
Abstract
Background:
Advanced age is the most important risk factor for pancreatic cancer and about half of patients are diagnosed with metastatic disease. In the first-line setting, multidrug chemotherapy regimens were shown to be more effective than gemcitabine alone. However, the older population was under-represented in randomized clinical trials. We aimed to describe the clinical profile of older patients with metastatic pancreatic cancer and their survival outcomes.
Materials and methods:
This was a retrospective, unicentric study that included patients diagnosed with metastatic pancreatic cancer (non-neuroendocrine), aged 65 years and over.
Results:
The study population comprised 196 patients. The median age was 73 years; 67% of these patients presented Eastern Cooperative Oncology Group performance status (ECOG) ⩽ 1 and the median Charlson Comorbidity score was 10. Chemotherapy was given to 89% of the patients. The most frequently used chemotherapy regimens were gemcitabine (44%), 5-fluorouracil and oxaliplatin [FOLFOX; 26%], and 5-fluorouracil, oxaliplatin and irinotecan (FOLFIRINOX; 20%). Patients treated with FOLFIRINOX were younger and they presented better performance status. After a median follow up of 19.8 months, the median overall survival (OS) was of 7.2 months and the median time to first-line-treatment failure was 4.6 months. Among patients treated with chemotherapy, the median OS was highest for those treated with FOLFIRINOX (13.8 months), as compared with FOLFOX (7.0 months) or gemcitabine (6.7 months); p = 0.004. Nonetheless, treatment with FOLFIRINOX was associated with increased risk of severe toxicity (p = 0.008).
Conclusion:
Older patients with metastatic pancreatic cancer benefit from palliative chemotherapy, and FOLFIRINOX is a therapeutic option in rigorously selected older patients.
Introduction
Pancreatic cancer is the 14th most frequent malignant neoplasm and the 7th most important cause of cancer-related death worldwide. 1 Additionally, the epidemiological burden of pancreatic cancer is expected to increase significantly in the decades to come, such that by 2030 it is expected to have become the second most common cause of cancer-related death in developed countries, only after lung cancer.2,3
Ductal adenocarcinoma is the most common histological type of pancreatic cancer, representing more than 80% of all malignant pancreatic neoplasms. 4 Given the aggressiveness of this neoplasm, and the lack of effective screening strategies, few patients are diagnosed at the initial stages. It is been estimated that only 20% of the patients are eligible for curative surgery. 5 Roughly half of the patients are diagnosed with metastatic disease, and for them, 5-year overall survival (OS) rates are below 10%.6,7
In the advanced disease scenario, the aim is to extend survival while improving quality of life. In a phase III study published more than 20 years ago, gemcitabine was shown as superior to 5-fluorouracil (5-FU) in terms of both OS and clinical benefit. 8 Subsequently, the PRODIGE4/ACCORD11 trial compared gemcitabine with a regimen containing 5-fluorouracil, oxaliplatin and irinotecan (FOLFIRINOX) and showed that the latter was associated with an expressive gain in median OS (11.1 versus 6.7 months in the control arm). 9 Likewise, in the MPACT trial, the combination of gemcitabine and nab-paclitaxel was superior to single-agent gemcitabine in terms of OS. 10
Advanced age is one of the most important risk factors for pancreatic cancer, 11 and more than half of the cases of pancreatic cancer occur after age 70. 12 Nonetheless, in both the PRODIGE4/ACCORD11 and MPACT trials, the older population was under-represented. In the former study, patients older than 75-years old were excluded, and only 29% of the included patients were aged 65 and over. In the second trial, despite the lack of age threshold for inclusion, older patients represented only 42% of the study population. Thus, it remains undefined to what extent the improvements seen in the systemic treatment of advanced pancreatic cancer apply to the older patient population.
Because of the dearth of data on the benefit and toxicity of palliative chemotherapy in the older population, we conducted a retrospective study to describe the clinical profile of elderly patients with metastatic pancreatic cancer treated at AC Camargo Cancer Center between 2008 and 2016. Additionally, we aimed to evaluate survival outcomes and toxicities among patients treated with different chemotherapy regimens.
