
Abstract
In recent years, growing research interest has focused on the so-called liquid biopsy. A simple blood test offers access to a plethora of information, which might be extremely helpful in understanding or characterizing specific diseases. Blood contains different molecules, of which circulating free DNA (cfDNA), circulating tumor DNA (ctDNA), circulating tumor cells (CTCs) and extracellular vesicles (EVs) are the most relevant. Conceivably, these molecules have the potential for tumor diagnosis, monitoring tumor evolution, and evaluating treatment response and pharmacological resistance. This review aims to present a state-of-the-art of recent advances in circulating DNA and circulating RNA in gastrointestinal stromal tumors (GISTs). To date, progress in liquid biopsy has been scarce in GISTs due to several issues correlated with the nature of the pathology. Namely, heterogeneity in primary and secondary mutations in key driver genes has greatly slowed the development and application in GISTs, unlike in other tumor types in which liquid biopsy has already been translated into clinical practice. However, meaningful novel data have shown in recent years a significant clinical potential of ctDNA, CTCs, EVs and circulating RNA in GISTs.
Keywords
Introduction
Technological advances, particularly next-generation sequencing (NGS), have paved the way to personalized medicine by drastically reducing the time and costs required to assess an individual’s and disease’s genetic make-up. Nowadays, it is indisputable that NGS technology provides the opportunity to look with unprecedented depth into biological samples, identifying low and ultralow frequency DNA variants.1–3 One promising application of NGS technology is liquid biopsy for cancer detection and monitorization towards a personalized cancer-medicine strategy. In recent years, not surprisingly, we have witnessed a growing research interest in liquid biopsy. The term ‘liquid biopsy’, according to the NCI Dictionary of Cancer Terms (www.cancer.gov), is defined as ‘a test done on a sample of blood to look for cancer cells from a tumor that are circulating in the blood or for pieces of DNA from tumor cells that are in the blood’. Indeed, a simple blood test offers access to a plethora of information, which might be helpful in understanding or characterizing a broad spectrum of diseases, including cancer.4,5 Blood contains different molecules, including circulating free DNA (cfDNA), circulating tumor DNA (ctDNA), circulating tumor cells (CTCs), circulating RNA (cRNA) and extracellular vesicles (EVs).6–11 All these molecules together potentially permit the diagnosis of tumors, monitoring their evolution, and evaluating treatment response and drug resistance.6,8,12–14 Consequently, liquid biopsy offers pivotal implications in clinical management, promising to revolutionize the standard management of oncological patients (Figure 1). Specifically, the variety of liquid biopsy applications includes:
- Biological and clinical understanding of the disease
- Risk-based stratification of tumor patients
- Personalization of therapy
- Evaluation of clinical outcome, including therapeutic efficacy assessment.

cfDNA, ctDNA, CTCs, cRNA and EVs
cfDNA and ctDNA
Current evidence points to cfDNA being released during physiological cell functions and refers to DNA fragments outside of cells in different body fluids, including the plasma, serum, urine, and saliva.15,16 The major part of extracellular DNA is adsorbed to the surface of leukocytes or erythrocytes (cell-bound DNA) in the bloodstream.17,18 A portion can be identified in the plasma and it is known as cfDNA. cfDNA has a short half-life and is often heavily damaged, mainly due to its easy degradation by nucleases.15,19–21 cfDNA also includes ctDNA, which is DNA-derived from tumors. 6 The exact mechanism through which ctDNA reaches body fluids is still unclear, although it has been proposed that apoptosis or necrosis of tumor cells, or active secretion from macrophages that have phagocytized necrotic cells, may have a prominent role in this process.9,18,21 DNA concentration in plasma varies greatly from one individual to another; for example, the cfDNA concentration is lower in healthy people than in cancer patients (10–20 mg/ml versus >1000 mg/ml),11,22,23 suggesting that the major contribution is given by ctDNA, while normal DNA only represents a small portion. As a result, ctDNA has emerged during the last decade as a novel and key source of information, profoundly diverse from tissue biopsy. Some key studies, across several cancer types, have also shown that mutations leading to treatment resistance can be detected in ctDNA several months before detection by imaging, suggesting its potential in monitoring drug response.24,25 Finally, liquid biopsy offers repeatability due to its minimally invasive nature, which in turn leads to better acceptance by patients. 19
