (liposomal irinotecan + 5-FU/LV) is indicated in the treatment of mPDAC as a second-line therapy following disease progression with gem-based treatment. 8
In the NAPOLI-1 study, combination therapy with liposomal irinotecan + 5-FU/LV significantly increased median overall survival (OS; primary endpoint) and progression-free survival (PFS; secondary endpoint) compared with 5-FU/LV alone. Median OS was 6.1 months [95% confidence interval (CI): 4.8–8.9] in patients randomized to liposomal irinotecan + 5-FU/LV, compared with 4.2 months (95% CI: 3.3–5.3) in patients randomized to 5-FU/LV alone [unstratified hazard ratio (HR): 0.67; 95% CI: 0.49–0.92; p = 0.012]. Median PFS was 3.1 months (95% CI: 2.7–4.2) in patients in the liposomal irinotecan + 5-FU/LV arm, compared with 1.5 months (95% CI: 1.4–1.8) in patients in the 5-FU/LV arm (unstratified HR: 0.56; 95% CI: 0.41–0.75; p = 0.0001). Patients assigned to liposomal irinotecan + 5-FU/LV had a median age of 63 years [interquartile range (IQR): 57–70], 91% had a performance score equivalent to Eastern Cooperative Oncology Group (ECOG) 0–1, and 34% had two or more previous lines of therapy. Median duration of exposure (DOE) for the patients treated with liposomal irinotecan + 5-FU/LV arm was 8.7 weeks (IQR, 5.4–22.0). 9
The narrow eligibility criteria for patients enrolled in clinical trials can mean that the studied population is very different from the population treated in normal life, which can impact patient outcomes. This review compared patient demographics and clinical outcomes from existing real-world evidence (RWE) that assessed mPDAC patients treated with liposomal irinotecan + 5-FU/LV.
Methods
A targeted search of PubMed Central® and Embase® databases for available RWE in pancreatic adenocarcinoma patients receiving liposomal irinotecan was conducted by two experienced reviewers in late September 2019. The search strategy contained the following terms and their associated MeSH® and Emtree® terms: irinotecan, nanoliposomal, nal-IRI, Onivyde®, database, registry, cohort, cohort analysis, retrospective, pragmatic, and pragmatic trial. The full search string can be found in Supplemental Table S1. Publications meeting the following criteria were included: patient population with mPDAC, use of liposomal irinotecan + 5-FU/LV, RWE study designs (database studies, registries, cohort analyses, and pragmatic clinical trials), study populations from January 2014 to September 2019. Manuscripts and congress materials were eligible for inclusion in the targeted review. Studies of primary indications other than mPDAC, non-real-world data or study designs (e.g., randomized clinical trial, preclinical, or formulation studies), pre-clinical studies, and studies published before 2014 were excluded.
A descriptive comparison of RWE studies was performed on study population demographics, treatment information, and outcome measures. The following data were extracted for comparison: median age at treatment onset (years), number of prior lines of therapy, duration of therapy exposure (DOE, weeks), adverse events (AEs)/toxicity experienced (%), ECOG performance status, OS (months), and PFS (months). Statistical analysis information reported for each outcome measure was extracted. 9
Results
The search strategy yielded 81 studies, 75 of which were excluded according to the criteria presented in Figure 1. The remaining six publications – Glassman et al., 10 Barzi et al., 11 Ahn et al., 12 Tossey et al., 13 Kieler et al., 14 and Yoo et al. 15 – were included in this analysis. Two studies, Barzi et al. 11 and Ahn et al., 12 utilized the same data source, time horizon, and the same patient population. They differed in the outcomes they analyzed, with Barzi et al. primarily reporting survival outcomes while Ahn et al. described dose modifications.11,12 These two studies were combined for extraction in this review. Tables 1–3 present comparisons of baseline patient characteristics, treatment efficacy results, and safety endpoints from the six studies, respectively.

Integrated database flow diagram.
Selected baseline patient characteristics of RWE studies.

ECOG, Eastern Cooperative Oncology Group; IQR, interquartile range; RWE, real-world evidence.
Selected treatment effectiveness results of RWE studies.
