
Abstract
Objective
This study was performed to investigate the physical performance parameters, including lower extremity function parameters, that may be risk factors for falls in patients with chronic heart failure.
Methods
Seventy patients with stable chronic heart failure were included in this retrospective cross-sectional study. The five-repetition sit-to-stand test (5STS) time, Controlling Nutritional Status (CONUT) score, and number of drugs were assessed.
Results
Simple linear regression analysis revealed that the 5STS time was positively correlated with age, the CONUT score, and the number of drugs but was negatively associated with the handgrip force, quadriceps force, and quadriceps muscle thickness. Multiple linear regression analysis showed a significant association between the 5STS time and the CONUT score, quadriceps force, and number of drugs.
Conclusion
The muscle strength, nutritional status, and number of drugs should be evaluated to prevent lower extremity weakness in patients with stable chronic heart failure.
Keywords
Introduction
Heart failure is one of the most common diseases of the cardiovascular system. The number of patients with heart failure has rapidly increased to an estimated 26 million patients worldwide. 1 In particular, the incidence of chronic heart failure (CHF) is increasing because of the aging of the population, while the pathology of CHF has become complicated. Recent studies have revealed many factors related to the prognosis of CHF, including sarcopenia, frailty, malnutrition, and polypharmacy; among these, frailty is associated with an increased risk of falls.2–6 Clinically, fracture is often suspected when a patient with CHF falls. Gerber et al. 7 reported that the fracture risk was higher in patients with than without CHF. Moreover, Cullen et al. 8 reported that CHF is a common and serious perioperative condition in patients with hip fracture. Therefore, special attention is required to prevent falls in patients with CHF. Ward et al. 9 reported that a slow sit-to-stand time as a lower extremity function test in the Short Physical Performance Battery (SPPB) was related to the cumulative incidence rate of falling. However, the factors of CHF that are related to the risk of falling remain unclear. The present study was performed to investigate physical performance parameters, including lower extremity function parameters, as potential risk factors of falls in patients with CHF.
Methods
Study design and patient population
This retrospective cross-sectional study involved patients with stable CHF who were admitted to the Nagasaki University Hospital for educational purposes or for examination of their CHF status from September 2015 to December 2016. The patients had been diagnosed with CHF according to the Framingham Heart Study criteria. 10 Stable CHF was defined as independent ambulation with no change in treatment or medication during the last several months and admission. The exclusion criteria were poor physical function, such as musculoskeletal or neurological disorders, and acute exacerbation of CHF due to comorbidities. We collected all patients’ information from their medical records. Diabetes was defined as a glycated hemoglobin concentration of >6.5%. 11 Kidney disease was defined as an estimated glomerular filtration rate of <60 mL/min/1.73 m2, calculated using the Modification of Diet in Renal Disease formula. 12 Anemia was defined according to the World Health Organization criteria (hemoglobin concentration of <13 g/dL in men and <12 g/dL in women). 13
Measurement of physical function
The handgrip force (HGF), isometric quadriceps force (QF), quadriceps muscle thickness (QT), and five-repetition sit-to-stand test (5STS) time were evaluated by a physiotherapist. The HGF was assessed in the dominant hand using a dynamometer (T.K.K.5401; Takei Kiki Kogyo, Niigata, Japan) in a standing position with the elbow extended and the arms fixed to the body. 14 The highest value (kg) of three attempts was recorded. The QF was evaluated as the peak force that developed during a maximal isometric knee extension maneuver using a handheld dynamometer with a fixing belt (µTas F-1; Anima Corporation, Tokyo, Japan) with a standard protocol. 15 It was tested on the dominant side with the patient in a sitting position with the hip and knee joints flexed at approximately 90°. The highest value (kg) of at least three maneuvers was recorded and expressed in kilograms. The QT was measured 15 cm above the patella by B-mode ultrasonography (ProSound 2; Hitachi, Tokyo, Japan) with the lower limbs extended in a sitting position. 16 All images and data were stored on a personal computer. The same physiotherapist (Y.M.) conducted all the measurements to reduce the risk of bias among examiners. 17 The 5STS time, which was the main outcome, was measured with the patient’s arms crossed over their chest, and the time required for the patient to stand up from a chair (45 cm in height) five times as quickly as possible without using their arms was measured using a stopwatch. The 5STS time was then assigned a categorical score ranging from 0 to 12 according to the SPPB, and sarcopenia was defined by a cutoff score of >9.5.18,19
Nutritional assessment
We calculated the Controlling Nutritional Status (CONUT) score, which was developed as a simple and cost-effective screening tool for early detection of a poor nutritional status by the serum albumin concentration, total cholesterol concentration, and lymphocyte count. 20 The CONUT score ranges from 0 to 12, and malnutrition is categorized as follows: none, 0–1; light, 2–4; moderate, 5–8; and severe, 9–12.