Material and methods
This is a retrospective, unicentric study which included older patients with metastatic pancreatic carcinoma treated at AC Camargo Cancer Center from January 2008 to December 2016. At AC Camargo Cancer Center, patients sign an informed consent term authorizing the use of anonymized data for the purpose of retrospective studies. For this reason, the need for additional consent was waived. This study was approved by the AC Camargo Cancer Center Ethics Research Board (ethical approval number 2548/18). Study data can be accessed under personal requisition, after approval by the AC Camargo Cancer Center Ethics Review Board.
Patients
The study included patients with the following characteristics: age 65 and over (at the time of metastatic disease diagnosis); histopathological confirmation of pancreatic carcinoma (non-neuroendocrine); pathological or radiological evidence of metastatic disease; and medical care at AC Camargo Cancer Center from 1 January 2008 to 31 December 2016. Patients treated for a second primary malignant tumor and those who underwent neither chemotherapy nor supportive treatment at AC Camargo Cancer Center were excluded.
Data collection
We collected the following data: demographic information (age and sex); clinical characteristics [Eastern Cooperative Oncology Group performance status (ECOG), age-adjusted Charlson Comorbidity Score (AACCS), polypharmacy, weight loss, body mass index, and family history of cancer]; characteristics of the neoplasm (primary tumor location, sites of metastasis, and serum cancer antigen (CA) 19-9 levels at the date of metastatic disease diagnosis); and information related to the treatment [type of treatment, type of first-line chemotherapy regimen, treatment delay and dose reduction during first-line chemotherapy, use of granulocyte colony-stimulating growth factor (G-CSF) during first-line chemotherapy, and number of subsequent chemotherapy lines]. Polypharmacy was defined as the continuous use of five or more medications. Weight loss was defined as a loss of ⩾10% of body weight in less than 6 months.
Outcomes
The primary objective of our study was to describe the clinico-epidemiological profile of older patients with metastatic pancreatic cancer treated at AC Camargo Cancer Center. Secondarily, we aimed to evaluate overall survival (OS), time to treatment failure in the first-line (TTF1) and toxicity of first-line chemotherapy. Toxicity was assessed according to the Common Toxicity Criteria 4.0. As FOLFIRINOX is expected to be more toxic than other chemotherapy regimens, we analyzed toxicity according to treatment (FOLFIRINOX versus other chemotherapy regimens). OS was defined as the time from diagnosis of metastatic disease to death from any cause. TTF1 was defined as the time from the diagnosis of metastatic disease to disease progression during first-line chemotherapy (as assessed by RECIST or treating physician’s opinion), first-line treatment discontinuation due to limiting toxicity, or death from any cause. Severe toxicity was defined as any toxicity that resulted in admission to the hospital or the emergency department. After the results of multivariate analysis, we performed a post hoc analysis comparing patients treated with FOLFIRINOX with those treated with other chemotherapy regimens.
Statistical analysis
We used absolute values and ratios to describe the distribution of categorical variables. Distributions of categorical variables were compared between different groups using Fisher’s exact test. We used the median value and the interquartile range (IQR) to describe the distribution of numerical variables. Distributions of two different numerical variables were compared using the Mann–Whitney U test. The Kaplan–Meier reverse method was used to calculate median follow-up. We used the Kaplan–Meier method to generate survival curves for OS and TTF1, and the log-rank test to compare survival curves. We used the Cox proportional hazard model to examine potential prognostic factors for OS and TTF1 among patients treated with chemotherapy. Variables with p < 0.20 in the univariate analysis were used to generate the multivariate model. We performed backward variable elimination using likelihood ratio tests and Akaike Information Criteria. We considered a two-tailed p value < 0.05 as statistically significant. Statistical analysis was performed using the software R version 3.4.0.
Results
From 1 January 2008 to 31 December 2016, 371 patients aged 65 and over with the diagnosis of pancreatic carcinoma were registered at AC Camargo Cancer Center. Two hundred forty-nine patients presented metastatic disease either at initial staging or follow up. A total of 53 patients were excluded for the following reasons: diagnosis of second metastatic primary cancer (7 patients) and no treatment whatsoever at AC Camargo Cancer Center (46 patients). Therefore, 196 patients were included and analyzed.
