
Abstract
Over the past decade, the detection and analysis of liquid biopsy biomarkers such as circulating tumor cells (CTCs) and circulating tumor DNA (ctDNA) have advanced significantly. They have received recognition for their clinical usefulness in detecting cancer at an early stage, monitoring disease, and evaluating treatment response. The emergence of liquid biopsy has been a helpful development, as it offers a minimally invasive, rapid, real-time monitoring, and possible alternative to traditional tissue biopsies. In resource-limited settings, the ideal platform for liquid biopsy should not only extract more CTCs or ctDNA from a minimal sample volume but also accurately represent the molecular heterogeneity of the patient’s disease. This review covers novel strategies and advancements in CTC and ctDNA-based liquid biopsy platforms, including microfluidic applications and comprehensive analysis of molecular complexity. We discuss these systems’ operational principles and performance efficiencies, as well as future opportunities and challenges for their implementation in clinical settings. In addition, we emphasize the importance of integrated platforms that incorporate machine learning and artificial intelligence in accurate liquid biopsy detection systems, which can greatly improve cancer management and enable precision diagnostics.
Keywords
Introduction
Liquid biopsies involve the collection of small volumes of biofluids to examine cancer cell-derived components. Blood, saliva, urine, and cerebrospinal fluid are rich sources of cancer biomarkers either existing in free form or are associated with other structures secreted in the fluids. 1 Liquid biopsy has significant advantages over traditional tissue biopsies in being minimally invasive and allowing for dynamic analysis and real-time monitoring of tumor progression and treatment response. 2 In addition, liquid biopsies have shown a superior representation of intratumoral heterogeneity when compared to tissue biopsies and are appropriate for longitudinal tracking of cancer development as well as identifying tumor cells that confer resistance.1,3 Dynamic investigations of molecular or cellular biomarkers are made more accessible by liquid biopsy. The liquid biopsy allows for accurate early-stage diagnosis, prognosis, surveillance of disease progression, assessing the efficacy of targeted treatments, and identifying therapeutic objectives for drug development. 4
The liquid biopsy also makes dynamic investigations of molecular or cellular biomarkers easier. Studies have established specific biofluid components which are vital for early-stage cancer detection, namely circulating tumor cells (CTCs) and ctDNA.5–7 Systems that characterize and analyze these components in patients’ biofluids facilitate monitoring cancer development. Components like CTCs and ctDNA are shed from the primary tumor site and enter the bloodstream, thereby contributing to the spread of malignancy.2,3,8 However, their low concentration (1–1000 CTCs per mL) and high degradability make them challenging to detect and analyze. 9 Furthermore, the morphological resemblance of CTCs to some WBCs, phenotypic heterogeneity, and epithelial-to-mesenchymal transition (EMT) represents a significant challenge for any isolation and characterization approach in cancer research. 10
Numerous enrichment, isolation, and characterization platforms for circulating biomarkers have emerged over the last decade. Each offers a unique biophysical strategy (size, density, electrical charge, and membrane markers) to facilitate high sensitivity, selectivity, and specificity of liquid biopsy components and their subsequent downstream molecular characterization. 11 The ideal liquid biopsy platform can isolate and detect the maximum CTCs from a small sample volume while maintaining a high recovery rate. The platforms must also be user-friendly and completely automated, requiring minimal sample preparation.11,12 This review explores novel strategies that allow for high-throughput enrichment, isolation, recovery, and characterization of CTCs and approaches for sensitive detection, amplification, and analysis of ctDNA in multiple cancers. The study presents a broad comparison of CTC and ctDNA analysis strategies, including developing microfluidics-based systems and comprehensive molecular analysis approaches toward effective cancer diagnosis. The operational principles of these systems are discussed, comparing their effectiveness as liquid biopsy systems and exploring future directions and opportunities for developing sensitive, reliable liquid biopsy platforms.
Current technologies for CTC and CTC clusters isolation
Microfluidics has shown potential in developing reliable cancer diagnostics, particularly in clinical point-of-care testing. 13 The design and geometry of these devices are influenced by their intended application, including biological features of targeted cells and particles within biofluids like size, density, deformability and compressibility, electrical, and hydrodynamic properties. In this study, we have categorized the microfluidic techniques based on their key functional concept (Table 1). This includes size/deformability-based, hydrodynamics-based, electric-based, and acoustics-based microfluidics. Microfluidics-based CTC isolation is also done using affinity-based techniques in which cells are captured based on their surface protein expression levels involving the use of relevant antibodies or aptamers, allowing the selection of cancer-specific biomarkers (Figure 1).