Classification of drugs
All drugs orally administered at admission were evaluated, and the numbers of different kinds of drugs were counted by pharmacist.
Cardiac function
Cardiac systolic function (left ventricular ejection fraction) and diastolic function (e’) were evaluated by echocardiography.
Statistical analysis
A regression analysis was performed to identify the clinical variables associated with the result of the 5STS of the SPPB. Candidate factors were selected according to a literature review, clinical expertise, and their significant contributions to the outcome of the simple linear regression analysis (p < 0.05). We selected five variables in the multiple linear regression models: three demographic parameters [age, body mass index (BMI), and number of drugs administered], physical function (QF), and the nutritional status (CONUT score). The physical function variables (QF, QT, and HGF) were significantly correlated, and we selected QF to avoid multicollinearity. These models were applied to assess whether these variables were independent factors of the 5STS time for patients with CHF. All analyses were performed using JMP® Pro 13 Version 13.0.0 (SAS Institute Inc., Cary, NC, USA). Data are expressed as median (25th–75th percentile) or percentage, as appropriate. The level of significance was <0.05 for all tests.
Ethics
This study was approved by the Human Ethics Review Committee of Nagasaki University Hospital (reference number 15111603). Informed consent was obtained in the form of an opt-out option on the website. Those who rejected were excluded. The patients’ information was anonymized and de-identified and stored on a lockable shelf. Identification and clinical data were stored separately.
Results
Patients’ characteristics (Tables 1–3)
Seventy patients with stable CHF (37 men; mean age, 73.5 years) were included in the present study (Figure 1). Among these patients, the most underlying cardiovascular disease of CHF was valvular disease (82.9% of patients). The New York Heart Association (NYHA) class was I, II, III, and IV in 17 (24%), 46 (66%), 7 (10%), and 0 (0%) patients, respectively.
Characteristics of patients with chronic heart failure.

Data are presented as median (interquartile range), n (%), or n.
BMI, body mass index; SBP, systolic blood pressure; LVEF, left ventricular ejection fraction; HFrEF, heart failure with reduced ejection fraction; HFmrEF, heart failure with mid-range ejection fraction; HFpEF, heart failure with preserved ejection fraction; COPD, chronic obstructive pulmonary disease; NYHA, New York Heart Association; ACE, angiotensin-converting enzyme; ARB: angiotensin II receptor blocker.
Blood test results.
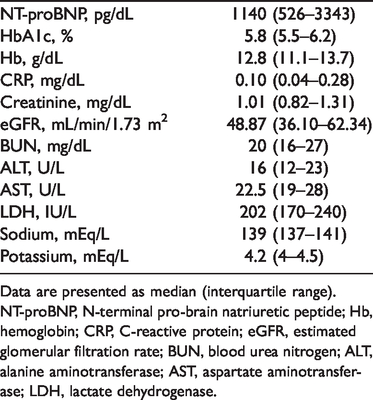
Data are presented as median (interquartile range).
NT-proBNP, N-terminal pro-brain natriuretic peptide; Hb, hemoglobin; CRP, C-reactive protein; eGFR, estimated glomerular filtration rate; BUN, blood urea nitrogen; ALT, alanine aminotransferase; AST, aspartate aminotransferase; LDH, lactate dehydrogenase.
Physical function and nutritional status parameters.
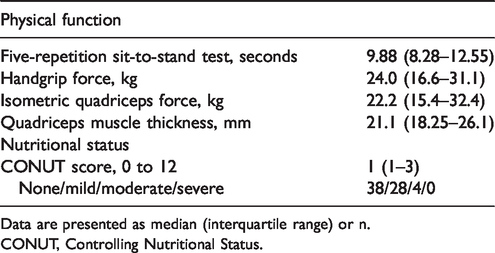
Data are presented as median (interquartile range) or n.