The median age at the time of metastatic disease diagnosis was 73 years (range 65–92); males and females were equally represented. About 95% of patients had ECOG 0–2 (n = 186). The median AACCS was 10 (IQR: 9–10), and polypharmacy was found in 43.8% (n = 86) of the patients. Ninety-five patients (48.4%) presented weight loss. The most frequent primary tumor site was the head of pancreas (58.1%; n = 114). The median number of metastatic sites was one (range one to three) and the liver was the single most frequent site of metastasis (64.7%; n = 127). The median serum level of CA 19.9 at the diagnosis of metastatic disease was 549 U/ml (IQR: 76.6–2807.7); Table 1.
Patients’ characteristics.

Polypharmacy was defined as the use of five or more continuous-use medications.
CA, cancer antigen; ECOG, Eastern Cooperative Oncology Group performance status; IQR, interquartile range; NOS, not otherwise specified.
Treatment
A total of 174 patients (88.7%) received at least one cycle of chemotherapy and 11.3% (n = 22) patients received solely best supportive care (BSC). The main reason for not receiving chemotherapy was poor performance status as judged by the treating physician (50.0%; n = 11); Table 2.
Treatment characteristics.

FOLFIRINOX, 5-fluorouracil, oxaliplatin and irinotecan combination chemotherapy; FOLFOX, 5-fluorouracil and oxaliplatin.
The most commonly used chemotherapy regimens were gemcitabine (44.2%; n = 77), FOLFOX (26.2%; n = 46) and FOLFIRINOX (20%; n = 35). The median duration of first-line treatment was 2.5 months (IQR: 1.1–6.0). The vast majority of patients discontinued first-line treatment (94.8%, n = 165). Disease progression was the main reason for treatment discontinuation (56.4%; n = 93), followed by clinical deterioration (33.3%; n = 55); Table 2.
Survival analysis
Median follow-up was 19.8 months [95% confidence interval (CI) 14.5–34.4]. There were 147 deaths and 45 patients were lost to follow up. In the entire population, median OS was 7.2 months (95% CI 5.5–8.5). Among patients submitted to chemotherapy, median OS was 7.8 months (95% CI 6.4–9.2) and median TTF1 was 4.6 months (95% CI 3.9–5.5); Figure 1. In the subgroup of patients who received BSC only, median OS was 2.9 months (95% CI 0.9–4.2); this is significantly inferior (p < 