CTCs
Recently, CTC analysis has become a significant field of study in biomedical research. In particular, CTC detection has emerged as an early marker of tumor recurrence, occurring before clinical symptoms manifestation, in various tumor types.26,27 CTCs are tumor cells that may be released by early tumor lesions or metastases, generating expectations by the research community for the development of a blood-based cancer test. However, CTCs detected in blood are usually in low numbers, being estimated that ~1–10 CTCs per ml of blood released by primary tumors or metastases may be detected in peripheral blood.28–31 Therefore, the development of a reliable CTC-based test for early cancer detection or monitoring cancer progression remains challenging. In addition, CTCs are heterogeneous and may circulate as single cells or clusters of cells, making their use in the clinical setting even more complex. For example, it has been observed that CTC clusters may have a higher metastatic potential and a shorter half-life in circulation.32,33 The majority of CTCs die in the bloodstream due to different causes, including physical and oxidative stress and paucity of growth factors and cytokines. However, the cancer cells that survive can exit the bloodstream and reach the surrounding tissues, where they start to divide and grow.34,35
cRNA
More recently, research in the liquid biopsy field has also focused on cRNAs, which includes mRNA and noncoding RNA (ncRNA). To date, it is well established that cRNAs are crucial mediators in cell-to-cell communication and in the regulation of gene expression and biological functions in recipient cells, thereby acting like hormones.36,37 Similarly to cfDNA, cRNAs are highly vulnerable to degrading enzymes in the bloodstream, such as RNases. Given the critical role of these messengers, cRNA is preserved enclosed in EVs, including microvesicles, exosomes and apoptotic bodies, or complexed with specific RNA binding proteins, such as Argonaute 2 (AGO2), high-density lipoprotein and low-density lipoprotein.7,38–41
According to a length cut-off of 200 nucleotides (nts), ncRNAs encompass two super families: small ncRNAs and long ncRNAs (lncRNAs). Small ncRNAs comprise (1) microRNA (miRNAs) and small interfering RNAs (siRNAs), mediating RNA-silencing at the post-transcriptional level; (2) small nuclear RNAs (snRNAs), regulating splicing; (3) small nucleolar RNAs (snoRNAs), which may affect ribosomal RNA, transfer RNA, and snRNA processing; and (4) P-element-induced-wimpy testis (piwi)-interacting RNAs (piwiRNAs), which regulate chromatin modification and have transposon-silencing capabilities. 36 The lncRNA family comprises ncRNAs that are heterogeneous in both size, from 200 to 10,000 nts, and role. Specifically, lncRNAs may act as regulators of gene expression, as scaffolds for protein binding and as decoys for different RNA molecules, including miRNAs.36,42–44 Additionally, deregulated lncRNA expression has been associated with the development of diseases, including cancer.45–47 Among all these circulating ncRNAs, miRNAs are the most known and well-characterized. miRNAs, at approximately 20–22 nts in length, exert their action as modulators by binding specific seed sequences on the 3′UTR of specific target genes. It has been widely reported that circulating miRNAs are extraordinarily stable in body fluids 48 and the amount and composition of exosomal miRNAs differ between cancer patients and healthy controls, suggesting these miRNAs may represent potential non-invasive biomarkers.49–51 The most recently discovered class are circular RNAs (circRNA), functioning as sponges for miRNAs or proteins. 52 circRNAs generally formed by the alternative splicing of pre-miRNAs, with 3′ and 5′ ends covalently linked, 53 are relatively abundant in exosomes and represent a new frontier in cancer research.54–58
