
Abstract
Pancreatic adenocarcinoma is one of the deadliest solid malignancies. A large proportion of patients are diagnosed with locally advanced or metastatic disease at the time of presentation and, unfortunately, this severely limits the number of patients who can undergo surgical resection, which offers the only chance for cure. Recent therapeutic advances for patients with advanced pancreatic cancer have extended overall survival, but prognosis still remains grim. Given that traditional chemotherapy is ineffective in curing advanced pancreatic adenocarcinoma, current research is taking a multidirectional approach in the hopes of developing more effective treatments. This article reviews the major clinical trial data that is the basis for the current chemotherapy regimens used as first- and second-line treatments for advanced pancreatic adenocarcinoma. We also review the current ongoing clinical trials, which include the use of agents targeting the oncogenic network signaling of K-Ras, agents targeting the extracellular matrix, and immune therapies.
Introduction
According to the American Cancer Society, there were an estimated 45,220 new cases of pancreatic adenocarcinoma in 2013 with an astounding 38,460 deaths [Siegel et al. 2013]. Despite comprising only 3% of all new cancer diagnoses, pancreatic cancer remains the fourth most common cause of cancer death [Siegel et al. 2013], and it is expected to rise to the second most common cause of death by 2030. Pancreatic cancers are typically diagnosed at advanced stages when the only available treatments are palliative; around 40% of patients are found to have metastatic disease at the time of diagnosis. During the last decade, the overall survival (OS) of patients with metastatic disease lingered around 6 months [Burris et al. 1997]. It has only been within the last 2 years, due to recent therapeutic advancements, that the OS was extended to nearly 1 year [Conroy et al. 2011; Von Hoff et al. 2013]. In this article, we review historical treatments, recent advances and current research in metastatic pancreatic adenocarcinoma.
First-line therapy for metastatic pancreatic cancer
Chemotherapeutics
5-fluorouracil monotherapy
Fluorouracil-based chemotherapy was the mainstay of treatment for pancreatic adenocarcinoma since the 1950s, despite mean survival of less than 6 months (Moertel, 1978), until recent therapeutic advances increased overall survival to nearly 1 year. Attempts to combine 5-fluorouracil (5-FU) with other chemotherapeutics such as doxorubicin, mitomycin C, cyclophosphamide, methotrexate, vincristine and cisplatin increased toxicities, but none of these combinations was shown to increase survival [Cullinan et al. 1985, 1990; Moertel, 1978].
Gemcitabine monotherapy
Gemcitabine was the first chemotherapeutic drug shown to be superior to 5-FU in terms of increasing overall survival. In a randomized controlled trial [Burris et al. 1997], 126 patients with advanced pancreatic cancer were randomized to receive either gemcitabine 1000 mg/m2 weekly for 7 weeks followed by 1 week off, then on days 1, 8, and 15 of a 28-day cycle, or weekly 5-FU 600 mg/m2. The primary endpoint in this trial was clinical benefit, which was defined by a pain score, Karnofsky performance score (KPS), and body weight (Table 1). Not only did patients receiving gemcitabine have a better clinical benefit (23.8% versus 4.2%; p = 0.0022), but gemcitabine-treated patients had a statistically better median overall survival (mOS; 5.65 versus 4.41 months; p = 0.0025) and overall one year survival rate (18% versus 2%; p = 0.0025). The Food and Drug Administration (FDA) based its approval of gemcitabine monotherapy as first-line treatment for advanced pancreatic cancer primarily on this clinical benefit.
Major clinical trials for advanced pancreatic adenocarcinoma.

5-FU, 5-fluorouracil; BSC, best supportive care; GEM, gemcitabine; OS, overall survival; PFS, progression-free survival; wk, week; BID, twice a day.
Gemcitabine-based combination therapies
The demonstrated efficacy of single-agent gemcitabine prompted a series of trials from the late 1990s to 2010s to explore more effective gemcitabine-based combinations [Berlin et al. 2002; Cunningham et al. 2009]. The combination regimen of gemcitabine with capecitabine was tested in two phase III trials. In one trial, 533 treatment-naïve patients with locally advanced or metastatic pancreatic cancer were randomized to receive weekly gemcitabine plus daily capecitabine (GEMCAP) versus gemcitabine alone (GEM) [Cunningham et al. 2009]. Patients treated with GEMCAP showed a trend toward improved OS compared with GEM-treated patients (7.1 versus 6.2 months; p = 0.08) and a statistically significant improvement in overall progression-free survival (PFS) rates at 12 months (13.9% versus 8.4%; p = 0.004); see Table 1. The second phase III study of 319 patients similarly showed a nonstatistically significant trend in mOS (8.4 versus 7.2 months; p = 0.234) and 1-year survival rates (32% versus 30%) in GEMCAP versus GEM-treated patients [Herrmann et al. 2007]. However, post hoc power analysis showed that patients with a good performance status (KPS of 90–100) had a statistically improved mOS (10.1 versus 7.4 months; p = 0.014) and PFS with a hazard ratio (HR) of 0.69 (p = 0.022) when treated with GEMCAP versus GEM [Bernhard et al. 2008; Herrmann et al. 2007]. These two trials set the premise for GEMCAP being recommended in the National Comprehensive Cancer Network (NCCN) Guidelines as a reasonable option for patients with metastatic pancreatic cancer who have a good performance status.