0.001) to the median OS of patients treated with chemotherapy. Among patients treated with chemotherapy, median OS was higher (p = 0.004) for those treated with FOLFIRINOX (13.8 months; 95% CI 9.2–31) when compared with those treated with FOLFOX/5-fluorouracil and irinotecan (FOLFIRI) (7.0 months; 95% CI 5.6–8.2) or gemcitabine (6.7 months; 95% CI 5.0–9.9); Figure 2.
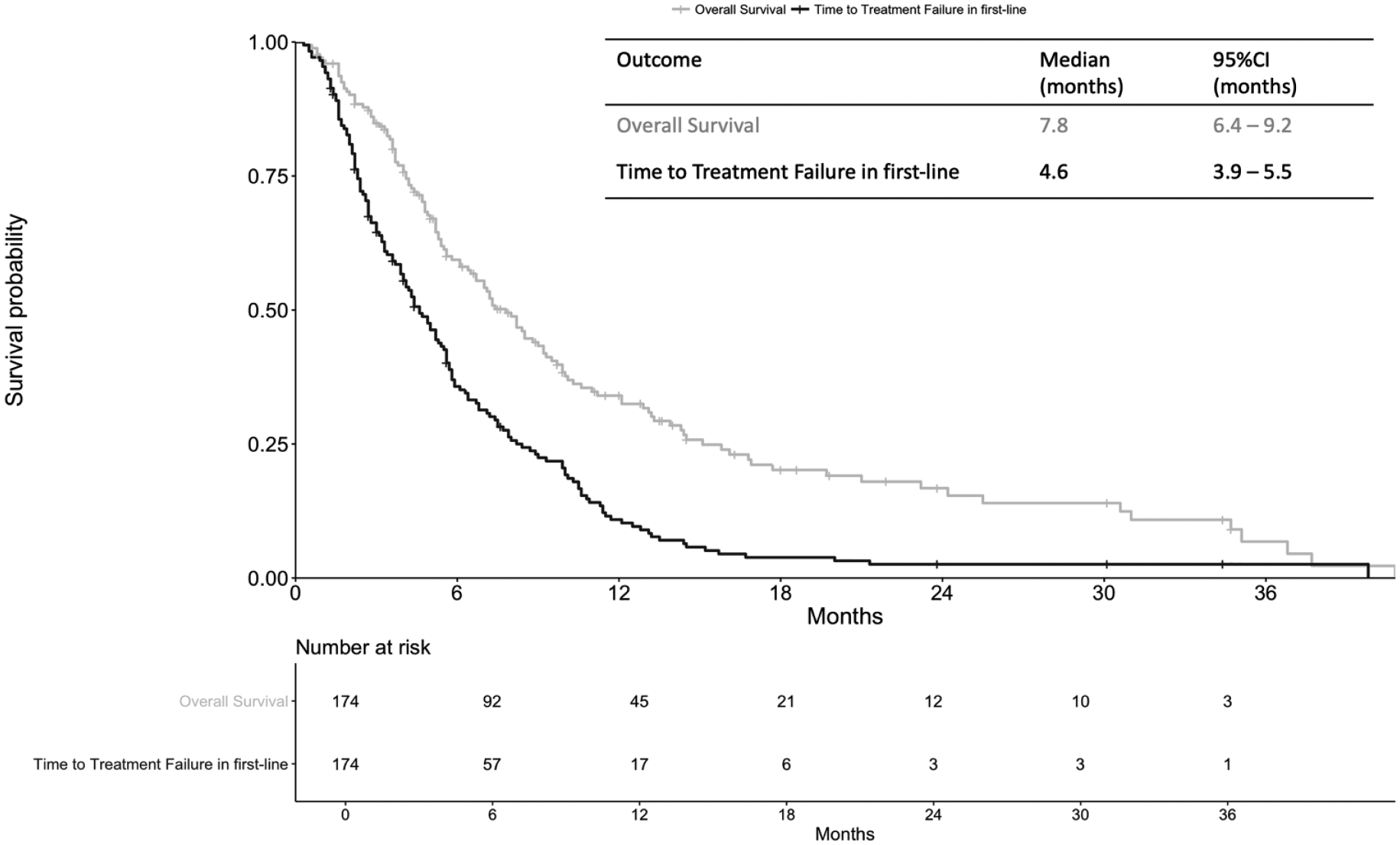
Overall survival and time to treatment failure in the first-line among patients treated with at least one line of chemotherapy.

Overall survival among patients treated with at least one line of chemotherapy according to the chemotherapy regimen.
FOLFIRINOX versus other chemotherapy regimens
In an exploratory analysis, we compared two groups according to the first-line treatment used: FOLFIRINOX (n = 35) versus other chemotherapy regimens (n = 139). The FOLFIRINOX group had lower age at diagnosis of metastatic disease (68 years versus 73 years for other regimens; p < 0.001), lower AACCS (9 versus 10 for other regimens; p < 0.001), and higher frequency of patients ECOG 0–1 (88.5% versus 66.3% for other regimens; p = 0.039); Supplementary Table 1. Additionally, Supplementary Table 2 depicts OS of patients treated with different chemotherapy regimens according to age at diagnosis, AACCS, and ECOG.
Toxicity
Most patients receiving FOLFIRINOX required some sort of dose adjustment (88.6%; n = 31), whereas 48.9% (n = 68) of patients treated with other chemotherapy regimens needed dose modifications (p < 0.001); Table 3. The use of G-CSF as primary prophylaxis for febrile neutropenia was more frequent (p < 0.001) in the FOLFIRINOX group (57.1%; n = 20) than in the other chemotherapy regimens group (2.9%; n = 4). There was no statistical difference between the two groups regarding overall grades 3–5 toxicities. However, severe toxicity was more common in the FOLFIRINOX group (42.9%; n = 15) than in the other chemotherapy regimens group (18.0%; n = 25; p = 0.008). There were two deaths attributed to chemotherapy in the FOLFIRINOX group (5.7%) and none in the other chemotherapy group (p = 0.04). Both deaths were due to febrile neutropenia and septic shock.
Treatment characteristics and toxicity profile of patients undergoing FOLFIRINOX and other chemotherapy regimens.