CONUT, Controlling Nutritional Status.

Flow chart.
Almost half of the patients (54.3%) had a normal nutritional status. The malnutrition status was mild in 40.0% and moderate in 5.7% of patients.
The median and maximum numbers of drugs, including both CHF and non-CHF medications, were 9 and 19, respectively. Among CHF drugs, loop diuretics were prescribed most frequently (71% of patients), while beta blockers and angiotensin-converting enzyme inhibitors or angiotensin II receptor blockers where prescribed for around 60% of patients, followed by spironolactone (38.9% of patients) and tolvaptan (11.0% of patients).
Non-CHF medications were prescribed more often than CHF medications (median [interquartile range], 3 [2–4] and 6 [3–9], respectively). Most non-CHF medications were digestive drugs followed by sleeping drugs, antidepressants, and tranquilizers.
Thirteen patients (18.6%) in this study had sarcopenia as defined by the SPPB.
Most patients had a perfect score for each item; the only item with a minimum score of 0 was the 5STS time.
Associations between 5STS time and variables in univariate and multivariate analyses
In the simple linear regression analysis, the 5STS time was positively correlated with age (ß = 0.10, p < 0.001), the CONUT score (ß = 2.53, p < 0.001), and the number of drugs (ß = 0.71, p < 0.001), whereas it was negatively correlated with the HGF (ß = −0.25, p = 0.02), QF (ß = −0.30, p < 0.001), and QT (ß = −0.36, p = 0.02). Vital signs (blood pressure and heart rate), cardiac function (LVEF, eʹ, and NYHA class), comorbidities (each comorbidity and number), and laboratory data were not significantly associated with the 5STS time (Table 4).
Single regression model results of five-repetition sit-to-stand test.

BMI, body mass index; SBP, systolic blood pressure; LVEF, left ventricular ejection fraction; NYHA, New York Heart Association; COPD, chronic obstructive pulmonary disease; NT-proBNP, N-terminal pro-brain natriuretic peptide; CRP, C-reactive protein; BUN, blood urea nitrogen; ALT, alanine aminotransferase; AST, aspartate aminotransferase; LDH, lactate dehydrogenase; CONUT, Controlling Nutritional Status.
In the multiple linear regression analysis adjusted for age and BMI, there was a significant association between the 5STS time and the CONUT score (ß = 1.81, p < 0.01), QF (ß = −0.20, p = 0.03), and number of drugs (ß = 0.47, p = 0.04) (Table 5).
Results from the multiple regression analysis of the time of five-repetition sit-to-stand.

This model had a coefficient of multiple determination (R2) of 0.36.
BMI, body mass index; CONUT, Controlling Nutritional Status.
Discussion
The present study of patients with stable CHF demonstrated two main findings. First, the 5STS time was positively correlated with age, the CONUT score, and the number of drugs and negatively correlated with muscle strength and muscle volume in the single regression analysis. Second, in the multiple linear regression analysis adjusted for age and BMI, the 5STS time was positively correlated with the CONUT score and number of drugs and negatively correlated with the QF.
Sit-to-stand movement is divided into three phases: the first phase, in which the upper body is brought forward; the second phase, in which the buttocks are removed from the chair; and the third phase, in which the upper body is brought upright and the knees are extended. The quadriceps muscle acts to extend the knee joint, and the hamstrings and gluteus maximus muscle act to extend the hip joint, pushing the center of gravity upward and simultaneously adjusting the posture to the upright position along with the erector spinae muscle and gastrocnemius muscle. Naturally, a quickly performed sit-to-stand from the chair requires lower limb muscle kinetic strength. Jones et al. 21 reported stronger associations between the 5STS time and QF. We investigated only the QF among lower limb muscle strengths, and our finding were compatible with their results. Moreover, the 5STS time has been reported to be a predictor of recurrent falls due to loss of body balance in healthy community-living subjects aged ≥65 years. 22
In a review of risk factors for falls based on the American Geriatrics Society guideline, muscle weakness was the strongest risk factor (odds ratio [OR], 4.4) followed by a history of falls (OR, 3.0), gait deficit (OR, 2.9), impaired activities of daily living (OR, 2.3), and age (OR, 1.7). 23 Taken together, other factors besides muscle weakness may be related to falls.