The addition of platinum to gemcitabine failed to improve survival over gemcitabine alone in several phase III trials [Colucci et al. 2002; Heinemann et al. 2006]. For example, in a large phase III trial, 400 patients with advanced pancreatic adenocarcinoma were randomized to receive either gemcitabine or gemcitabine with cisplatin. Gemcitabine 1000 mg/m2 was administered weekly for 7 weeks followed by 1 week off then on days 1, 8, and 15 every 28 days. In the combination arm, gemcitabine was given on the same schedule along with cisplatin 25 mg/m2 on days 1, 8, 15, 29, 36, and 42 followed by 1 week off, and then both drugs were continued on days 1, 8, and 15 every 28 days [Heinemann et al. 2006]. The addition of cisplatin to gemcitabine did not improve mOS (8.3 versus 7.2 months; p = 0.38) or PFS (3.9 versus 3.8 months; p = 0.80) compared with gemcitabine alone (Table 1). However, a meta-analysis of 5 randomized trials with a total of 623 patients revealed a clinically significant survival benefit in patients receiving gemcitabine plus a platinum analog compared with gemcitabine alone (HR = 0.85; p = 0.010) [Rougier et al. 2013], but only when a combined analysis of the 5 trials was performed. The NCCN has endorsed the combination of a platinum analog to gemcitabine in the advanced setting, but generally only for those patients with possible hereditary pancreatic cancer.
BRCA mutations
Although cisplatin combined with gemcitabine is generally not the standard of care based on the clinical trials discussed earlier, emerging evidence suggests that patients with BRCA-mutated or familial pancreatic cancer may be particularly sensitive to a cisplatin-based regimen. Mutations in BRCA1/2 result in inefficient repair of damaged DNA by homologous recombination, increasing the risk of developing a malignancy [Moynahan et al. 1999]. A retrospective study conducted in 2010 at Johns Hopkins University evaluated 468 metastatic pancreatic cancer patients who had received a cisplatin-based regimen [Oliver et al. 2010]. Cisplatin functions as an alkylating agent and binds with DNA to form intrastrand crosslinks, altering the conformation of DNA and thus affecting DNA replication. Normally, these crosslinks would be repaired by homologous recombination, so BRCA deficient cells are thought to be potentially more sensitive to a platinum-based chemotherapy [Kennedy et al. 2004]. Patients who had a strong family history of breast, ovarian or pancreatic cancer had a mOS of 22.9 months versus 6.3 months (p ⩽ 0.01) for patients without a strong family history of these cancers. In a small case series, 15 patients with either a BRCA1 or BRCA2 mutation had a mOS of 27.6 months when treated with a poly (ADP- ribose) polymerase (PARP) inhibitor or platinum-based chemotherapy [Lowery et al. 2012]. The PARP family of proteins binds DNA and is associated with repairing damaged DNA, so inhibiting PARP prevents the repair of damaged DNA and ultimately leads to cell apoptosis and cell death [Murai et al. 2012]. Although neither of these studies were randomized prospective clinical trials, a platinum-containing regimen may be considered in patients with BRCA-mutated or familial pancreatic adenocarcinoma given the significant improvement in mOS.
Like cisplatin, addition of oxaliplatin [Louvet et al. 2005; Poplin et al. 2009], irinotecan [Stathopoulos et al. 2006] or pemetrexed [Oettle et al. 2005] to gemcitabine failed to improve OS in several phase III trials. In the GERCOR and GISCAD trials, combined gemcitabine and oxaliplatin showed statistically significant improvement of PFS (5.8 versus 3.7 months; p = 0.04), but not mOS (9.0 versus 7.1 months; p = 0.13) [Louvet et al. 2005]; see Table 1. A randomized phase III ECOG study (E6201) of 832 patients comparing fixed-dose rate (FDR) gemcitabine (1500 mg/m2 administered as a 150-minute infusion on days 1, 8, and 15 every 28 days cycle), versus standard weekly gemcitabine given as a 30-minute infusion weekly for 3 weeks followed by 1 week off or gemcitabine 1000 mg/m2 administered as a 100-minute infusion on day 1 in combination with oxaliplatin 100 mg/m2 on day 2 (GEMOX) given every 14 days, did not find a significant improvement in mOS or PFS [Poplin et al. 2009].
Recent advances
FOLFIRINOX (5-FU, leucovorin, irinotecan and oxaliplatin)
In 2011, combination chemotherapy in metastatic pancreatic cancer finally showed a meaningful survival benefit over single agent gemcitabine [Conroy et al. 2011]. The ACCORD phase II/III trial [Conroy et al. 2011] studied 342 patients with previously untreated metastatic pancreatic cancer who were randomized to receive FOLFIRINOX (5-FU 400 mg/m2 IV on day 1 followed by 2400 mg/m2 continuous IV infusion over 46 hours, leucovorin 400 mg/m2 IV on day 1, irinotecan 180 mg/m2 IV on day 1, and oxaliplatin 85 mg/m2 IV on day 1 given every 14 days) or gemcitabine (1000 mg/m2 IV given weekly for 7 weeks then weekly for 3 weeks followed by 1 week off) alone. Patients treated with FOLFIRINOX had a significantly improved mOS of 11.1 months compared with 6.8 months in the gemcitabine arm (p < 0.001), as well as an improved PFS of 6.4 months compared with 3.3 months (p < 0.001); see Tables 1 and 2. A higher tumor response rate was seen in the FOLFIRINOX arm as well (31.6% versus 9.4%; p < 0.001). Perhaps not surprisingly, there was a significantly increased incidence of grade 3 and 4 toxicities in the FOLFIRINOX arm compared with gemcitabine (Table 2). Interestingly, 31% of the patients in the FOLFIRINOX group, as opposed to 66% of patients in the gemcitabine group, had a definitive decrease in the scores on the Global Health Status and Quality of Life scale at 6 months (HR = 0.47; 95% confidence interval [CI] 0.30–0.70; p < 0.001), which most likely is a result of improved survival in the FOLFIRINOX group [Gourgou-Bourgade et al. 2013]. FOLFIRINOX is now considered one of the first-line regimens for patients with metastatic pancreatic cancer and good performance status.