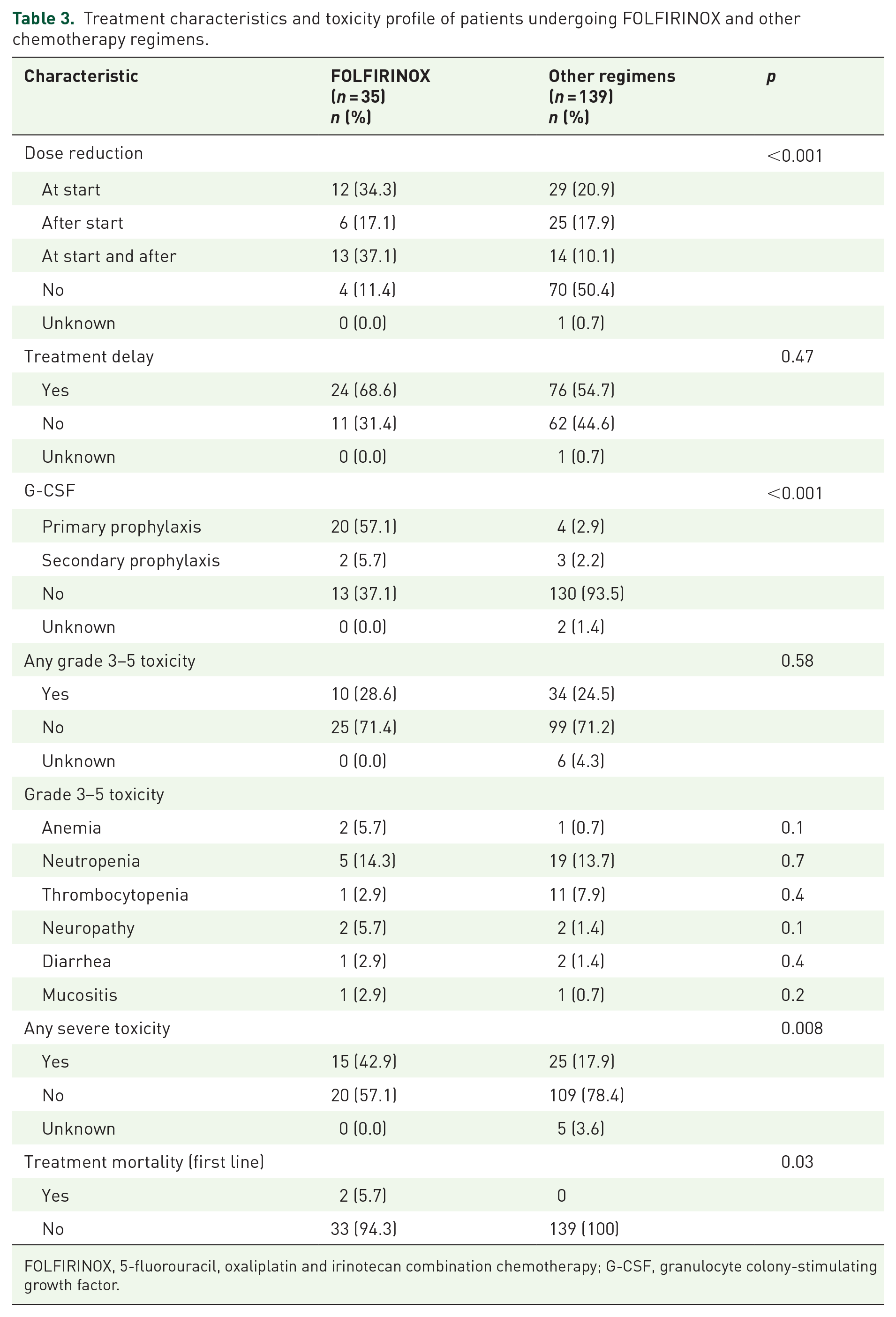
FOLFIRINOX, 5-fluorouracil, oxaliplatin and irinotecan combination chemotherapy; G-CSF, granulocyte colony-stimulating growth factor.