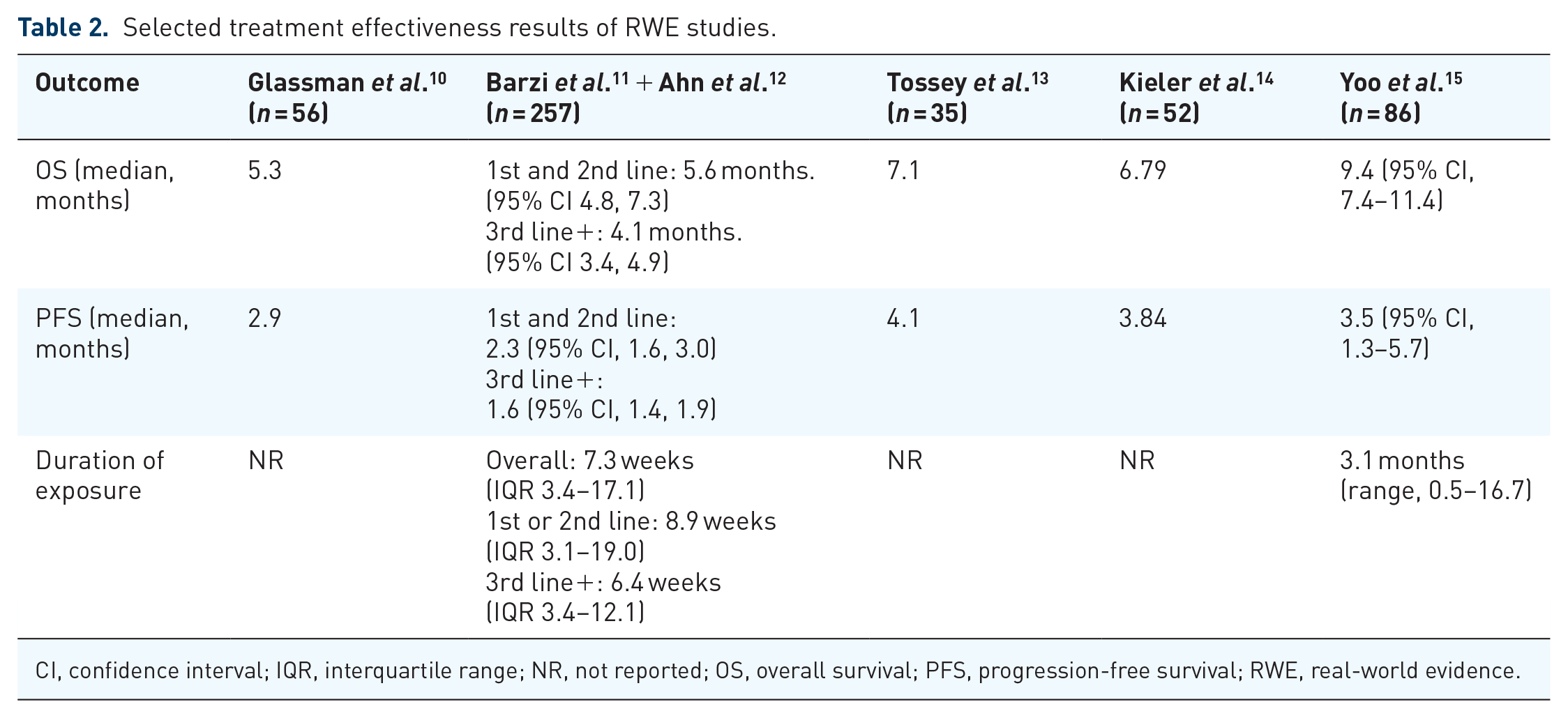
CI, confidence interval; IQR, interquartile range; NR, not reported; OS, overall survival; PFS, progression-free survival; RWE, real-world evidence.
Adverse events of RWE study results.