First-line therapies for metastatic pancreatic adenocarcinoma.

GEM, gemcitabine; 5-FU, 5-fluorouracil; PR, partial response; CR, complete response; SD, stable disease; PD, progressive disease; OS, overall survival; PFS, progression-free survival; mo, months.
Gemcitabine plus nab-paclitaxel
Of all epithelial tumors, pancreatic adenocarcinoma has one of the densest stroma, and this is thought to contribute to chemotherapy resistance by reducing drug delivery to cancer cells [Li et al. 2012]. Nab-paclitaxel is the most recently approved first-line treatment for metastatic pancreatic cancer in combination with gemcitabine. Nanoparticle albumin-bound paclitaxel (nab-paclitaxel) uses nanotechnology to combine human albumin with paclitaxel, which allows for the delivery of an insoluble drug in the form of nanoparticles to the tumor, increasing the bioavailability of paclitaxel. For intracellular uptake of nab-paclitaxel into pancreatic stromal cells, specific albumin-binding proteins are necessary. Secreted protein acidic and rich in cysteine (SPARC) has been proposed to be one of these [Infante et al. 2007]. The albumin portion of nab-paclitaxel is thought to bind to SPARC, allowing the drug to then enter cells. SPARC has also been proposed as a biomarker for nab-paclitaxel-based regimens. Peritumoral fibroblasts in pancreatic adenocarcinoma have been shown to overexpress SPARC [Von Hoff et al. 2006] and overexpression was previously found to be a marker of poor prognosis, but only when SPARC was expressed in the stroma and not in the pancreatic tumor cells [Infante et al. 2007]. A phase I/II trial of gemcitabine plus nab-paclitaxel showed substantial antitumor activity, with a mOS of 12.2 months and 48% of patients alive at 1 year post-trial [Von Hoff et al. 2011]. SPARC was also evaluated as a biomarker in this trial and SPARC status was evaluated in 36 patients. SPARC levels were evaluated using immunohistochemistry and patients were grouped into either a high-SPARC group (average z-score ⩾ 0) or low-SPARC group (z-score <0). A significant increase in mOS was seen in patients with the high-SPARC group compared with patients in the low-SPARC group (17.8 versus 8.1 months; p = 0.431). However, in another phase II trial of nab-paclitaxel as a second-line agent in metastatic pancreatic cancer, SPARC expression and patient outcome was inconclusive [Hosein et al. 2013]. In a phase III randomized, open-label, multicenter trial (MPACT), 861 untreated patients with metastatic pancreatic cancer were randomized to receive gemcitabine plus nab-paclitaxel or gemcitabine alone [Von Hoff et al. 2013]. mOS, PFS and tumor response rates were significantly improved in the gemcitabine plus nab-paclitaxel group compared with gemcitabine alone (8.5 versus 6.7 months, p < 0.001; 5.5 versus 3.7 months, p < 0.001; 23% versus 7%, p < 0.001, respectively); see Table 2. As expected, patients treated with the gemcitabine/nab-paclitaxel combination had a higher incidence of myelosuppression and peripheral neuropathy (Table 2). A detailed analysis regarding SPARC expression and overall survival from the MPACT trial was recently reported at the European Society for Medical Oncology (ESMO) meeting in 2014, and SPARC was not associated with better survival.
Targeted agents
Anti-EGFR agents
Epidermal growth factor receptor (EGFR) is a transmembrane tyrosine kinase receptor that plays a critical role in cell cycle regulation. Overexpression of EGFR is reported in up to 90% of pancreatic cancer samples [Fjällskog et al. 2003; Tobita et al. 2003], rendering small molecule inhibitors that target the EGFR tyrosine kinase domain a promising therapeutic agent. In a large phase III trial, 569 patients with locally advanced or metastatic pancreatic adenocarcinoma were randomized to receive gemcitabine with or without erlotinib 100–150 mg daily [Moore et al. 2007]. Patients in the combination arm had a modest but statistically significant improvement in mOS (6.24 versus 5.91 months; p = 0.038) and PFS (3.75 versus 3.55 months; p = 0.004). This study led to FDA approval of erlotinib in 2005 in combination with gemcitabine for the treatment of advanced pancreatic adenocarcinoma (Table 1). In a subset analysis of this trial, the mutational status of KRAS and EGFR copy numbers were evaluated in 117 patients; neither was shown to be predictive of a survival benefit in patients receiving the combination of gemcitabine/erlotinib [Da Cunha Santos et al. 2010]. In contrast to the results with combination erlotinib, addition of the EFGR monoclonal antibody cetuximab to gemcitabine did not improve mOS, PFS, or tumor response rates in a phase III randomized, controlled trial (Table 1), even though 92% of patients’ tumor samples stained positive for EGFR by immunohistochemistry [Philip et al. 2010].