Prognostic factors
In the multivariate analysis, ECOG 1 [hazard ratio (HR) = 2.39, 95% CI 1.29–4.43; p = 0.005], ECOG 2–3 (HR = 3.19, 95% CI 1.62–6.28; p < 0.001), and serum CA 19-9 levels ⩾ 3.000 U/ml (HR = 2.33, 95% CI 1.46–3.70; p < 0.001) were associated with inferior OS among patients treated with chemotherapy. Additionally, the use of chemotherapy regimens other than FOLFIRINOX was an adverse prognostic factor for OS (FOLFOX or FOLFIRI: HR = 2.01, 95% CI, 1.10–3.66, p = 0.022; gemcitabine: HR = 2.06, 95%CI 1.13–3.76; p = 0.018); Table 4.
Cox’s proportional hazard model for overall survival for patients submitted to first-line chemotherapy (n = 174).

AACCS, age-adjusted Charlson Comorbidity Score; CA, cancer antigen; CI, confidence interval; ECOG, Eastern Cooperative Oncology Group performance status; FOLFIRINOX, 5-fluorouracil, oxaliplatin and irinotecan combination chemotherapy; FOLFOX, 5-fluorouracil and oxaliplatin; FOLFIRI, 5-fluorouracil and irinotecan; HR, hazard ratio.
In the multivariate model for TTF1, the following prognostic factors were associated with worse outcome: serum CA 19-9 level ⩾ 3.000 U/ml (HR = 2.03, 95% CI 1.36–3.04; p < 0.001) and use of chemotherapy regimens other than FOLFIRINOX. In this regard, patients treated with gemcitabine showed the highest risk of failure when compared with FOLFIRINOX (HR = 2.29, 95% CI 1.41–3.72; p < 0.001); Table 5.
Cox’s proportional hazard model for time to treatment failure in the first-line (n = 174).

AACCS, age-adjusted Charlson Comorbidity Score; CA, cancer antigen; CI, confidence interval; ECOG, Eastern Cooperative Oncology Group performance status; FOLFIRINOX, 5-fluorouracil, oxaliplatin and irinotecan combination chemotherapy; FOLFOX, 5-fluorouracil and oxaliplatin; FOLFIRI, 5-fluorouracil and irinotecan; HR, hazard ratio.
Further treatments
Overall, 72 patients (41.3%) received at least one chemotherapy regimen after first-line treatment failure; Supplementary Table 3. Patients in the FOLFIRINOX group were more likely to receive further treatments after failure on first-line (60.0%; n = 21) than patients treated with other regimens (36.6%; n = 51; p = 0.05).
Discussion
Pancreatic cancer predominantly affects older adults. It has been shown 73% of all patients with pancreatic cancer in the USA are aged 65 and over. 13 Nonetheless, this group has been systematically under-represented in clinical trials. Even in specialized cancer hospitals, only 5% of older patients with pancreatic cancer are enrolled onto clinical trials. 14 Previous retrospective studies have shed light on the characteristics and treatment outcomes of older patients with pancreatic cancer. However, many of these studies did not portray the use of new and more effective chemotherapy regimens. That said, it is not known to what extent the improvements witnessed in the treatment of metastatic pancreatic cancer according to recent clinical trials hold true for older patients.
The survival gains associated with chemotherapy in metastatic pancreatic cancer are well-established. 15 Nonetheless, older patients with advanced pancreatic cancer are less likely than the younger counterparts to receive anticancer therapy. 16 At the population level, less than 25% of all older patients with metastatic pancreatic cancer are given anticancer treatment. 17 In part, this stems from the misconception that older patients with pancreatic cancer derive less survival benefit from chemotherapy. The role of age as a prognostic factor in patients with advanced pancreatic cancer is controversial and there are significant data from retrospective studies suggesting that the benefit from chemotherapy is not dependent on chronological age.18,19
In our hospital, 89% of all older patients with metastatic pancreatic cancer received chemotherapy. This number is significantly higher than the ones seen in other studies. It might be explained by the age threshold used in our study14,20 and by the fact that, as in other single-center studies, many of our patients are self-seeking individuals searching for treatment in a cancer-dedicated institution. 14 However, the reasons for not delivering anticancer treatment to older patients with pancreatic cancer are complex, and they also involve sociocultural and family issues.19–21 In a Latin American country, cultural and religious beliefs might have impacted the drive to perform chemotherapy, as seen in other scenarios of advanced cancer care in the Hispanic American population. 22 That said, we believe after a rigorous patient assessment, a fair discussion about treatment expectations is the best way to decide whether or not to treat an older patient with advanced pancreatic cancer.