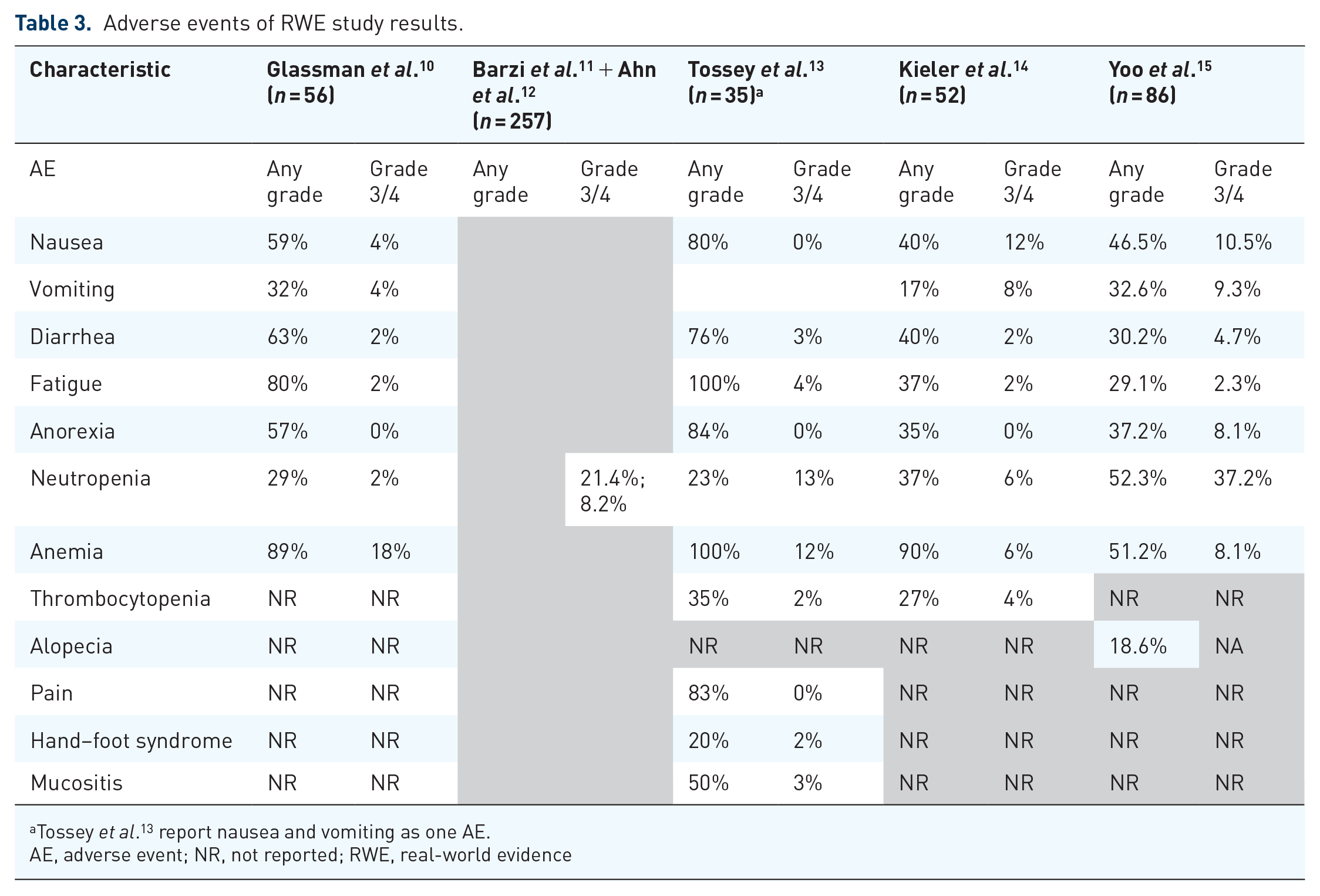
Tossey et al. 13 report nausea and vomiting as one AE.