EVs
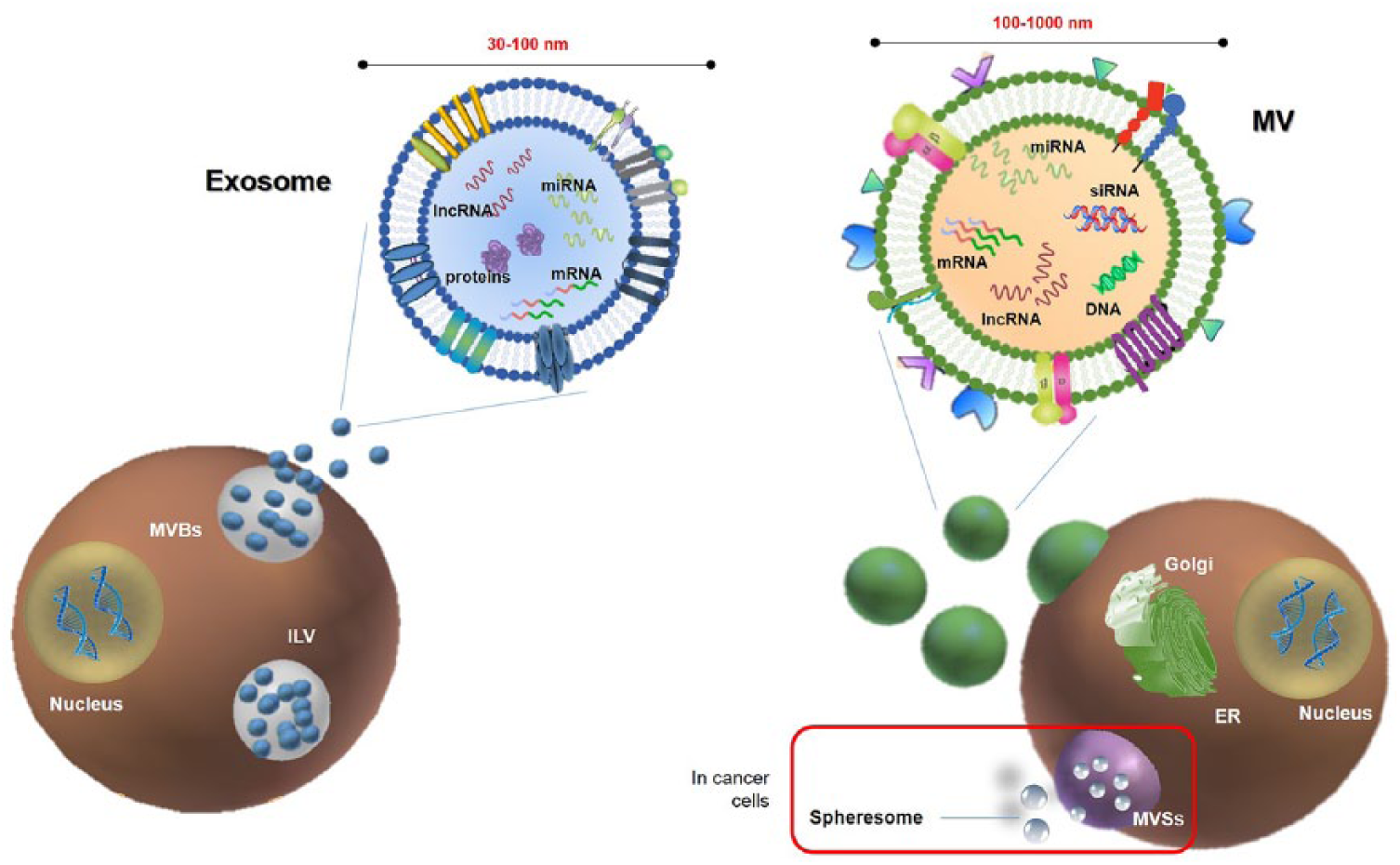
EVs are cell-derived submicron membranous vesicles released into extracellular space.59–61 They are small, lipid-bound particles packaging diverse nucleic acids and protein cargo, which are secreted from cells within normal and pathological conditions. 62 These can be potentially released in all body fluids, including saliva, blood, urine, breast milk and tears. Exosomes are the smallest vesicles, ranging in size from 30 to 100 nm and are generated by exocytosis of multivesicular bodies (MVBs) (Figure 2). 63 Microvesicles (MVs) are larger vesicles with a size spanning between 100 and 1000 nm, formed through a finely regulated budding/blebbing of the plasmatic membrane. MV production is generally low under physiological conditions, whereas tumors excrete them in a high constitutive manner.63–68
Taken together, ctDNA and cRNA offer the chance to gain a time-dynamic picture of the tumor, allowing the following of the eventual progression, pharmacological response or appearance of drug resistance.13,69
This review aims to present a state-of-the-art of the current progresses in ctDNA and RNA findings in GISTs.
Table 1 summarizes the main features of cfDNA, ctDNA, CTCs, cRNA and EVs
Summary of the main features of circulating biomaterials.

CAPP-Seq: cancer personalized profiling by deep sequencing; CNA: copy number aberration; CTC: circulating tumor DNA; DLS: dynamic light scattering; EV, extracellular vesicle; GIST, gastrointestinal stromal tumor; MVs: microvesicles; NGS: next-generation sequencing; OS: overall survival; PCR, polymerase chain reaction; PFS, progression-free survival; qRT-PCR: quantitative-real-time reverse transcription PCR; Safe-SeqS: safe-sequencing system; TAm-Seq: tagged-amplicon deep sequencing; WGS: whole genome sequencing; WES: whole exome sequencing.
Clinical epidemiology of GISTs
GISTs are rare sarcoma with an incidence in Europe of 15–20 cases per million per year. Although GISTs account for fewer than 1% of all gastrointestinal tumors, they constitute the most common sarcoma subtype. 70 KIT or PDGFRA gain-of-function mutations are the key drivers of this neoplasm and are found in approximately 85–90% of GISTs, whereas 10–15% do not present any alteration on these genes and are referred to as KIT/PDGFRA wild-type (WT) GISTs.71–76 KIT/PDGFRA mutant GISTs include a plethora of different primary mutations in well-known regions. Primary mutations in KIT involve exons 9, 11, 13 or 17, whereas exons 12, 14 or 18 are the major hotspots in the PDGFRA gene. Single amino-acid substitutions, in-frame deletions or insertions are the predominant mutations types regardless of the gene and the exons. The development of tyrosine-kinase inhibitors (TKIs), such as first-line imatinib, revolutionized GIST management in the early 2000s through specific targeting of KIT/PDGFRA molecular drivers. However, the majority of GIST patients experience disease progression associated with the acquisition of secondary KIT/PDGFRA alterations; alternatively, the involvement of pharmacogenetic and epigenetic mechanisms on imatinib resistance has been investigated, without conclusive results.75–80 To overcome the loss of imatinib response, the multikinase inhibitors sunitinib and regorafenib have been introduced successively as standard second- and third-line treatments, adding clinical benefits to GIST patients.81–85 The emergence of new studies, together with the implementation of cutting-edge technologies in the field, highlights that the ever-increasing complexity in GIST molecular biology challenges the success of consecutive lines of treatment. 86 In the light of this complexity, liquid biopsy could emerge as a windfall in the near future. To date, progress in liquid biopsy in GISTs have been hampered mainly by the heterogeneity of primary and secondary mutations in KIT and PDGFRA receptor tyrosine kinases.87,88 Indeed, this heterogeneity in mutational hotspots has slowed down liquid biopsy development and clinical use in GIST patients, unlike in other tumors such as lung cancer, in which it is being successfully implemented. 89 Given this assumption, in the following sections, we will analyze the most recent findings in liquid biopsy, considering both cDNA and cRNA in GISTs.