In summary, new combination chemotherapies of gemcitabine with nab-paclitaxel or combination chemotherapy with FOLFIRINOX have emerged as the main front-line treatment options for patients with good performance status in the treatment of metastatic pancreatic adenocarcinoma.
Second-line therapy in metastatic pancreatic adenocarcinoma
Despite the aggressive nature of pancreatic cancer, nearly half of patients who have progressed on front-line therapy are able to receive second-line therapy. A fluorouracil-based regimen is currently recommended for patients who progress through gemcitabine. In a phase III clinical trial, patients who had progressed on a gemcitabine-based chemotherapy were randomized to receive folinic acid 200 mg/m2 on day 1, 8, 15, and 22, then 5-FU 2000 mg/m2 as a continuous 24-hour infusion on day 1, 8, 15, and 22, and oxaliplatin 850 mg/m2 on day 8 and 22 of a 42-day cycle (OFF regimen), or best supportive care (BSC) [Pelzer et al. 2011]. The study was terminated early due to low recruitment, but despite this, the OFF regimen showed a median second-line survival of 4.82 versus 2.30 months (p = 0.008) and a mOS survival benefit of 9.09 versus 7.90 months (p = 0.031) in patients treated with OFF compared with BSC. However, recently the results of the CONKO-003 trial were published, which was a randomized, open-label phase III trial in which 168 patients with advanced pancreatic cancer who had progressed on gemcitabine were randomized to folinic acid and fluorouracil (FF) or oxaliplatin and FF (OFF) [Oettle et al. 2014]. Median overall survival was significantly longer in the OFF group compared with FF alone (5.9 versus 3.3 months; p = 0.010). Progression-free survival was also extended in the OFF treatment arm compared with the FF arm (2.9 versus 2.0 months; p = 0.019). Based on these trials, the NCCN Guidelines recommends fluropyrimidine plus oxaliplatin as a second-line treatment option. Although both of these clinical trials used the OFF regimen, most clinicians in the US will give oxaliplatin, folinic and fluorouracil as FOLFOX (oxaliplatin 85 mg/m2 on day 1, 5-FU 400 mg/m2 IV on day 1 followed by 2400 mg/m2 continuous infusion over 46 hours, and leucovorin 400 mg/m2 IV on day 1 repeated every 14 days), based on familiarity with this regimen, as it is commonly used for other gastrointestinal malignancies, and ease of administration. Other chemotherapeutic agents, such as pemetrexed [Boeck et al. 2007], paclitaxel [Oettle et al. 2000], oxaliplatin [Androulakis et al. 2005] and capecitabine [Boeck et al. 2007], were investigated in advanced or metastatic pancreatic cancer after progression on gemcitabine. Pemetrexed, paclitaxel, oxaliplatin and capecitabine showed a mOS of 4.7, 4.1, 3.9 and 7.3 months, respectively, whereas OS for patients receiving BSC is only around 10 weeks. Given that there is no standard of care for patients who progress after gemcitabine, patients ideally should be enrolled in clinical trials. For patients who received FOLFIRINOX in the front-line setting, the second-line option often is a gemcitabine-based therapy, although there is no clear evidence to support this approach. In patients with good performance status, gemcitabine combined with nab-paclitaxel is commonly used due to the survival benefit of this combination in the front-line setting, but the true clinical benefit of gemcitabine plus nab-paclitaxel in the second-line setting is still largely unknown. There is no standard of care currently recommended for patients who have progressed beyond two lines of systemic therapies, so for these patients, clinical trials are recommended.
Current investigational strategies
Given that metastatic pancreatic cancer remains one of the most lethal solid malignancies, current research is taking a multidirectional approach, and novel targeted approaches are being developed that will hopefully improve survival of patients with pancreatic cancer.
Improved chemotherapy
Many clinical trials are currently in phase II/III development with different chemotherapeutic combinations in the hopes that one of these will supersede FOLFIRINOX as either superior in clinical response or equivalent but less toxic. These combinations include dose-attenuated FOLFIRINOX [ClinicalTrials.gov identifier: NCT01523457] and gemcitabine plus etoposide, the latter of which has just completed analysis in a phase II trial [ClinicalTrials.gov identifier: NCT00202800]. However, the majority of the ongoing phase II/III clinical trials for metastatic pancreatic cancer involve combining gemcitabine plus nab-paclitaxel with a novel agent.