The most used circulating tumor cell (CTC) isolation systems, and their advantages and disadvantages.


Schematic depicting the various strategies for separation and detection of circulating tumor cells (CTCs) and CTC clusters based on differences in their physical and biological features. Techniques such as density gradient, filters, electrophoresis, and microwells exploit the unique biophysical properties of CTCs to isolate them from peripheral blood. Positive/negative selection exploits the unique biological expression profile of CTCs and clusters for isolation and analysis.
Size/deformability-based technique
Filtration is a microfluidics-based technique for cell separation by size and deformability differences between blood components, such as RBC, WBC, and CTCs. Microstructure post filters, microporous membranes, and microfluidic constrictions are the most commonly used microfluidic microfiltration techniques. Different shapes of microfluidic post-filters have been explored to achieve maximum CTC capturing efficiency from blood samples, which include funnel constrictions, micro-elliptical posts, and micropillars. Recently, micro-elliptical posts have been implemented to capture CTCs in both whole and lysed blood samples. 26 The smooth circular micro-elliptical posts were arranged with gradually reduced microfluidic gaps, leading to minimal cell damage while maintaining higher cell viability. From 2 to 3 mL of metastatic breast cancer and non-small-cell lung cancer (NSCLC) samples, the capturing efficiency was ~90%, and cell viability of 96%. However, the major disadvantage of this system is the limited recovery rate which hinders its downstream analysis.
Clogging is another challenge, resulting in additional workload and hampering the analysis of samples. The study took advantage of ratcheting mechanisms in the microfluidic device and captured 77−90% of CTCs from whole blood, despite the relatively similar size of sample components. The captured CTCs are also available for downstream characterization as the restoration process can be conducted. In addition, 20 blood samples from prostate cancer patients were used to test the device, and the results were compared with those of the CellSearchTM system. Despite the microfluidic device’s high separation precision and sensitivity, its poor throughput prevents it from processing the usual volume of 7.5 mL of the blood sample.27,28
Microporous membranes are another microfluidic filtration strategy that has achieved comparatively high throughput (>3 mL/h). 29 In this approach, size-selective microcavity arrays with differential cavity shapes (circular, rectangular, and pyramidal) are employed to isolate CTCs. 30 Hosokawa et al. developed an integrated microfluidic device with a modified circular microcavity array enabling enrichment, staining, and restoration of CTCs from blood samples. The device capturing efficiency for 1 mL blood sample spiked with 10–100 lung carcinoma NCI-H358 cells was 97%, with a viability of ~98%. By increasing the number of occupied microcavities, the flow resistance became higher, which caused cell deformation and CTC loss and decreased the capture efficiency.
Rectangular-shaped microcavities were designed to optimize CTC capturing efficiency using this method to capture smaller CTCs. This device captured around 80% of the small-cell lung cancer (SCLC) (NCI-H69 and NCI-H82) cells spiked in a 1 mL whole blood sample. In a patient sample, Hosokawa et al. detected CTCs in 17 out of 22 NSCLC patients utilizing a microcavity system. They could also detect CTCs in 20 out of 21 SCLC patients. 31 In addition, changing the shape from circular to rectangular reduced the number of captured leukocytes, thereby diminishing a significant number of leftover leukocytes. In a study, the clinical application of rectangular microcavities detected CTCs in all samples (16 of 16). 32 While the system demonstrated superiority over the CellSearch™ system toward the detection of CTCs in patients with NSCLC, the sensitivity was comparatively poor for SCLC samples. The size-based separation inevitably resulted in the loss of smaller size SCLC cells and compromised the CTC isolation and detection sensitivity. 33
Yin et al. developed a new microfluidic device integrated with pyramidal-shaped microcavities for better CTC enrichment with fewer leftover leukocytes. This device consisted of two polydimethylsiloxanes (PDMS) layers on the top and bottom of the pyramidal microcavity arrays made by standard photolithography. The gradual increase in the entry size of the channel and the pyramidal shape of cavities allowed for reduced clogging and draining of blood cells. At a flow rate of 6 mL/h, the device could capture 80% of the spiked CTCs from 1 mL of whole blood. 34 Despite all the improvements made in the microcavity array capturing technique, the efficiency of small CTCs capturing is still low and requires further optimization and advancements. 35 Studies have also explored strategies that enable high-efficiency capturing of CTCs while maintaining minimal contamination from RBCs and WBCs. Yoon et al. introduced a microfluidic device with slanted weir microchannels to separate invasive breast cancer cells. The results reported in the study revealed a high capturing efficiency of 97%, but smaller cancer cells (<350 μm2) were found in both waste and target outlets, making the device unsuitable for capturing small CTCs. 36