ctDNA and cfDNA in GISTs
The majority of reports are focused on primary and secondary KIT alterations, and aim to develop ctDNA as a novel biomarker to help clinicians in management of GIST patients. The first reported evidence for liquid biopsy in GISTs was presented at the 2013 ASCO Annual Meeting. 90 In this study, Demetri and colleagues analyzed both plasma and tissue DNA from a subgroup of GIST patients with advanced disease following imatinib and sunitinib failure, enrolled in the phase III GRID study. Specifically, the authors compared DNA mutational status (performed by Sanger sequencing) from archival tumor tissues with plasma samples (analyzed with bead emulsion amplification and magnetics; BEAMing). The analysis showed an 84% overall concordance in detection of primary KIT exon 9 and 11 mutations between tumor tissue and plasma. In particular, the concordance was 100% for KIT exon 9, but only 79% for KIT exon 11. Remarkably, BEAMing detects more frequently KIT secondary mutations in plasma (47%) compared with tumor tissue (12%). Overall, this represents the first report validating the feasibility of plasma-based ctDNA analysis in GISTs. In the same year, Maier and colleagues reported the results from patients enrolled in the NCT01462994 trial. 91 This study aimed to detect KIT and PDGFRA mutations in cfDNA in plasma from GIST patients with known activating KIT/PDGFRA mutations in tumor tissue, regardless of disease status and planned treatment. 92 Specifically, the authors evaluated 291 plasma samples from 38 GIST patients using 25 different allele-specific ligation (L)-polymerase chain reaction (PCR) assays covering common KIT/PDGFRA mutations. Mutations were detected in 15 patients, 9 having active disease (i.e. having at least one progressing lesion or responding to treatment) while the remaining 6 were without evidence of residual disease after surgery. Interestingly, the authors observed dynamic changes in mutant/wt allele ratios correlated with the course of the disease. 92 For instance, they showed a decrease in mutant cfDNA or negativization in patients responding to TKIs. Of note, all six patients with no evidence of disease had a high (n = 5) or moderated (n = 1) risk of relapse (Miettinen criteria), emphasizing that mutant cfDNA might also serve as tumor-specific biomarkers for the early prediction of recurrence in localized GISTs. Despite these promising data, reports on liquid biopsy in GISTs are still relatively limited (Table 2).
Summary of the studies performed in GIST patients and included in the review.

BEAMing: bead emulsion amplification and magnetics; cfDNA: circulating free DNA; ctDNA: circulating tumor DNA; ddPCR: digital droplet PCR; FFPE: formalin-fixed paraffin-embedded; GIST, gastrointestinal stromal tumor; PCR, polymerase chain reaction; qRT-PCR: quantitative-real-time reverse transcription PCR; NGS: next-generation sequencing; TKI, tyrosine-kinase inhibitor.
Following the work by Maier and colleagues, Yoo and collaborators assessed circulating biomarkers in TKI-refractory GIST patients recruited in a single-arm phase II trial using dovitinib. 93 BEAMing analysis of ctDNA identified primary kinase mutations in 16.7% of the patients; these mutations were 100% concordant with the results observed in the corresponding tumor tissue. 51 The detection of primary mutations was relatively low, compared with secondary KIT/PDGFRA mutations. This result is not surprising considering that BEAMing better detects predesigned point mutations, common as secondary mutations, rather than the complex KIT primary mutations in exon 11. Subsequently, Bauer and collaborators reported additional results on liquid biopsy in GISTs at the 2015 ASCO Annual Meeting. In particular, they prospectively collected 30 plasma and 15 matched tumor samples from 22 metastatic GIST patients. 94 Using a custom-designed targeted sequencing panel in an Illumina Miseq platform, they detected a total of 87 nonsynonymous KIT mutations in plasma samples. Primary mutations, all matching tumor analysis, were identified in 41% of GIST patients; resistance mutations were observed in 86% of GIST patients, although they were also observed in patients responding to imatinib. 94 Recently, Kang and collaborators, using NGS, provided more data from plasma samples through the monitorization of three GIST patients under TKI treatment. The authors analyzed tumor mutational status in baseline tumor biopsies and plasma samples collected during the follow up. 95 Additional mutations in plasma emerged in those patients who had a partial response or progressive disease, whereas they kept detecting only the primary mutation in the patient with stable disease. 95 The study had important limitations, such as the lack of plasma samples with matched biopsies and the absence of NGS data confirmation with a different technique. Particularly, considering that KIT and PDGFRA mutations are mutually exclusive, we may assume that the presence of a secondary PDGFRA mutation on a patient harboring a clonal KIT primary mutation is an artefact derived from the NGS methodology. Nevertheless, NGS applications hold the pivotal advantage to detect novel secondary mutations conferring resistance. Therefore, it may represent an enrichment for future studies or clinical trials of novel/repositioned/existing drugs specifically targeting secondary mutations. In the wake of this idea, Wada and coworkers investigated four imatinib-resistant GIST patients, who underwent surgical resection. 96 In particular, the authors analyzed, through an NGS approach, mutations in tumor tissue from resected primary and imatinib-resistant lesions and in ctDNA isolated before and after imatinib treatment. All the four patients had a primary KIT exon 11 lesion with deletions involving codons 550 to 559. Patients with imatinib-resistant lesions had resistance mutations in the KIT exon 13 (n = 3) and exon 18 (n = 1); the same genetic alterations were measured in ctDNA.