AE, adverse event; NR, not reported; RWE, real-world evidence
Eligible studies
Glassman et al. was a retrospective chart review of patients with mPDAC who underwent liposomal irinotecan + 5-FU/LV treatment between October 2015 and June 2017. 10 The review took place at Memorial Sloan Kettering Cancer Center (MSKCC) and its regional network. MSKCC’s electronic medical record (EMR) database allowed for the collection of: performance status (ECOG scale), date of diagnosis, date of advanced disease diagnosis and carbohydrate antigen 19–9 (CA 19–9) level at baseline, prior treatment details and duration, liposomal irinotecan + 5-FU/LV starting dose, liposomal irinotecan + 5-FU/LV dose reductions, liposomal irinotecan + 5-FU/LV treatment duration, AE, PFS, and OS. Prior lines of therapy in Glassman et al. referred to chemotherapies received prior to initiating liposomal irinotecan combination therapy. 10 The study also integrated germline and tumor genomics (methodology described in [ClinicalTrials.gov identifier: NCT01775072]) in order to analyze relationships between genotypes and outcomes. All adverse events were noted and graded according to NCI-CTCAE V4.0. 10
Barzi et al. and Ahn et al. were retrospective observational studies that, between them, described real-world characteristics, dose intensity at 6 weeks, dose modification, reasons for treatment discontinuation, and outcomes of patients with mPDAC on liposomal irinotecanliposomal irinotecan + 5-FU/LV treatment.11,12 The studies utilized the Flatiron Health database, a nationwide longitudinal, demographically and geographically diverse database derived from de-identified electronic health record (EHR) data for more than 2 million cancer patients treated at over 265 diverse cancer clinics (~800 sites of care). De-identified patient-level data included structured and unstructured data, curated via technology-enabled abstraction. Patients were treated from 1 January 2014 to 31 August 2017; baseline characteristics, time-to-treatment failure (TTF), OS, and AE data were analyzed. Prior lines of therapy were measured by providing the therapy line number at which liposomal irinotecan combination therapy was initiated in the metastatic setting.11,12
Tossey et al. was a single-center, retrospective, cohort study that analyzed RWE available for patients with mPDAC aged 18–89 years and treated with liposomal irinotecan + 5-FU/LV therapy at The Ohio State University Comprehensive Cancer Center, James Cancer Hospital, and Solove Research Institute from October 2015 to August 2018. 13 PFS, defined as the time from the first dose of chemotherapy to disease progression or death, was the primary outcome of the study. Secondary outcomes were TTF, OS, frequency of dose reductions or treatment delays, and frequency of AEs. Prior lines of therapy were described as the number of systemic therapies received prior to the initiation of liposomal irinotecan combination therapy. Eligibility criteria included previous gem-based therapy, either as the first-line treatment of unresectable or metastatic disease, or as either neoadjuvant or adjuvant treatment if within the preceding 6 months. 13
Kieler et al. was a single-center, retrospective, observational cohort study of patients with PDAC that was locally or metastasized at the Medical University of Vienna between January 2012 and August 2018 treated with one or more doses of liposomal irinotecan + 5-FU/LV. 14 Patient characteristics, including ECOG performance status, were described. The outcomes analyzed included OS, PFS, number of treatments prior to initiating liposomal irinotecan + 5-FU/LV, and all treatment related AEs, graded per the CTCAE V4.0. 14
Yoo et al. was a multicenter, retrospective, observational cohort study conducted by the Korean Cancer Study Group of patients with mPDAC who entered into the Liposomal Irinotecan Managed Access Program in Korea between January 2017 and April 2018. 15 Ten institutions participated in the study. Patients were eligible for inclusion if they had experienced prior progression on gem-based therapy. Patient characteristics, ECOG performance status, duration of treatment, response rate, OS, PFS, and AEs graded using CTCAE V4.03 were assessed. 15
Patient characteristics
A total of 56 patients (median age: 68 years) were included in the Glassman et al. study. 10 Most patients had metastatic disease at liposomal irinotecan + 5-FU/LV treatment onset (96%), and were previously exposed to ⩾2 lines of advanced disease therapy (58%). Barzi et al. and Ahn et al. included 257 patients (median age: 68 years) with mPDAC treated with a liposomal irinotecan based regimen, of whom 43.6% had at least two prior lines of therapy in the metastatic setting.11,12 Of the 75 patients with locally advanced or metastatic PDAC in Tossey et al., 35 patients (median age: 63 years) received liposomal irinotecan + 5-FU/LV treatment. 13 Kieler et al. included 52 patients (median age: 64.6 years) with 40% of patients who initiated liposomal irinotecan after ⩾2 prior lines of therapy. 14 Yoo et al. identified 86 patients (median age: 61 years) with mPDAC. 15 Of these patients, 61% had experienced ⩾2 lines of therapy prior to liposomal irinotecan initiation. Baseline patient characteristics, including age, number of prior lines of therapy, and performance status were similar across included patient populations (Table 1). In aggregate, 43.7% of patients had experienced ⩾2 prior lines of therapy and 69.1% of patients had an ECOG score of 0–1.