Generally, size-based systems need a considerable volume of blood and might not be able to trap the smaller CTCs than WBCs, as the main limitations. Furthermore, these methods are typically inefficient in purity and lack specificity, although the cost of applying them is relatively inexpensive. 37
Hydrodynamic-based technique
In contrast to microfiltration systems, hydrodynamic-based CTC isolation does not rely on physical barriers, thereby reducing the chance of clogging and increasing the throughput and viability rate. This method processes samples at high flow rates to generate the hydrodynamic forces that separate cells based on size. 10 Deterministic lateral displacement (DLD) and inertial microfluidics are the most popular hydrodynamic-based microfluidic separation techniques. 38
Deterministic lateral displacement
A DLD microfluidic device consists of micron-sized tilted pillar arrays that generate a fluid bifurcation and a unique number of streamlines between the gaps corresponding to the periodicity of the DLD array. Particle flows in the DLD array are influenced by fluidic forces and pillar obstacles’ effects. Depending on the pillar size and spacing, cells with diameters less than the critical diameter move directly through the gaps between the micropillars, while cells bigger than the critical diameter bump into the micropillars and displace laterally to the next streamline. 39
A number of DLD devices have been investigated to isolate CTCs and CTC clusters from blood samples. 40 For example, Loutherback et al. developed a DLD microfluidic device consisting of arrays of triangular-shaped micro-posts to increase throughput and reduce clogging. Using this device, they achieved >85% CTC capturing efficiency at an extremely high flow rate of 10 mL/min without compromising the cell viability. 41 Au et al. developed a two-stage DLD microfluidic device to continuously isolate CTCs and clusters based on their size and irregularity. In the first stage, large clusters (>30 μm) were captured within a standard DLD channel with round micropillars (50 μm diameter, 63 μm gaps). The remaining blood components, including smaller CTC clusters and cells, were then transported into the second stage inlet, where irregular ‘I’-shaped pillars were designed with a restricted height for more efficient CTC capture. The overall recovery of CTCs using this device was ~99% and due to low shear stress throughout the channels, >87% of cells remained intact and viable. 42 Recently, a new concept called filter DLD was introduced and developed by Liu et al. Using this cascaded microfluidic device, they could isolate CTCs at relatively higher throughputs than the conventional DLD devices with no clogging issues. This device captured CTCs at >96% efficiency, 99.99% cell purity (removal of WBC), and >98% viability. 43
In addition, recent developments make it possible to use DLD pillar arrays to detect biomolecules, including proteins and vesicles.44–47 In addition, recent developments in DLD demonstrate its capacity to classify particles according to their shapes, flexibility, and electrical features. Although DLD has demonstrated versatility as a particle separation technique with high resolution for various applications, it is limited by several drawbacks. These include low throughput, pillar clogging, and a challenging experimental setup. 48
Inertial microfluidics
Inertial microfluidics is a technique by which cells of different sizes and shapes are differentially ordered in microchannels without needing external forces. By flowing the sample into microchannels, cells are exposed to a superposition of lift and shear forces acting on particles in opposite directions. 49 Over the last few years, multiple applications of inertial microfluidics have been implemented for capturing CTCs from the biofluids like blood. In 2018, Zhou et al. designed a simple straight microfluidic channel with a rectangular cross-section to separate CTCs directly from whole blood and RBC-lysed samples. In this study, they could separate spiked HepG2 cells from blood with 89% efficiency. This device is a multi-flow channel where the saline solution was used as a buffer to collect targeted cells migrating from side streams to the middle cell-free stream. The cutoff size was set to 15 μm to reduce WBC contamination and leftovers. However, small CTCs could not be separated using this proposed multi-flow microfluidic channel.12,50
To increase the throughput, multiplexing of several devices into one has been explored in many studies. For example, Khoo et al. enriched CTCs from blood samples of patients with both advanced-stage metastatic breast and lung cancers. They reported that their novel multiplexed spiral device could quickly detect the CTCs with high sensitivity (100%) from 7.5 mL of clinically relevant blood sample in less than 5 min. 51