The non-invasive detection of mutations is pivotal for the selection process of target agents. Indeed, the efficacy of sunitinib correlates with the secondary mutation genotype; specifically, sunitinib is more effective in KIT exon 13 or 14-mutant GISTs.95,102 With regard to the third-line treatment, regorafenib, the GRID study reported the same benefits for patients harboring the most common primary KIT mutations. More recently, the study by Ben-Ami and coworkers suggested regorafenib provides long-term benefit in metastatic GIST patients with KIT exon 11 primary mutations and WT for KIT/PDGFRA.80,83 Overall, it is clearly important to know the tumor secondary mutational status to predict the efficacy of TKIs in imatinib-resistant GISTs. Wada and collaborators evaluated also the cfDNA as a surrogate biomarker of response. Indeed, in the literature, there are different reports evaluating its feasibility in this context. 103 The study by Wada and colleagues, also reported that cfDNA decreased marginally with treatment in two patients, while another patient with stable disease exhibited a substantial increment in the cfDNA concentration. These data pinpoint that the concentration of cfDNA might not accurately reflect tumor evolution. 96 However, we should not under-evaluate that specific tumor markers may be predominantly present in the cell-bound rather than in the cell-free fraction. 104 This issue should be considered with caution as tumor treatment often influences leukocytes or erythrocytes apoptosis, with consequent release of cell-bound DNA into plasma. Therefore, an increase in some markers will be a clue to blood cell death, rather than reflecting tumor growth. Actually, the work by Wada and colleagues in one patient following surgery of primitive lesion, showed that cfDNA increased substantially, while ctDNA was below the threshold of detection before recurrence. After progression of the imatinib-resistant lesion, ctDNA increased and then returned to the value below the threshold following sunitinib treatment, while cfDNA was constantly at high levels. In this regard, ctDNA may be a better biomarker compared with cfDNA. 96 Nonetheless, this has to be taken with caution as ctDNA may reflect a mixed population: it can derive from dying tumor cells responding to therapy or from tumor cells resistant to therapy. 18 Unfortunately, to date, no further reports focusing on the impact of resistance mutations have been published. Taken together, the data led us to speculate on the importance of liquid biopsy to follow the tumor evolution under TKI treatment. However, the available literature is still too scarce, and additional prospective investigations recruiting a major number of patients are critical before its translation into clinical practice in GISTs.
More recently, three papers have focused their attention on the detection of primary mutations in GISTs. In the first of these works, Kang and colleagues 97 analyzed plasma samples, collected before surgery, from 25 patients with localized gastric GISTs. This is one of the few studies addressing the role of ctDNA detection in localized GISTs. The standard treatment for localized GISTs is complete surgical resection; however, mutational status is important for the indication of adjuvant or neoadjuvant imatinib therapy, and occasionally helps in the diagnosis of GISTs. However, tumor tissue samples before surgery can be inadequate for standard mutation analysis. In this context, liquid biopsy may have the potential to detect primary mutations prior to resection. In addition, presence of mutant ctDNA after surgery might allow assessing microscopic residual disease, possibly responsible of recurrence, and guiding adjuvant therapy recommendation. Mutational status of the paired plasma-tissue samples were investigated through Sanger sequencing (tissue) and an NGS panel covering KIT exons 9, 11, 13, 17 and PDGFRA exon 18 (plasma). A total of 18 out of 25 GISTs were KIT exon 11 mutants, and the remaining were KIT/PDGFRA WT. The reported concordance between plasma and tissue samples was 72%, with 13 patients identified as KIT exon 11 mutants in plasma. None of the seven KIT/PDGFRA WT patients had measurable mutations in the plasma DNA. 97 In a subsequent study, Boonstra and collaborators showed digital droplet PCR (ddPCR) may be useful in the detection of common KIT exon 11 mutations in both GIST tumor tissue and ctDNA. 98 In particular, the authors used an in-house designed single ddPCR assay covering two hotspots in exon 11. According to COSMIC, around 80% of the mutations in this exon cluster in two hotspot regions of approximately 25 bp within a 100 bp range from each other. 105 The authors first validated ddPCR in 36 pretreatment biopsies of GIST patients previously tested via Sanger sequencing or NGS. A total of 27 patients were KIT exon 11 mutants, whereas 9 had no KIT exon 11 mutations and served as negative controls. ddPCR resulted in 100% of specificity since all controls turned out to be negative, and in 77% of sensitivity, detecting 21/27 mutations. However, five mutations were located within the annealing sequence of the primers; one of the five samples had a duplication that was considered negative even characterized by a typical pattern of droplet distribution. Considering the remaining 22 samples covered by ddPCR, only 1 with a single nucleotide variant located within the detection range of probe 2 was a true false-negative tumor, and therefore the assay showed an overall sensibility of 95% for the regions covered in KIT exon 11. Subsequently, the ddPCR assay was tested on plasma samples available before and at multiple time points during imatinib therapy for 14 GIST patients with metastatic disease and 8 with localized GISTs. All the 22 patients had measurable disease before collection of the first (baseline) plasma sample. Analysis of the baseline plasma sample highlighted the presence of a KIT exon 11 mutation in 13 of 14 metastasized patients, and only in 1 of 8 with localized disease. The authors also used ddPCR to monitor the treatment response in serial plasma samples from 11 metastasized GISTs under TKI treatment. They showed a decrease in KIT exon 11 mutant ctDNA during treatment, which was in agreement with radiological treatment response or stable disease, evaluated according to RECIST criteria. 98
More lately, Namløs and colleagues applied an NGS approach to analyze ctDNA samples from 44 treatment-naïve GIST patients (n = 35 KIT and n = 9 PDGFRA mutants). 99 Somatic mutations in ctDNA were found in 36% of the plasma samples (n = 16 patients). The ctDNA detection rate was higher for KIT mutants (42.8% mutants detected) compared with PDGFRA mutant GISTs (11.1%). In addition, plasma from high-risk patients or with metastatic disease showed more frequently detectable mutations in ctDNA compared with patients with localized or intermediate to low-risk GISTs. Furthermore, the authors showed that ctDNA detection in patients undergoing TKI treatment might be related to disease development. Indeed, analysis on six KIT mutant GISTs receiving TKIs at the time of blood collection, revealed the presence of ctDNA in patients with progressive disease; no mutations were observed in patients with stable disease.