Overall, traditional chemotherapy has been disappointing in the treatment of metastatic pancreatic cancer. One approach to this problem is to develop more potent chemotherapeutic drugs. PEP02 is irinotecan encapsulated into liposomal-based nanoparticles; this modification to the delivery of irinotecan prolongs the time the drug remains in circulation and increases its efficacy without significantly increasing its toxicity [Drummond et al. 2006]. In a phase II trial, 40 patients were enrolled to receive PEP02 120 mg/m2 every 3 weeks with the primary objective being the 3-month survival rate. The OS rate at 3 months was 75%, with a median PFS of 2.4 months and mOS of 5.2 months [Ko et al. 2013]. The data from the phase III trial (NAPOLI-1 trial) of nanoliposomal irinotecan sucrosofate (MM-398, also known as PEP02) was recently presented at the European Society of Medical Oncology’s 16th World Congress on Gastrointestinal Cancer in Barcelona [Von Hoff et al. 2014]. In this phase III trial, 417 patients with metastatic pancreatic adenocarcinoma who had progressed after a gemcitabine-based regimen, were randomized to receive either MM-398 120 mg/m2 IV every 3 weeks, 5-FU 2000 mg/m2 IV over 24 hours with leucovorin 200mg/m2 weekly for 4 weeks followed by 2 weeks off, or a combination of MM-398 80 mg/m2 IV with 5-FU 2,400 mg/m2 given over 46 hours with leucovorin 400 mg/m2 every 2 weeks. The primary endpoint was OS. Overall survival was significantly improved with the combination therapy of MM-398 plus 5-FU and leucovorin compared to 5-FU and leucovorin alone, with a mOS of 6.1 months compared with 4.2 months, respectively (HR = 0.67, p = 0.012). Progression-free survival also improved significantly, from 1.5 months with the standard therapy compared with 3.1 months in patients receiving MM-398 with 5-FU and leucovorin (HR = 0.56, p < 0.001). MM-398 alone did not demonstrate a statistically significant improvement in efficacy. Given the positive results, MM-398 is in the process of being filed with the FDA for approval for use in pancreatic cancer.
Targeted therapies
EGFR inhibition
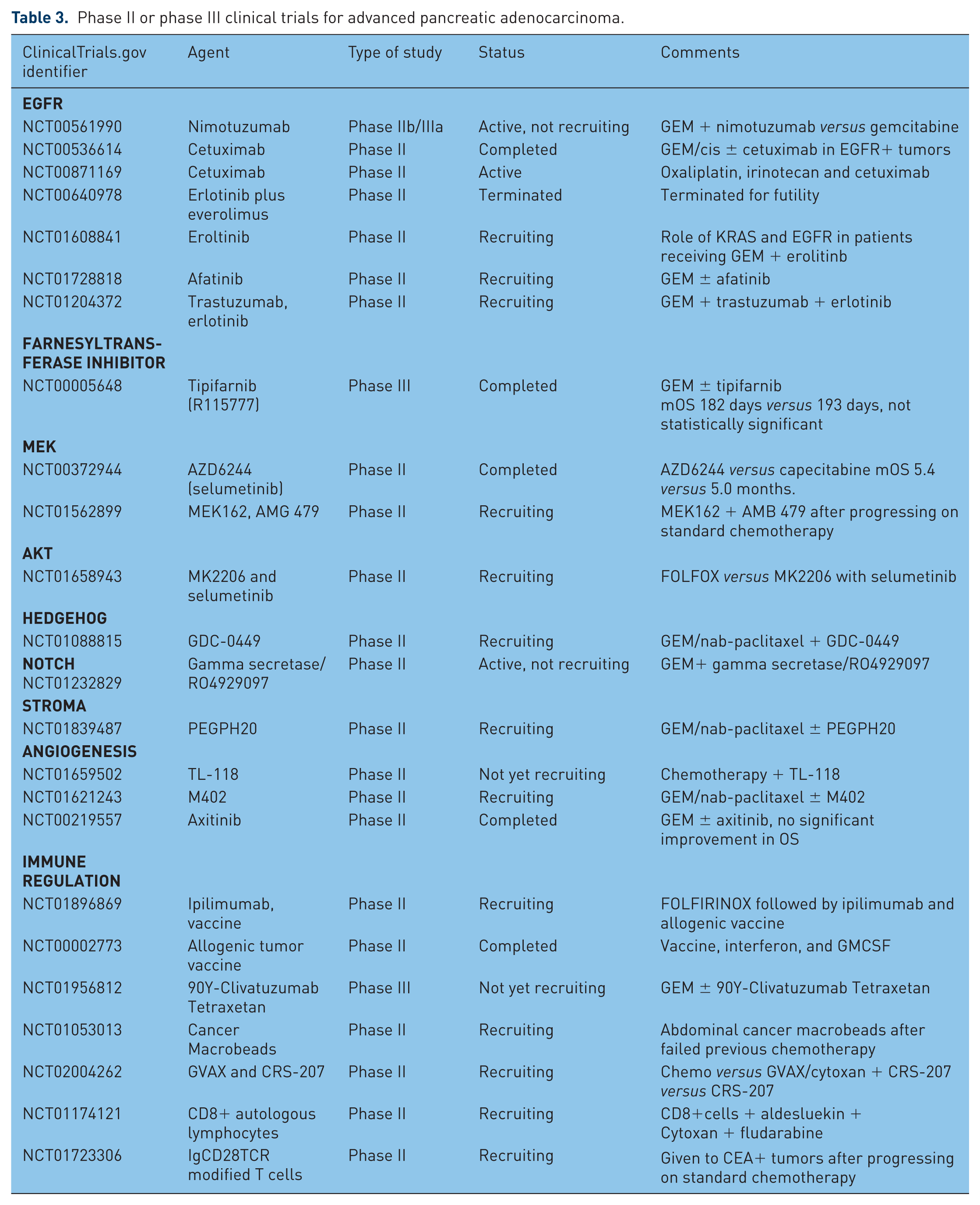
Binding of EGFR to its ligand leads to dimerization of EGFR, activation of its tyrosine kinase domains and downstream activation of the RAS/RAF/MEK, PIK3/AKT and JAK/STAT pathways, which are important in cell proliferation and survival [Eser et al. 2014]. Preclinical studies showed that KRAS-mutated pancreatic cancer requires intact EGFR signaling for survival and progression [Ardito et al. 2012; Navas et al. 2012]. Despite this, as discussed previously, the phase III clinical trial with erlotinib only showed a very modest improvement in mOS [Moore et al. 2007]. At present, other anti-EGFR agents such as nimotuzumab, a humanized anti-EGFR monoclonal antibody; afatinib, a dual EGFR and HER2 tyrosine kinase inhibitor; and combined trastuzumab and erlotinib are being evaluated in phase II trials (Table 3).