Curvilinear channels have also been investigated for CTC isolation, where the spiral geometry of channels causes a lateral Dean to drag force in addition to the shear and wall induced lift forces. The resulting Dean flow is a consequence of centrifugal acceleration of fluid flow in curved channels. In 2013, Hou et al. developed a spiral microfluidic channel to separate CTCs from patient blood. Their spiral microchannel recovery efficiency was >85%, and the device proved 100% sensitive in clinical validation with metastatic lung and breast cancer patients. 52 In a subsequent study by the group, they reduced the processing time using multiplexed spiral microchannels, enabling CTC isolation at a flow rate of 36 mL/h 53 . The study also used an RBC-lysis pre-step that ensured minimal contamination, reducing cell concentration and cell–cell interactions. 54 In another study published by Bhagat et al. and colleagues, a method for processing diluted blood was introduced and developed based on inertial microfluidics. This method dynamically pinched flow with a high aspect ratio microchannel to focus rare CTCs and functioned with high throughput. The capturing efficiency of the device was investigated with spiked MCF-7 blood samples with 20 times dilutions. Results revealed more than 80% recovery efficiency with 3.25 × 105 fold RBC and 1.2 × 104 fold leukocyte enrichment. 55
Lin et al. developed a labyrinth microfluidic device with a combination of sharp edges and long microchannels to capture and isolate CTCs with high purity and throughput. The recovery efficiency of this device was > 90% at a 150 mL/h flow rate, and leukocyte leftovers were calculated at approximately 600 cells/mL. 56
Gao et al. developed a novel multi-stage microfluidic device to isolate cancer cells from an unprocessed blood sample. Regarding their report, U87 cells (human brain malignant glioma cells) were isolated with more than 90% efficiency and a 95% viability rate. However, the device’s throughput was 0.54 mL/h, making it unsuitable for applications requiring higher operational throughput. 57 Other approaches were introduced to increase CTC capturing efficiency and throughput by combining microfluidics with affinity-based capturing techniques. CTC-iChip is one of the most well-known techniques where the magnetic-affinity-based capturing technique is combined with both DLD and inertial microfluidics. 58 This system can isolate all types of CTCs at high throughputs (8 mL/h) and with broader applicability to non-epithelial cancers. In 2021, Nasiri et al. proposed a hybrid technique using inertial microfluidics and magnetophoresis to capture CTCs. To this end, the CTCs-anti-EpCAM conjugates and magnetic nanoparticles were spiked in diluted blood and processed at 60 mL/h flow rate. The result showing capture efficiency and purity of the system was ~95% and 93%, respectively. 59 While these combined strategies ensure high capturing efficiency, they require further optimization to ensure high purity and minimize antibody consumption, making it more affordable than other label-free isolation techniques.
Overall, inertial microfluidics has proven advantageous over other techniques due to its minimum cell deterioration effects, high throughput, simplicity, and ease of use. The two examples of successfully commercialized inertial microfluidic platforms are Vortex Bioscience and ClearCell FX.50,52
One of the major shortcomings of inertial microfluidic devices for studying CTCs and clusters is their inability to replicate entirely in vivo. For example, in vitro-generated models might show variations in gene expression and phenotype in contrast to primary tumors that are characterized by heterogeneity. 60 Another constraint in these models is the need for specialized training in operation and fabrication. This is due to the absence of established standards in the development of microfluidic devices. Simplified and user-friendly operation is essential for translating these systems into the clinical setting. 61
Dielectrophoresis
Dielectric forces result from interactions between a non-uniform electric field and the induced electrical polarization of cells. The method exploits the polarizability of cells and particles within an electric field gradient to facilitate cell separation. The induced polarization and unique cell and membrane properties create high-field regions that either hold the cells in place (positive dielectrophoresis) or push cells away from the region (negative dielectrophoresis). The particle’s motion is influenced by its polarization properties and the surrounding medium, thus allowing for label-free cell separation. 62 Dielectrophoresis has been implemented for sorting multiple types of cells, including CTCs, and has demonstrated superiority over other electrophoretic cell separation methods. 40
Two commercially available dielectrophoretic platforms are DEPArray and ApoStream; the first functions by trapping single CTCs, while the latter allows for continuous isolation of CTCs. 63 DEParray is mainly used for downstream analysis of single CTCs after being isolated either via a microfluidic platform or a commercial machine like the CellSearch system. ApoStream uses interdigitated electrodes at the bottom of a microfluidic channel. In this technique, CTCs are influenced by positive dielectrophoretic forces and collected from the target outlet. At a 1 mL/h flow rate, >70% recovery efficiency has been reported for mesenchymal and epithelial cell lines, equal to approximately 10,000 white blood cells per mL of sample. 64 One of the primary limitations of ApoStream™, as well as other DEP-based sorting systems, is the limited cell throughput, which is below 200 million cells/hour. Moreover, the technology requires an advanced multi-injection system as another technical improvement. 65 Some other dielectrophoresis strategies include optically induced dielectrophoresis and dielectrophoretic field flow fractionation. However, these methods mainly suffer from low throughput despite high recovery rates. 66 Overall, dielectrophoretic methods are more feasible and affordable than flow cytometry cell sorters and magnetic-based separation since they do not require cell labeling. 67