CTCs in GIST
Research data on CTCs in GISTs are very scarce, and currently, only one study has been published in the literature. 100 In particular, Li and collaborators investigated the feasibility of detecting ANO1 (known as DOG1) expression in peripheral blood mononuclear cells (PBMCs) of GIST patients. ANO1 is, together with KIT, a diagnostic biomarker in GISTs. A total of 54% of the patients analyzed were ANO1-positive and a higher expression was significantly associated with a larger tumor size, high mitotic count and risk. The authors investigated also the prognostic role of ANO1. In particular, ANO1 expression was tested in 112 before and 4 weeks after surgical resection. A total of 51.8% of patients were ANO1-positive pre-resection, and only 12.1% (n = 7) of them turned out positive after surgery; these patients were characterized by liver metastasis. Afterwards, ANO1-positive status emerged in 21 GISTs experiencing recurrence after surgery. Finally, the authors evaluated imatinib efficacy after 3 months of neoadjuvant treatment in 26 GIST patients, preoperatively treated with TKIs. ANO1 expression was tested in PBMCs pre and post imatinib treatment. The 17 patients with disease control (partial response or stable disease) showed a reduction trend of ANO1 expression and 10 patients became negative, whereas the expression level did not change in the 9 patients with progressive disease. Despite the limitations of the study, including the sample size, these results showed that CTC detection in PBMCs by quantifying ANO1 could be taken into account and may offer an interesting opportunity to monitor the disease course as well as the clinical response to imatinib. 100
Circulating vesicles and RNA in GIST
If the literature on circulating DNA in GISTs is quite scarce, reports on the different molecules are anecdotal, representing a new, valid and largely unexplored field of investigation. Up to now, the majority of the studies focused on circulating vesicles. The first evidence of exosome release in GISTs dates back to 2014, when Atay and collaborators investigated the role of exosomes in mediating the complex interplay between the tumor and stroma during disease progression. 101 In particular, they selected the human cell line GIST-T1 as an in vitro disease model, expressing the most common type of mutation involved in GIST pathogenesis (i.e. KIT exon 11). The authors showed GIST cells secreted high number of exosomes, or ‘oncosomes’, carrying the activated oncogenic KIT receptor. Interestingly, the authors reported that the invasion of stromal cells, through these specific exosomes, led to the production of interstitial cells of Cajal (ICC)-like cells. Indeed, these oncosomes act like phenotypic modifiers of their microenvironment, promoting tumor progression through the regulation of downstream KIT-signaling pathways in stromal cells, which differentiate to ICC-like cells. Moreover, conditioning with GIST-T1-derived exosomes promotes enhanced secretion of the matrix metalloproteinase (MMP) 1, which is recognized to dynamically contribute to tumor cell invasion. 101 Even if the authors could not prove the direct contribution of KIT in this process due to methodological issues, these preliminary data indicate that tumor transformation in not solely driven by oncogenes but other factors are involved. Indeed, the selective blocking of MMP exosome-mediated, MMP-1 secretion abrogated tumor invasiveness. In other words, this first report highlighted the existence of a feedback loop between a signaling mediated by the exosomes and matrix MMPs and suggests a potential role for exosomes as stroma-modifiers. 101 Subsequently, a work by Junquera and collaborators, described for the first time multivesicular sphere (MVS) production in GIST cells in vivo. 106 Specifically, MVSs are spherical membrane structures produced through a budding process from the plasma membrane, containing many MVs referred to as spheresomes. Interestingly, spheresomes are different from exosomes, and represent a novel mechanism coming from a spherical membrane structure. Analyzing eight gastric biopsies from GIST patients, MVSs containing spheresomes were observed establishing interactions with cytoskeleton filaments and the extracellular matrix. In particular, once in the extracellular matrix, medium MVSs can release the spheresomes (remaining empty) or cross the wall of blood vessels near cancer cells, entering the circulation. This last observation contributes to strengthening the evidence that tumor-derived EVs, besides stimulating cells at distant sites in the organism, play a key role in the initiation of the metastatic niche. The idea is that tumor-derived EVs give rise to the receptive microenvironment supporting the cell arrival, engraftment and survival in the metastatic site.106,107 In addition, Junquera and colleagues observed a considerable variability depending on the tumor sample; in particular, early stage tumors (<4.5 cm and low mitotic activity index) secrete a high number of spheresomes, while tumor with high mitotic activity do not show a presence of spheresomes. This suggests that exacerbation of a specific communication process between mesenchymal cells within tumors could occur, facilitating growth or metastases. 106 Therefore, MVSs may represent a novel and alternative approach to cancer treatment in which MVSs are important therapeutic targets, in a strategy aimed at neutralizing or trapping, thus preventing the signaling process they initiate. After these preliminary studies, the most recent data in GISTs were presented, this year, by Atay and collaborators. 108 In this work, they performed a comprehensive vesicular proteome profiling of GIST-derived exosomes (GDEs), from two GIST cell lines (GIST-T1 and GIST-882), providing important information on the content, biological role and therapeutic value of these vesicles. Specifically, authors showed that GIST cell lines are characterized by an inherent overactive exosome production mechanism, leading to their release and accumulation. Proteomic analysis showed that total exosomal protein content was significantly higher in GDEs compared with the non-transformed primary myometrial smooth muscle cells, representing the host healthy cells surrounding the tumor in vivo. In particular, the authors identified a core of 1060 proteins supporting the exosomal origin (e.g. features shared with exosomes-derived from other cells types), while maintaining the tumor identity. Specifically, the core protein was enriched in diagnostic markers and other features related to GISTs as well as novel kinases, phosphatases and tumor-associated antigens, previously unreported in GISTs. Interestingly, among the markers, the authors showed an enrichment of the markers of autophagy, which is involved in GIST survival and progression (for a review see Ravegnini and colleagues 109 ). An added value of this work is the evaluation of selected GDE-associated core protein in clinical specimens, with the capture and isolation, of KIT positive (KIT+) exosomes from the plasma of GIST patients (n = 18) and healthy donors (n = 12). In this preliminary analysis, Atay and colleagues showed that the number of KIT+ vesicles in controls was small, suggesting the majority of them in GIST patients originate from the tumor. 101 This concept was further supported by the correlation between circulating KIT+ levels with tumor burden and treatment response. Indeed, the authors observed that accumulation of circulating KIT+ exosomes was: (1) enhanced in the peripheral blood of patients with metastatic GISTs compared with primary disease, and (2) decreased in patients responding to treatment. In view of these considerations, quantitative changes in exosomes might represent a tool to predict malignant capabilities (e.g. recurrence or metastasis) and response to therapy. Overall, the results of this comprehensive proteomic analysis of exosomes secreted by GIST cells have unveiled different clinically relevant candidates to be circulating diagnostic and monitoring-disease biomarkers. Nevertheless, despite an in-depth examination of the proteome of isolated KIT+ exosomes holding great promise, the feasibility of the analysis remains to be elucidated.