Overall survival
The OS reported in Glassman et al. for all patients was 5.3 months. Patients who initiated liposomal irinotecan in earlier lines of therapy experienced improved survival relative to later lines. 10 Second line patients had a median OS of 8.4 months while patients starting liposomal irinotecan in their fourth line had a median OS of 4.5 months, suggesting that the lower survival rates in this group may be related to initiating liposomal irinotecan + 5-FU/LV later in the disease course. Observed statistically significant relationships between earlier use of liposomal irinotecan treatment and PFS (p = 0.0031) and OS (p = 0.0002) support this. Similarly, median OS in Barzi et al. and Ahn et al. were improved among patients initiating liposomal irinotecan + 5-FU/LV treatment in earlier lines of therapy.11,12 Patients initiating liposomal irinotecan + 5-FU/LV as a first- or second-line treatment had a median OS of 5.6 months (95% CI, 4.8–7.3) while patients who initiated this regimen as a third-line or later treatment had a median OS of 4.1 months (95% CI, 3.4–4.9). Median OS in the liposomal irinotecan group reported by Tossey et al. was 7.1 months. 13 The median OS values reported by Kieler et al. and Yoo et al. were 6.79 months and 9.4 (95% CI, 7.4–11.4) months, respectively.14,15
Progression-free survival
Glassman et al. reported a median PFS of 2.9 months for the entire cohort. 10 Barzi et al. and Ahn et al. reported time until treatment failure (TTF).11,12 Patients who utilized liposomal irinotecan + 5-FU/LV as a first or second therapy had a TTF of 2.3 months (95% CI, 1.6–3.0) while patients in third and later lines had a TTF of 1.6 months (95% CI, 1.4–1.9). Median PFS in the liposomal irinotecan group reported by Tossey et al. was 4.1 months. 13 Kieler et al. observed a median PFS of 3.84 months. 14 Additionally, the line of therapy in which liposomal irinotecan was given was a significant predictor of PFS (second line: 4.49 months vs third or later lines: 3 months, p = 0.0275). The median PFS reported by Yoo et al. was 3.5 months (95% CI, 1.3–5.7). 15
Duration of exposure
The median DOE for the population in Barzi et al. and Ahn et al. was 7.3 weeks (IQR, 3.4–17.1) (Table 2).11,12 Patients using liposomal irinotecan as a first- or second- line treatment had a median DOE of 8.9 weeks (IQR, 3.1–19.0) while patients using this regimen as a third-line or greater treatment had a median DOE of 6.4 (IQR 3.4–12.1) weeks. The median DOE among patients included in Yoo et al. was 3.1 months (range, 0.5–16.7). 15 Glassman et al., Tossey et al., and Kieler et al. did not report DOE.10,13,14
Adverse events/toxicity
In Glassman et al., several patients experienced grade 3 or 4 AEs including nausea (4%), vomiting (4%), diarrhea (2%), fatigue (2%), neutropenia (2%), and anemia (18%). 10 Barzi et al. and Ahn et al. only reported grade 3 and 4 neutropenia among 21.4 and 8.2% of the population, respectively.11,12 Barzi et al. 11 and Ahn et al. 12 did not describe any other specific AEs. Tossey et al. 13 observed diarrhea (3%), fatigue (4%), stomatitis (3%), neutropenia (13%), thrombocytopenia (2%), anemia (12%), and hand–foot syndrome (2%). Kieler et al. reported that patients experienced the following grade 3 and 4 AEs: nausea (12%), vomiting (8%), diarrhea (2%), fatigue (2%), thrombocytopenia (4%), neutropenia (6%), and anemia (6%). 14 Yoo et al. reported on a similar set of grade 3 and 4 AEs and observed the following: nausea (10.5%), vomiting (9.3%), diarrhea (4.7%), fatigue (2.3%), neutropenia (37.2%), and anemia (8.1%). 15
The frequencies of AEs observed are summarized in Table 3.
Discussion
The RWE in mPDAC reviewed here demonstrates that patients tend to be older, have experienced more lines of therapy (47.3% with two or more prior lines), with poor performance status (69.1% with ECOG 0-1) in practice settings, compared with prior clinical trial research (NAPOLI-1, [ClinicalTrials.gov identifier: NCT01494506]). 9 Only one of the included studies had a median age below that of the patients treated with liposomal irinotecan + 5-FU/LV in the NAPOLI-1 trial. Additionally, patients tended to be heavily pre-treated, with some patients receiving three or more chemotherapy regimens before being treated with liposomal irinotecan combination therapy. Despite evidence of clinical fragility in this real-world patient population, liposomal irinotecan combination therapy had a similar effectiveness in terms of OS and PFS as reported in NAPOLI-1.