Acoustophoresis
Acoustophoresis is another CTC-capturing technique that exploits the physical properties of the cells. This label-free technique uses acoustic waves to expose cells to acoustic force and displace them in a specific direction. 68 Ultrasonic acoustic resonance induced by piezoelectric material within a microchannel produces force to manipulate cell particles. The density and compressibility of cells influence the magnitude of the acoustic forces, the fluid medium, and the amplitude of acoustic waves. Thanks to these acoustic forces particles can be controlled rapidly and spatially without affecting their viability. These acoustic forces allow rapid and precise spatial control of particles in microchannels without impacting cell viability. 69
In 2015, Li et al. proposed an acoustic-based microfluidic technique to isolate CTCs from patient blood at 20 times higher throughput than tilted-angle standing surface acoustic waves (taSSAWs) with high capturing efficiency. This technique could achieve 83–96% recovery efficiency for different types of spiked cancer cells. 70 Due to the overlapping acoustic properties of some WBCs with CTCs, the purity of the acoustic-based technique is compromised, and additional post-processing is usually required. Cushing et al. developed an immune-acoustophoresis technique to cope with this challenge using acoustic pressure antinodes. 71 In this study, WBCs were bound by elastomeric particles (EPs) that are activated with CD45 antibodies. The EP/WBC complexes were then aligned at the antinodes of acoustic pressure while CTCs were concentrated in the microchannel’s center. This technique reduced WBC contamination and eliminated particle aggregation with negative acoustic contrast by utilizing a unique acoustic actuation workflow. The separation efficiency of breast and prostate CTCs were 98.6% and 99.7% with a high viability rate of 89.8% and 85%, respectively. Scientists at Duke University have successfully isolated and characterized CTCs and CTC clusters from clinical patient samples with metastatic prostate cancer using their unique acoustic-based CTC separation platform. They identified CTCs from five clinical blood samples using immunostaining criteria, ranging from 0.93 to 400 CTCs per mL. 72
Despite the high performance of acoustic-based techniques, there still is a lack of stability during long-term procedures and sufficient throughput to analyze larger sample volumes. 40 Moreover, this method also suffers from higher costs associated with the complex equipment required for cell sorting.73,74
CTC clusters isolation
While most technologies have prioritized the analysis of individual CTCs, isolation of disease-relevant CTC clusters has also garnered significant research interest in the recent past. 42 Studies have shown that the metastatic competence of multicellular clusters of CTCs could be 100-fold higher than that of individual CTCs. 75 CTC clusters are aggregates of more than two CTCs, usually containing not only tumor cells but also endothelial cells, stromal cells, cancer-associated fibroblasts, leukocytes, erythrocytes, and platelets found in the blood of solid tumor patients. 76 In mouse models, CTC clusters appear to seed half or more secondary metastatic tumors, and patients with small-cell lung cancer, breast cancer, and prostate cancer have considerably lower progression-free survival (PFS) rates even when one CTC cluster is detected in their blood samples. 42
Over the past few years, several research groups have developed technologies to enhance the capturing efficiency of these CTC clusters. Zeinali et al. and colleagues designed a biomarker-independent microfluidic ‘Labyrinth’ device that recovered 100% of heterogeneous CTCs and 96% of CTC clusters in patients with metastatic NSCLC. 77 While the system achieved high efficiency and recovery rate, it still needed RBCs to be removed using dextran solution density separation prior to running the sample, thus increasing the processing time. Kamyabi et al.’s team developed a microfluidic model with 10,000 trap chambers to isolate CTC clusters according to size and dynamic force balancing against a pillar obstacle in the trapped chamber. 78 This device works with unprocessed blood samples so that after injecting the whole blood, the clusters were back flushed for downstream analysis. In another study, researchers presented a continuous microfluidic chip using DLD based on size and inherent asymmetry to isolate and recover viable CTC clusters from blood. 42 With minimal cluster dissociation, this integrated two-stage device recovered CTC clusters of 2–100+ cells from whole blood with 99% recovery of large clusters, 87% cell viability, and five times the red blood cell depletion. The platform offered a continuous, label-free, and low-shear stress design that can be integrated with downstream analyzing technologies as well as sorting CTC clusters into different outlets based on size.