To date, no additional studies in GISTs described these or additional kinds of circulating molecules. In particular, the literature on circulating miRNAs or lncRNAs is missing, leaving many questions unanswered on their potential role in tumor progression and metastasis, as well as in TKIs response.
A small number of studies on miRNAs and lncRNAs, limited to tissue GISTs (for a review see Nannini and colleagues 110 and Kupcinskas 111 ) have showed a few miRNAs and lncRNAs involved in regulating several genes and biological processes in GIST pathogenesis; however, up to now, none of these have been translated to the clinic or obtained from the bloodstream. Nevertheless, in the near future, molecular investigation of miRNA and lncRNA could represent interesting circulating candidates as prognostic, diagnostic and disease monitoring biomarkers.
Liquid biopsy in GISTs: clinical utility and challenging issues
Liquid biopsy has demonstrated to be a valuable tool, and recent technological innovations are generating promising clinical results, suggesting that liquid biopsy might be incorporated into clinical practice in the near future. This is the case of ctDNA analysis in non-small cell lung carcinoma and CTCs analysis in breast and colon cancer.112–115 However, for other tumors, liquid biopsy is still a wish, highlighting a great lack of homogeneity between the various types of cancer patients. In this context, GISTs, despite the attractive biology based on a few driver mutations, are among the tumors in which the advances in liquid biopsy are very limited. Certainly, even if the studies so far reported do not permit drawing any definitive conclusion, some individual cases underscore that liquid biopsy may be useful in monitoring the clinical response to TKIs in GISTs. The development of resistance mutations is the main mechanism of acquired resistance to TKIs, found in 80–90% of patients experiencing disease progression.87,116,117 Therefore, the prompt identification of these mutations might be clinically relevant to drive therapeutic decision-making. On the other hand, the application of liquid biopsy to improve GIST early diagnosis appears to be challenging. In particular, the heterogeneity of primary mutations in KIT or PDGFRA and the relative paucity of circulating elements in the bloodstream clearly impairs the sensitivity. Moreover, the lack of standardized methods of analysis realizes that we are still far behind in the application of liquid biopsy in GISTs. Therefore, in order to broaden the knowledge and application of liquid biopsy in early diagnosis and prognosis, methodological issues need to be addressed. In this regard, KIT exon 11 mutations, accounting for approximately 90% of KIT mutations, vary remarkably in length and location; consequently, their detection in plasma, through PCR-based methods is quite problematic. 94 Great enthusiasm has emerged regarding NGS applications, and their ability to identify low and ultralow frequency mutations, although this approach involves inherent experimental errors. Indeed, even for methods with the lowest reported error rate, thousands of false positive variants are possible in a fully sequenced human genome. 118 Errors can result from bioinformatics analysis and experimental process (e.g. sample or library preparation and sequencing chemistries). Experimental errors can be reduced through confirmatory sequencing studies, in a manner independent of the algorithms and chemistries used. Nevertheless, NGS applications hold the pivotal advantage of reducing false-negative results, compared with BEAMing and allele-specific L-PCR, which are certainly limited by the identification of predesigned mutations conferring resistance. In view of this consideration, overcoming this limitation with novel NGS techniques is mandatory. Actually, optimizing target mutation profiling is beneficial for patients, as the identification of known and novel resistance mutations may help in selecting optimal responders for molecular therapies.
Conclusion
The concept of ‘oncogene addiction’ was first introduced in the late 20th century to describe the constitutive activity of specific activated/overexpressed oncogenes needed for the continuous maintenance of the malignant phenotype. 119 Afterwards, it did not take long to realize that drugs, specifically targeting hyperactivated oncogenes, could selectively kill cancer cells. Overall, this finding paved the way to the era of precision medicine and targeted therapy, which are based on correct patient selection. The study and understanding of biological processes underlying tumor development and progression have deeply changed cancer treatment, as witnessed in GISTs. In the early 2000s, imatinib revolutionized the field of targeted treatment, particularly in a disease in which no effective treatments were available at that time. The identification of a specific gene status (KIT and PDGFRA mutations) in a precise tumor type (GISTs) enables the selection of patients for targeted therapies. In this panorama, it is extremely important to have tools available for early diagnosis, improving the prognosis, for real-time monitoring of the disease, and ultimately the survival rate.