Phase II or phase III clinical trials for advanced pancreatic adenocarcinoma.
IGFR inhibition
Binding of the insulin-like growth factor-1 receptor (IGFR) to its ligand, like EGFR, leads to the activation of signaling pathways, including activation of the PIK3/AKT pathway, which is important in cell proliferation and survival [Sachdev and Yee, 2007]. Two monoclonal antibodies against IGFR, AMG-479 (ganitumab) and MK-0646 (dalotuzumab), are being evaluated in clinical trials. To date, AMG-479 in combination with gemcitabine has not been shown to be effective. The phase III GAMMA trial of gemcitabine with AMG-479 was closed after a preplanned interim analysis showed that the addition of AMG-479 to gemcitabine was unlikely to demonstrate a statistically significant improvement in the primary endpoint of overall survival compared with gemcitabine alone. There is currently one active phase II trial in which AMG-479 is combined with a mitogen-activated extracellular kinases (MEK) inhibitor (Table 3).
Direct RAS targeting
Mutational activations of KRAS are present in up to 90% of pancreatic cancers [Almoguera et al. 1998], resulting in constitutively active RAF/MEK/ERK and PIK3/AKT pathways and uncontrolled cellular growth. Given the high rate of this mutation seen in pancreatic cancer, inhibiting KRAS seems an attractive target. Following translation, Ras proteins undergo post-translational modifications including farnesylation, which allows the Ras protein to be attached to the plasma membrane for signal transduction [Takashima and Faller, 2013]. Unfortunately, several farnesyltransferase inhibitors such as tipifarnib have failed to show clinical efficacy as a single agent [Macdonald et al. 2005] or when combined with gemcitabine [Van Cutsem et al. 2004]. It is now known that KRAS may alternatively undergo geranylgeranylation in the presence of tipifarnib, making tipifarnib ineffective. Unfortunately, combined inhibition of farnesyl transferase and geranylgeranyl transferase proved to be too toxic in preclinical studies (Table 3). Other attempts to inhibit KRAS by attempting to block it from reaching the cell membrane and preventing the exchange of GDP for GTP are currently being investigated [Collins Pasca di Magliano, 2014].
MEK/ERK inhibition
The lack of efficacy of direct anti-Ras agents diverted attention to targeting its downstream signaling cascades. Selumetinib is an oral MEK1/2 inhibitor. A phase II trial of selumetinib (AZD 6244) compared with capecitabine in patients who progressed after gemcitabine showed a mOS of 5.4 months in the selumetinib arm compared with 5.0 months in the capecitabine arm, but this was not statistically significant [Bodoky et al. 2012]. Trametinib, a reversible inhibitor of MEK 1/2, was recently approved by the FDA for the treatment of metastatic melanoma. A phase Ib trial of gemcitabine, with or without trametinib, did not show a significant improvement in OS with a mOS of 8.4 months in the gemcitabine plus trametinib arm compared to 6.7 months in the gemcitabine alone arm (p = 0.453) [Infante et al. 2013]; see Table 3. These results suggest that simultaneous inhibition of other signaling cascades, such as the PI3K/Akt/mTOR pathway, may be required to effectively block oncogenic network signaling of KRAS.
AKT
Once activated, Ras phosphorylates PI3K, which then leads to the phosphorylation and activation of AKT, another serine/threonine kinase, the targets of which are involved in cellular growth and proliferation [Berndt et al. 2011]. MK a space between MK and 2206. 2206, an oral AKT inhibitor, is currently being investigated in a phase II trial in combination with selumetinib compared with modified FOLFOX for metastatic pancreatic cancer [Yap et al. 2011].