By exploiting the unique geometry of cellular aggregates, Sarioglu et al. could capture CTC clusters in 30–40% of unprocessed blood samples of metastatic breast, prostate cancer, and melanoma patients using a novel Cluster-chip. 79 A subsequent study by this group introduced Cluster-Wells with >100,000 microwells to physically arrest CTC clusters ranging from 2 to 100+ cells in the unprocessed whole blood samples of ovarian and prostate cancer patients. Due to its many microwells, this device could analyze large volumes of samples in minutes. Using microwells rather than a traditional membrane filter protected clusters from external stresses during or after processing, allowing them to be used in further analysis. 80
Edd et al. developed a microfluidic PDMS device combining inertial focusing with repetitive flow-shifting in a non-equilibrium inertial separation array to continuously isolate CTC clusters and preserve their configurations. They reported that minimum cluster breakup on chip happens compared to filtering methods. With 4 mL/min processing time, it is a very fast device that can be used to generate CTC lines and downstream in vitro drug testing. 81 There is evidence that CTC clusters are associated with decreased overall patient survival and PFS. 82 Therefore, the isolation and in-depth study of CTC clusters are necessary for holistic metastasis comprehension and better management of cancer.
Clinically available methods
Although the CellSearch system is still the only FDA-approved method for isolating CTC, clinical application of other technologies is also reported in many studies. 83 Using Vortex technology, Dhar et al. enriched CTCs from NSCLC patient samples with a very high efficiency rate to help determine response to immunotherapies. 84 Another isolation technique, DEPArray, integrates microelectronics and microfluidics in a highly automated platform to isolate pure, single, and viable CTCs for further molecular analysis. 63 The utilization of DEPArray technology in analyzing copy number alteration (CNA) burden has revealed that CTCs have different aberration levels depending on the time point and subtype. 85
In 2014, Warkiani et al. introduced a cost-effective, fast, and user-friendly microfluidic device. This device can isolate CTCs from large patient blood volumes using a label-free, size-based approach while achieving ultra-high-throughput. The rapid processing time of this technology, which is capable of processing 7.5 mL of blood in under 10 min, coupled with its capacity for recovering a greater number of CTCs from larger blood samples, presents a diverse array of possibilities for genomic and transcriptomic research. One notable benefit of this device is its capacity to recover all blood fractions, including plasma (through centrifugation), CTCs, and white blood cells (sorted based on size), which can be utilized for various biomarker studies or molecular assays like real-time polymerase chain reaction (RT-PCR). The biochip’s clinical efficacy was demonstrated through the detection of CTCs in blood samples collected from patients with advanced-stage metastatic breast and lung cancers. 86 In addition to the example methods in the clinic, EPISPOT assay, Parsortix, NanoVelcro technology, ApoStream, and others are applied for CTC enrichment and isolation in clinics.87–89
Despite many discoveries in liquid biopsy, widely implementing these techniques in clinics requires many challenges to be addressed. Improving the sensitivity and specificity of CTC and ctDNA detection techniques is essential for accurately identifying and quantifying these biomarkers in the bloodstream, particularly during the early stages of the disease. 90 Standardizing methods for the isolation, detection, and analysis of CTCs and ctDNA are essential to preserve comparable accuracy of results across different medical settings and laboratories. Standardized protocols and quality control can minimize inter-laboratory variability and boost the quality of liquid biopsy findings. 91
Validation of the clinical utility of CTC and ctDNA analysis is necessary through comprehensive, prospective clinical trials. These trials should aim to evaluate the diagnostic precision, prognostic significance, and medical consequences linked with liquid biopsy examinations across various cancers and their different stages. 92 Another issue with using liquid biopsy testing is the cost of analysis. To expand the accessibility of CTC and ctDNA analysis, it is essential to cut the cost of these tests. There is a pressing need to advance the development of liquid biopsy technologies and methods that are both cost-effective and scalable to promote their widespread implementation. 93
Novel approaches in CTC characterization
While antigen-independent approaches have been prioritized toward developing enrichment and isolation of CTCs, conventional systems like immunocytochemistry, genomic aberration studies, and RT-qPCR have been relied upon for the molecular profiling of CTCs.94–96 Moreover, molecular-based single CTC analysis has provided new insights into key cancer mechanisms, including tumor cell dissemination from the primary site, migration to the target organs, and metastasis. 97 Molecular approaches allow for assessing the changes in protein expression or alterations in the CTCs and CTC cluster surface markers whose biophysical strategies cannot investigate. Thanks to recent advances in single-cell technology, in-depth genome, transcriptome, and proteome characterization are now possible using next-generation sequencing (NGS), single-cell sequencing, and proteomics studies (Table 2).25,94,98,99
Molecular profiling of circulating tumor cells.