Our data show that older patients treated with chemotherapy fare significantly better than those treated solely with BSC. This is also supported by findings from previous investigations.18,19 Despite the selection bias, the median OS of the treated patients in our study is very close to that of the patients in the experimental arm of the MPACT trial, 10 clearly reaffirming the role of chemotherapy in this setting. Thus, given the chance to extend survival and palliate symptoms in properly selected older patients with metastatic pancreatic cancer, age should not be considered a dominant factor in determining treatment strategies.
The most studied chemotherapy regimen in older patients with pancreatic cancer is single-agent gemcitabine. It has been shown to be effective and safe in this population. 23 In our study, 44% of all patients were treated with single-agent gemcitabine in the first-line setting. The median OS of these patients was somewhat inferior to the ones observed in other retrospective analysis of older patients treated with gemcitabine-based regimens.20,24,25 In contrast to what was seen in other investigations, all patients in our study had metastatic disease. Also, some of the patients in these studies were given gemcitabine-based combinations. Both these arguments explain the slightly inferior survival outcomes. Additionally, our survival data compare favorably to the ones of the pivotal randomized trial that tested the activity of single-agent gemcitabine, 8 and we believe these figures better reflect the true survival of older patients with metastatic pancreatic cancer treated with single-agent gemcitabine.
Some of the patients in our study were treated with FOLFOX based on a putative higher response rate when compared with gemcitabine and on its favorable toxicity profile. 26 Nevertheless, the survival of patients treated with the former regimen was not superior to that of patients treated with single-agent gemcitabine. During most of the study’s timespan, nab-paclitaxel was not available in Brazil. Therefore, we could not evaluate its activity and compare it with single-agent gemcitabine (only one patient was treated with gemcitabine plus nab-paclitaxel). In the pivotal trial, gemcitabine plus nab-paclitaxel has been given to elderly patients 10 and subsequently even to patients with ECOG = 2, 27 with a relatively mild toxicity profile, especially when given as a modified regimen. 28 Thus, we believe that the combination of gemcitabine plus nab-paclitaxel might be particularly useful for the older population with advanced pancreatic cancer. However, for those not deemed fit enough for either gemcitabine plus nab-paclitaxel or FOLFIRINOX, we believe single-agent gemcitabine should be considered standard of care.
FOLFIRINOX stands as the regimen with the most impressive survival figures in metastatic pancreatic cancer. 9 Nonetheless, in the pivotal study, only 29% of the patients were aged 65 and over. Also, concerns about its increased toxicity rates when compared to gemcitabine have hindered its use in older patients. In our study, patients treated with FOLFIRINOX experienced a median OS of 13.8 months, significantly longer than that of patients treated with other regimens and treatment with FOLFIRINOX was independently associated with improved OS. Patients treated with FOLFIRINOX were younger and presented better ECOG performance status. In line with our data, recent evidence suggests that, in properly selected older patients with advanced pancreatic cancer, FOLFIRINOX can be safely given with survival results comparable with the ones seen in younger patients.29–31
However, in our study, two deaths (5.7%) were attributed to FOLFIRINOX-related toxicity. Both these patients had ECOG = 2 and died from neutropenic septic shock. Also, patients treated with FOLFIRINOX had a higher frequency of severe toxicity when compared with other chemotherapy regimens. It has been previously shown that the incidence of severe neutropenia and febrile neutropenia during treatment with FOLFIRINOX is higher in older patients. 32 Thus, care must be taken in delivering this regimen to older patients. Notably, modifications of the FOLFIRINOX regimens have been shown to maintain its efficacy while reducing the frequency of side effects.33,34 Also, a more liberal use of prophylactic G-CSF is likely to improve the safety profile of FOLFIRINOX in this population. Currently, researchers of a phase II trial (PAMELA70) are enrolling older patients to treatment with modified FOLFIRINOX; the results of this trial are expected to improve understanding of the role of FOLFIRINOX in the treatment of older patients with metastatic pancreatic cancer [ClinicalTrials.gov identifier: NCT02143219].