Developmental pathways
Hedgehog
The Hedgehog (Hh) signaling cascade regulates embryonic development. This pathway is silent in normal pancreatic tissue. However, pathological activation of the Hh pathway is common and shown to be oncogenic in pancreatic cancer [Chen et al. 2002]. Hedgehog binds to the extracellular receptor, Patched, which releases Smoothened, which then acts to activate transcription factors which is thought to be one of the mechanism involved in the development of cancers. Interestingly, Hh signaling in pancreatic cancer is restricted to the stromal compartment and Sonic Hedgehog (SHh) has been shown to produce a desmoplastic reaction in mice, contributing to the maintenance of the tumor microenvironment [Bailey et al. 2008]. The desmoplastic reaction is characteristic of most pancreatic adenocarcinomas and is thought to contribute to the development of metastatic disease, as well as limit the ability of chemotherapeutic drugs to penetrate into pancreatic tissue. In mouse models, inhibition of SHh resulted in improved gemcitabine delivery, depletion of the dense stroma, and increased vascularization of the tumors [Olive et al. 2009], suggesting that this pathway could be an appealing drug target. A phase I trial of GDC-0449 (vismodegib), an inhibitor of the key Hh signaling modulator Smoothened, showed an acceptable safety profile and some antitumor effects in a variety of solid tumors [LoRusso et al. 2011]. A phase II trial is currently open to assess the effectiveness of GDC-0449 in combination with standard chemotherapy in metastatic pancreatic cancer (Table 3). Preliminary data from this trial suggests that vismodegib in combination with nab-paclitaxel and gemcitabine is well tolerated, and more than 80% of the 59 patients have achieved stable disease or better [De Jesus-Acosta et al. 2014]. Unfortunately, another randomized, phase II trial targeting the Hh pathway showed disappointing results. IPI-926, a small molecule Smoothened inhibitor, was given in combination with gemcitabine 1000 mg/m2 IV weekly for 3 weeks with 1 week off, and the trial was closed after preliminary interim analysis showed decreased survival in the IPI-926 plus gemcitabine arm, with median overall survival less than the historical median survival of gemcitabine alone of approximately 6 months.
Notch
Notch signaling is implicated in tumorigenesis and appears to be activated in pancreatic adenocarcinoma [Leach, 2005]. Currently, there is a phase II trial of a Notch signaling inhibitor/gamma secretase in combination with gemcitabine in patients with previously treated metastatic pancreatic adenocarcinoma (Table 3).
Extracellular matrix/stromal microenvironment
Hyaluronan
Pancreatic cancer is uniquely characterized by a strong desmoplastic stroma comprised of a dense extracellular matrix, fibroblasts, inflammatory cells and abnormal vasculature. Stromal depletion strategies such as degradation of hyaluronic acid could potentially allow better penetration of chemotherapeutic agents into tumor sites [Olive et al. 2009]. Currently, there is an active phase II trial investigating the use of PEGPH20, a pegylated formulation of recombinant hyaluronidase, in combination with gemcitabine and nab-paclitaxel for metastatic pancreatic cancer (Table 3), after a phase I study showed promising results [Hingorani et al. 2013]. In the phase Ib study, 28 patients were enrolled and received PEGPH20 plus gemcitabine. Of the 21 patients evaluated, 7 patients had a partial response for an overall response rate of 33%, and 9 had stable disease for more than 2 months.
Angiogenesis
Vascular endothelial growth factor (VEGF) causes the proliferation of endothelial cells, which in turn stimulates neoangiogenesis. The addition of bevacizumb, ablifercept or axitinib to gemcitabine all failed to improve mOS or PFS for patients with advanced pancreatic cancer [Kindler et al. 2010, 2011; Rougier et al. 2013]; see Table 1. TL-118 is an oral medication consisting of a nonsteroidal anti-inflammatory agent, an alkylating agent, a histamine H2 blocker and a sulfonamide with possible anti-angiogenic properties. A phase II trial using a combination of TL-118 and gemcitabine in metastatic pancreatic cancer is currently underway (Table 3).
Heparan sulfate proteoglycans
Heparan sulfate proteoglycans (HSPGs) are polysaccharide molecules covalently bound to proteins associated with the plasma membrane or the basement membranes in cells, including tumor cells [Zhou et al. 2011]. HSPGs are thought to play a key role in the tumor microenvironment by binding to factors that support tumor growth. M402 is a mimetic of heparan sulfate created to inhibit the multiple interactions thought to involve heparan sulfate [Zhou et al. 2011]. A phase II clinical trial is actively recruiting participants to investigate M402 in conjunction with standard chemotherapy (Table 3).
LOX inhibition
Upregulation of 5-lipoxygenase has been reported in several cancer types, including pancreatic cancer [Boger et al. 2012; Ding et al. 1999]. Arachidonic acid is metabolized to leukotrienes and other inflammatory compounds via 5-lipooxgenase. Increased expression of 5-lipoxygenase has been seen in esophageal adenocarcinoma, precancerous colonic adenomas [Wasilewicz et al. 2010], papillary thyroid cancer [Kummer et al. 2012], mantle cell lymphoma [Mahshid et al. 2009], and renal cell carcinoma [Faronato et al. 2007] among others. In in vitro cell models, lipoxygenase (lox) inhibitors inhibit cell proliferation and induce apoptosis [Tong et al. 2012]. Inhibition of 5-lipoxygenase is therefore a proposed therapeutic target in pancreatic cancer. However, a phase II randomized, double blind study comparing LY293111, a LTB4 receptor antagonist, with gemcitabine to gemcitabine plus placebo, showed no difference in 6-month survival (p > 0.2) or PFS (p > 0.05) [Saif et al. 2009].
Immune therapy
Owing to the relatively ineffective treatments using traditional chemotherapeutic drugs, other possible avenues such as immunotherapy are being explored. There is evidence that pancreatic tumors use numerous mechanisms to evade detection by the immune system, such as negatively regulating T-cell responses, secreting factors such as transforming growth factor (TGF)-β and interleukin (IL)-10 that suppress the immune system, and downregulating MHC class I expression [Sideras et al. 2014]. Tumor-specific antigens, such as mesothelin, have also been identified, leading the way for the possible development of a tumor vaccine [Le et al. 2014].