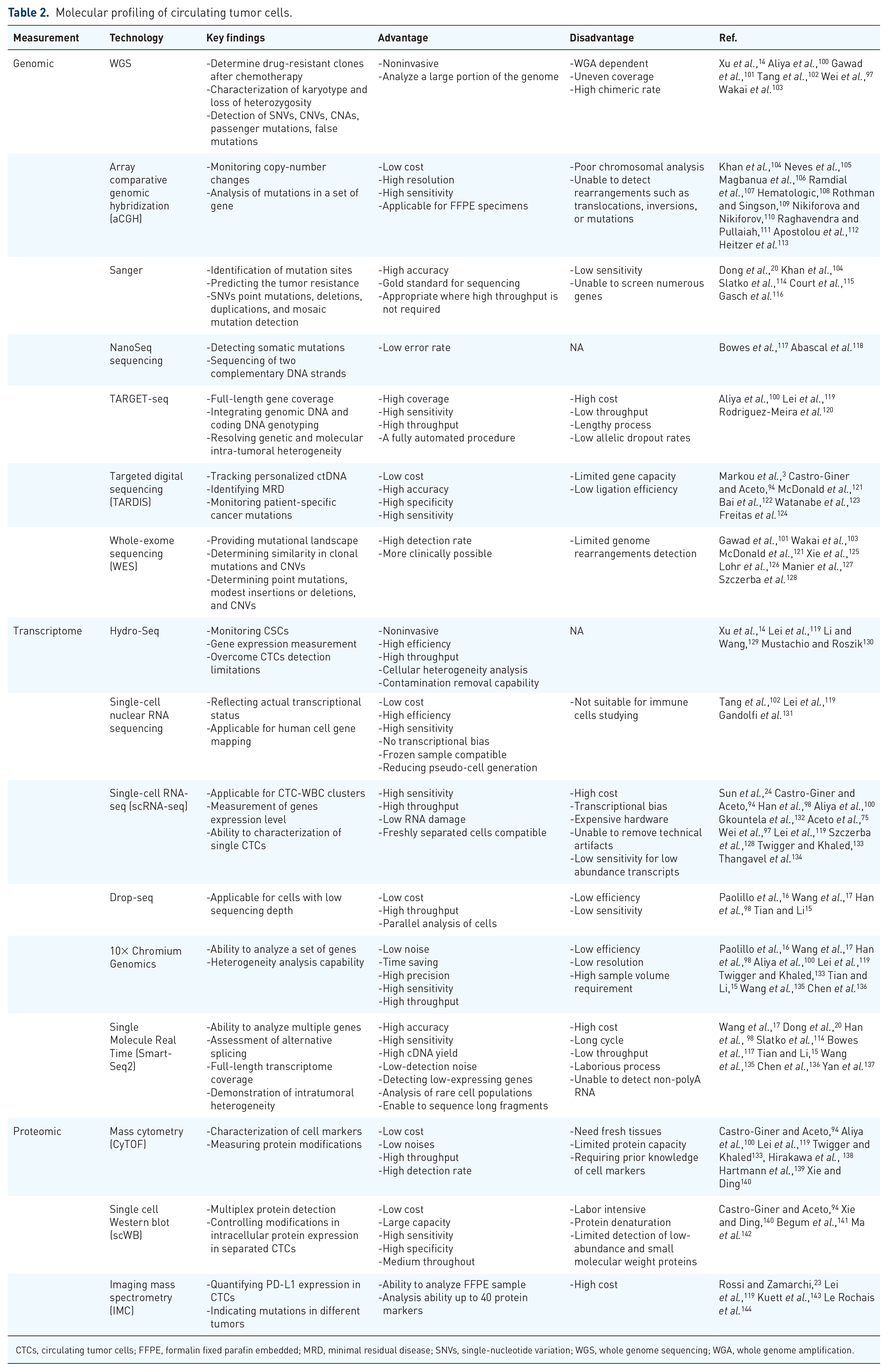
CTCs, circulating tumor cells; FFPE, formalin fixed parafin embedded; MRD, minimal residual disease; SNVs, single-nucleotide variation; WGS, whole genome sequencing; WGA, whole genome amplification.
Immunophenotypic characterization of CTCs and CTC clusters
Multiple studies have been conducted to assess the metastatic potential of CTCs using membranous detection of epithelial and mesenchymal markers since these cells have been known to promote metastatic progression.145,146 However, additional markers that may not be exhibited in all CTCs can provide a comprehensive view of cancer heterogeneity.