No reports have addressed the relationship between the nutritional status and the 5STS time or risk of falls in patients with CHF. Although the detailed causal relationship between the nutritional status and physical performance is unknown, some studies have demonstrated that physical performance was improved by administering nutritional support.24–26 Among them, Lombardi et al. 26 reported that supplementation with essential and semi-essential amino acids for 3 months in patients with stable CHF improved exercise tolerance. Thus, the nutritional status may be important for fall prevention via improvement in the exercise tolerance of patients with CHF.
According to a systematic review on how a combination of exercise and dietary supplementation affects muscle mass and muscle function in patients with sarcopenia, increased muscle strength was noted in 82.8% of studies (29 of 35 randomized controlled trials [RCTs]) following exercise intervention. Dietary supplementation showed additional benefits in only a few studies (8 [22.8%] of 35 RCTs), and most studies showed an increase in physical performance following exercise intervention (26 [92.8%] of 28 RCTs) according to the SPPB. 27 Thus, in patients with sarcopenia, exercise intervention seems to be more effective than nutritional intervention. However, no reports have focused on the effect of nutritional intervention on the 5STS time, especially in patients without sarcopenia.
Our study included non-elderly patients who were able to walk independently. Only 18% of patients had sarcopenia, and almost half of the patients had a normal nutritional status, while the remaining patients had only mild malnutrition. Thus, even in patients with stable CHF without severe malnutrition, the nutritional status is related to decreased lower extremity function.
The present study included patients with mild stable CHF (many patients had NYHA class I and II CHF), a preserved ejection fraction, and a reduced ejection fraction. Thus, there was no significant relationship of the 5STS time with the ejection fraction or NYHA class in the present study. Additionally, we found no association between the number of drugs administered and the 5STS time. Kojima et al. 28 reported that the number of drugs was significantly associated with falls in their multiple logistic regression analysis of geriatric outpatients. A systematic review of falls in patients with CHF showed that benzodiazepines and digoxin were medications that increased the risk of falls and that patients who had a reduced gait speed and poor balance were at a greater risk of falls. 29 In this study, we were unable to evaluate the influence of specific drugs on the 5STS time. However, we found a positive relationship between the number of drugs and the 5STS time. Thus, further studies are needed to identify the relationship between the type of drugs and the 5STS time in patients with stable CHF.
The population in this study is a special group because the most common cause of heart failure was valvular disease. Our patients had stable CHF, and many were hospitalized for preoperative examination rather than treatment. The reason that this cohort was different from that in the general Japanese cohort study is many patients underwent surgery for valvular disease at the facility of the present study, and this must be considered in the interpretation of our results.
This study had several limitations. First, this study involved a relatively small patient population and was performed at a single facility. Further studies involving more patients are needed to gather additional evidence. Second, we focused on the prediction of falls according to the 5STS time, but the patients’ actual history of falls was not investigated. Third, we did not evaluate the doses of medications or the strength of medical therapy for CHF. Fourth, the effects of nutritional interventions and organizing drugs were not examined. Further investigations are needed to elucidate the precise physical function, nutritional status, and polypharmacy in patients with stable CHF.
Conclusion
We investigated the relationship of physical performance parameters, including lower extremity function test results, with muscle weakness, malnutrition, and the number of drugs. Clinicians should consider the nutritional status, number of drugs administered, and muscle strength to prevent a decrease in physical performance, even in patients with stable CHF.
Footnotes
Authors’ contributions
YM contributed to the study conception and design; acquisition, analysis, and interpretation of data; drafting of the article; and final approval of the version to be published. HK contributed to revision of the article. KM contributed to acquisition and classification of data, especially medication data. YY and TF contributed to more than half of the acquisition of physical function data. RK, KE, and KM contributed to critical revision of the manuscript for important intellectual content and final approval of the version to be published from each professional’s point of view.
Declaration of conflicting interests
The authors declare that there is no conflict of interest.
Funding
This study was supported by a Grant-in-Aid for Young Scientists (B) (No. 26750190) from the Japan Society for the Promotion of Science (KAKENHI).