We believe the decision to deliver anticancer treatment to older patients with metastatic pancreatic cancer is complex, also entailing subjective factors, such as cultural and religious aspects. However, objective information should be used to optimally assess patient suitability for treatment and to define the best chemotherapy regimen. In this sense, use of geriatric assessments is valuable in aiding the treating physician to define proper treatment strategies, as they can detect subtle health conditions not picked up during routine clinical practice.14,35
Also, information about the prognostic factors in this population might help physicians decide the best treatment approach. In our study, poor performance status, treatment other than FOLFIRINOX, and serum CA 19-9 levels ⩾ 3000 UI/ml were associated with worse OS in the multivariate analysis. Poor performance status and treatment regimens using fewer drugs are well-documented factors associated with worse survival in the older population.14,18 Other studies have shown that high serum CA 19-9 levels are also associated with worse OS, as this translates to a higher tumor burden. 20 Interestingly, poor ECOG was associated with worse OS but not with worse TTF1. In advanced pancreatic cancer, this might be explained by the fact that outcomes like progression-free survival or time to treatment failure are more driven by the tumor growth rate, while OS is more dependent on the general health status of the patient. 36
In our study, age and AACCS were associated with OS and TTF1 only in the univariate analysis. Due to collinearity issues, only the comorbidity index was used in the multivariate analysis and it was not an independent prognostic factor. We believe that apart from the patient’s clinical condition, age and comorbidities play a less significant part in survival in a disease characterized by an aggressive behavior such as pancreatic adenocarcinoma. 18
Our study has some limitations. It represents a retrospective, single institution experience in the treatment of older patients with metastatic pancreatic cancer. Also, we do not have data on response to treatment or quality of life. Additionally, patients in our study were not submitted to formal geriatric assessment. Nonetheless, we present data on a robust number of older patients treated in a cancer-dedicated hospital. Also, our study brings new data on the patterns of treatment of older patients with pancreatic cancer in a Latin American country, with its diverse religious and cultural aspects. We also provide detailed information regarding patients’ features, treatments, and outcomes.
To conclude, chemotherapy is associated with improved survival in older patients with metastatic pancreatic cancer considered fit enough for treatment, and advanced age alone should not hamper the delivery of anticancer treatment for these patients. Also, FOLFIRINOX may be suitable for adequately selected patients, and this regimen provides superior survival. Lastly, in the older population with pancreatic cancer, poor performance status, treatment with regimens other than FOLFIRINOX, and elevated serum CA 19-9 levels were associated with inferior outcomes.
Supplemental Material
Supplementary_tables – Supplemental material for Characteristics and survival of older patients with metastatic pancreatic cancer: a retrospective analysis of the AC Camargo Cancer Center experience
Supplemental material, Supplementary_tables for Characteristics and survival of older patients with metastatic pancreatic cancer: a retrospective analysis of the AC Camargo Cancer Center experience by Josenon Gomes Costa, Victor Hugo Fonseca de Jesus, Marcos Pedro Guedes Camandaroba and Aldo Lourenço Abbade Dettino in Therapeutic Advances in Medical Oncology
Footnotes
Acknowledgements
We thank Dr Rachel Simões Pimenta Riechelmann, head of the Medical Oncology Department at the AC Camargo Cancer Center, for supporting this study.
Josenon Gomes Costa: conceptualization, methodology, investigation, writing and visualization; Victor Hugo Fonseca de Jesus: conceptualization, methodology, data curation, writing and visualization; Marcos Pedro Guedes Camandaroba: conceptualization, methodology, writing and visualization; Aldo Lourenço Abbade Dettino: conceptualization, methodology, writing and visualization.
Funding
The authors received no financial support for the research, authorship, and/or publication of this article.
Conflict of interest statement
The authors declare that there is no conflict of interest.
Supplemental material
Supplemental material for this article is available online.
References
Supplementary Material
Please find the following supplemental material available below.
For Open Access articles published under a Creative Commons License, all supplemental material carries the same license as the article it is associated with.
For non-Open Access articles published, all supplemental material carries a non-exclusive license, and permission requests for re-use of supplemental material or any part of supplemental material shall be sent directly to the copyright owner as specified in the copyright notice associated with the article.