AEs in NAPOLI-1 were identified in 56 (48%) patients assigned to the liposomal irinotecan + 5-FU/LV arm. AEs that resulted in dose reduction occurred in 39 (33%) patients in the liposomal irinotecan + 5-FU/LV arm. The most common AEs that precipitated dose reduction were neutropenia (27%), diarrhea (13%), vomiting (11%), and fatigue (14%). Similar distributions of AEs were observed in analyzed RWE, suggesting that the safety profile of liposomal irinotecan combination is comparable across clinical practice settings.
This comparison of available RWE for patients with mPDAC undergoing liposomal irinotecan + 5-FU/LV treatment indicates that outcomes of patients treated with liposomal irinotecan + 5-FU/LV, including survival and progression outcomes, are consistent across multiple real-world settings and are similar to those reported in NAPOLI-1. Safety profile and frequencies of AEs reported in the observed real-world studies were comparable. Taken together, the RWE suggests that liposomal irinotecan + 5-FU/LV is effective in routine clinical practice settings, with a similar adverse event profile to a randomized controlled trial, while being administered to clinically fragile populations. These characteristics likely define the real-world status of mPDAC patients outside of clinical trial settings.
RWE has several notable limitations. Data elements may be missing or incorrect due to entry error. Moreover, the characteristics of each RWE study should be considered. Glassman et al., Tossey et al., and Kieler et al. were relatively small, single-center studies with limited generalizability.10,13,14 Despite this, their results were comparable with the analysis of a national cancer database in Barzi et al. and Ahn et al.11,12 Yoo et al. reported the highest median OS of 9.4 months, 15 which mirrors the median OS of 8.9 months for patients from the NAPOLI-1 trial treated at Asian centers. 16 Finally, limited studies are published employing RWE to investigate liposomal irinotecan + 5-FU/LV utilization. One strength of RWE is that it reflects current real-world treatment utilization and decision making across clinical practice settings, regardless of formal labeling recommendations. RWE may provide a more direct understanding of current patient management practices and outcomes. Stronger insights may be gleaned if a more robust evidence base, both in terms of publication number and quality, is available.
Conclusion
There is a pressing need for more effective chemotherapeutic treatments for mPDAC. RWE provides a supplemental source of information for more comprehensive understanding of patient outcomes for this less controlled patient population in real-world clinical practice settings. The RWE studies examined here provide evidence supports the real-world effectiveness of liposomal irinotecan treatment across different settings of care and patient types. Unlike in randomized controlled trials, in routine clinical practice, patients tended to be older with more prior lines of therapy and poor performance status. Additionally, some real-world patients were heavily pre-treated before being treated with liposomal irinotecan combination therapy. Despite this, patients treated with liposomal irinotecan combination therapy had similar OS, PFS, and AE outcomes as those in NAPOLI-1.
Supplemental Material
Supplemental_Table_1 – Supplemental material for Comparing real-world evidence among patients with metastatic pancreatic ductal adenocarcinoma treated with liposomal irinotecan
Supplemental material, Supplemental_Table_1 for Comparing real-world evidence among patients with metastatic pancreatic ductal adenocarcinoma treated with liposomal irinotecan by Jim Koeller, Andy Surinach, Steven R. Arikian, Marko Zivkovic, Patrick Janeczko, Paul Cockrum and George Kim in Therapeutic Advances in Medical Oncology
Footnotes
Acknowledgements
Conflict of interest statement
PC is an employee of Ipsen. AS, SRA, MZ, PJ are employees of Genesis Research and report an advisory/consulting role with Ipsen. JK reports a consulting advisory/consulting role with Ipsen, Coherus, Daiichi, and Tocagen. GK reports no conflict of interest.
Funding
The authors disclosed receipt of the following financial support for the research, authorship, and/or publication of this article: This study was sponsored by Ipsen Biopharmaceuticals, Inc. The sponsor was involved in the design of the study, analysis, and interpretation as well as final approval of the manuscript.
Supplemental material
Supplemental material for this article is available online.
References
Supplementary Material
Please find the following supplemental material available below.
For Open Access articles published under a Creative Commons License, all supplemental material carries the same license as the article it is associated with.
For non-Open Access articles published, all supplemental material carries a non-exclusive license, and permission requests for re-use of supplemental material or any part of supplemental material shall be sent directly to the copyright owner as specified in the copyright notice associated with the article.