CTLA-4
Ipilimumab is a human monoclonal antibody directed against the cytotoxic T-lymphocyte- associated antigen-4 (CTLA4) found on activated T cells. Binding of ipilimumab to CTLA4 enhances T-cell activation and its antitumor effect [Weber, 2008]. Ipilimumab is currently approved by the FDA for the treatment of melanoma [Hodi et al. 2010]. A phase II study of FOLFIRINOX followed by ipilimumab with an allogeneic tumor vaccine is currently underway in patients with metastatic pancreatic adenocarcinoma (Table 3).
Tumor vaccines
Whole tumor vaccines are promising cancer immunotherapies. Allogeneic pancreatic tumor vaccines are vaccines created from the tumor cells of one patient and given to another patient, with the hope that specific tumor antigens will be expressed and recognized by the new host’s immune system, creating an immune response directed toward the host’s own tumor cells. Currently, the only FDA-approved cancer vaccine is sipuleucel-T for hormone resistant prostate cancer [Kantoff et al. 2010]. CRS-207 is a pancreatic cancer vaccine currently under investigation. It uses a live-attenuated strain of Listeria monocytogenes that expresses mesothelin, a cell surface glycoprotein that is overexpressed in pancreatic tumors. The proposed mechanism of action is that the bacteria will invade phagocytes, produce mesothelin and, in turn, activate cytotoxic T cells against mesothelin, resulting in cell death of the mesothelin-expressing tumor cells. A phase II trial to investigate the use of CRS-207 in conjunction with GVAX, a whole-cell vaccine expressing human granulocyte macrophage-colony stimulating factor, is now recruiting (Table 3). A recently completed phase II trial of 90 patients showed a statistically significant OS benefit in patients receiving the combination of GVAX and CRS-207 immunotherapies compared to patients receiving GVAX immunotherapy alone, with a mOS of 6.1 months compared with 3.9 months, respectively (p = 0.011) [Le et al. 2014].
Tumor-specific antibodies
Yttrium Y-90 clivatuzumab tetraxetan is a radioimmunoconjugate made of a monoclonal antibody directed against the pancreatic tumor antigen MUC 1 conjugated to the chelating agent tetra-azacyclodecanetetra-acetic acid and radiolabeled with the radioisotope yttrium Y90. A phase I trial showed promising activity with a good safety profile [Ocean et al. 2012], and this agent is currently being investigated in a phase III trial (Table 2).
Modified lymphocytes
Another approach to cancer treatment is to use T cells that have been engineered to have a T-cell receptor (TCR) that recognizes a specific antigen by fusing the TCR to the antibody binding domain of an immunoglobulin (Ig). IgCD28TCR is a T cell designed with an Ig portion that recognizes carcinoembryonic antigen (CEA), allowing T cells to recognize and destroy cells expressing CEA. A phase II clinical trial is currently recruiting participants with any CEA expressing adenocarcinoma, including pancreatic adenocarcinoma (Table 3).
Conclusion
Recent developments of new therapeutic regimens have resulted in significant improvement of survival for patients with metastatic pancreatic cancer. The past three decades have seen exciting improvements in the understanding of the basic molecular mechanisms that drive pancreatic carcinogenesis. This has allowed the expansion of treatments beyond chemotherapy to include targeted therapies, expanded drug-delivery systems, and manipulation of the immune system. Now, with the advent of next-generation sequencing, we will be able to achieve a more comprehensive view of the complex genomic landscape of this deadly cancer. Recent exome sequencing of 99 patients with pancreatic adenocarcinoma showed an average of 26 mutations per patient, identifying mutations that will hopefully lead to a better understanding of the molecular pathophysiology of this disease [Biankin et al. 2012]. The four most commonly mutated genes were KRAS, TP53, CDKN2A and SMAD4. Unfortunately, targeting KRAS, as described earlier, has yet to be successful, and attempting to correct the loss of a tumor suppression gene, such as TP53, currently remains unattainable. The exome sequencing of these patients also highlighted the heterogeneity of pancreatic tumors, with a large number of novel mutations at low frequencies, making the likelihood of successfully treating pancreatic cancer by targeting only one genetic aberration at a time low. Importantly, more basic and translational research is needed to elucidate the functional consequences of these many yet understudied intrinsic genetic lesions. Furthermore, the lack of efficacy of many targeted agents in pancreatic cancer, proven to be effective in other cancer types, indicates that pancreatic cancer possesses uniquely challenging characteristics not yet well understood. Therefore, continuing to attack pancreatic cancer from as many angles as possible will likely give the best chance of one day making metastatic pancreatic cancer a curable disease.
Footnotes
Funding
This publication was supported by the Washington University Institute of Clinical and Translational Sciences (grant numbers UL1 TR000448 and KL2 TR000450 from the National Center for Advancing Translational Sciences). The content is solely the responsibility of the authors and does not necessarily represent the official views of the NIH.
Conflict of interest statement
Andrea Teague and Kian-Huat Lim have no conflict of interests to declare. Andrea Wang-Gillam has served as a consultant for Merrimack.