Currently, tissue biopsy represents the gold standard for a precise diagnosis of cancer; however, this approach suffers from several limitations, summarized in Figure 3. In view of these limits, there is an urgent need of minimally invasive techniques allowing a strict patient follow up at different time points; here originates the concept of liquid biopsy. The development of a ‘liquid biomarker’, which can be easily isolated from any body fluids, represents a great opportunity for early diagnosis and drug response monitoring. Despite the promising expectation, the research is still in its embryonic phase. Indeed, we can list a series of pros and cons (Figure 3) related to liquid biopsy, whilst for some circulating components, such as exosomes, we are even far from clinical applications.
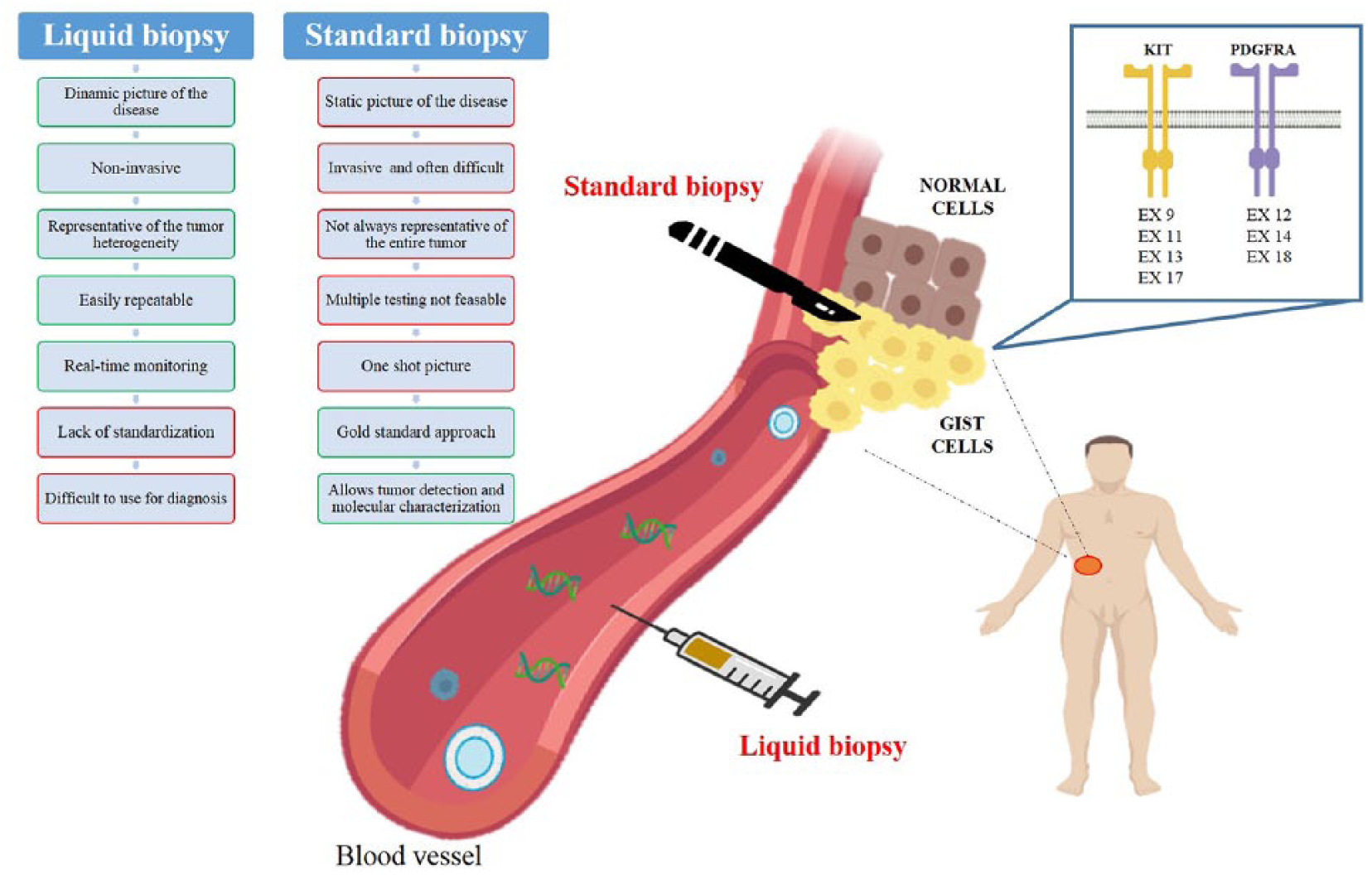
Pros and cons of liquid and standard biopsy in GIST.
In conclusion, liquid biopsy has entered the scene of the era of personalized medicine, representing a key tool to complement the other available techniques routinely used in the clinic. With regard to GISTs, a global effort should be considered as mandatory to translate the use of liquid biopsy into the clinic.
Footnotes
Funding
Gloria Ravegnini is supported by an MSD Italia fellowship granted by and on behalf of Merck Sharp & Dohme Corporation and L’Oréal-UNESCO for Women in Science. Giulia Sammarini is supported by Fondazione Famiglia Parmiani. This work was supported by the Ministry of Education, University and Research of Italy (MIUR, grant number 2015Y3C5KP_002 to SA).
Conflict of interest statement
The authors declare that there is no conflict of interest.