While certain surface epithelial markers, such as EpCAM, are expressed in most cancer cells, detecting them on CTCs is challenging due to their low and inconsistent expression profiles. Moreover, the downregulation of epithelial markers like EpCAM might result from EMT. 147 In this phase, applying EpCAM-based selection methods does not allow for an accurate estimation of the number of CTCs. Therefore, simultaneously detecting epithelial and mesenchymal markers and adopting marker-free detection methods can improve CTC characterization efficiency.148,149 For example, a dual antibody assay targeting N-cadherin and EpCAM can detect CTCs in breast cancer patients. 150 Belthier et al. employed magnetic bead-linked anti-CD44 antibodies to identify EpCAM-negative CTCs in colorectal cancer (CRC) patient samples and observed that CD44 was highly expressed on CTCs. 151 In a similar study, researchers used Graphene Oxide CTC chips to characterize breast cancer cells using anti-HER-2 and anti-Vim/N-cad antibodies. 152 These studies also compared the human epithelial growth factor receptor 2 (HER2) expression level in the primary tumor and CTCs. To characterize various cellular subtypes having EMT features, other methods, including Vimentin and N-cadherin immunofluorescence (IF) analyses, have been attempted. 152 Due to considerable biological variability, different cancer types express different markers on CTCs. Furthermore, within a single tumor, spatially distinct microenvironments generate incongruent CTCs that describe the population with minimum detectable indicators. 153 Thus, there is high demand for better characterization of CTCs, by improving the sensitivity and efficiency of immunophenotyping or by integrating with other molecular analysis methods.
CTC clusters are multicellular CTC aggregates and can be differentiated into homotypic (composed of similar CTCs) or heterotypic (CTCs and various cell types like immune cells, fibroblasts, platelet, etc.) clusters (Figure 2). 154 CTC clusters are more metastatic than single CTCs because they express specific adhesion and stemness markers such as plakoglobin and CD44, responsible for a higher metastatic potential. 155 Furthermore, the participation of other cell types, particularly immune cells, confers the CTC clusters with unique properties due to the diverse immune cells having specific surface markers and characteristics. 156 Compared to single CTCs or homotypic CTC clusters, WBC-CTC clusters are more durable and aggressive (Figure 2). 157

(a) Circulating tumor cells (CTCs) and CTC clusters found in NSCLC patients. CTCs were detected by drawing 7.5 mL of peripheral blood. CTCs were enriched by microfilter isolation, and immunofluorescence staining was performed for cytokeratins (CK) 8/18 and/or 19, EpCAM, CD45, and the nucleus identified with DAPI (a–d). CTC clusters were defined as an aggregated group of ⩾2 CTCs. CTC clusters were observed in different shapes: spherical (e,f), triangular (g,h). Reproduced with permission from Manjunath et al. 154 under open Creative Commons Attribution License.
Interaction of CTCs and CTC clusters with immune cells
Following dissemination from the origin site and entering the bloodstream, CTCs go through the vascular walls of a target organ to generate new tumor tissues. 158 Although there is no agreement upon where CTC clusters are generated, CTCs can interact with numerous immune cells such as macrophages, neutrophils, natural killer (NK) cells, and lymphocytes, and form WBC-CTC clusters. This interaction can occur between cells directly through their surface markers to make a heterotypic cluster/hybrid or indirectly via molecules that impact the cell phenotype and function. Cell–cell adhesion is crucial for CTC survival, shielding them from the harsh environment inside the bloodstream and enabling their extravasation. 159 Studying surface or soluble markers on immune cells or CTCs contributing to these interactions can be a valuable tool for characterizing CTCs, CTC clusters, and hybrid cells.
Neutrophils are the first line of cellular defense and the most abundant WBC in the blood. They suppress tumor growth and metastasis and kill the tumor cells via their anti-tumorigenic activities. In addition to tumor-killing neutrophils (N1), protumor phenotype (N2) facilitates tumor expansion. 160 Imbalanced neutrophil to lymphocyte ratio is an independent factor associated with lower overall survival (OS) in various solid and hematological malignancies. 161 Vascular cell adhesion molecule 1 (VCAM-1), which mediates the interaction of neutrophils with CTCs, has been shown to promote CTC proliferation and metastatic potential. 128
It has been discovered that the binding between CD11b+ neutrophils and triple-negative breast cancer (TNBC) cells is facilitated by the intercellular adhesion molecule (ICAM-1). In vivo experiments have shown that inhibiting CD11b deficiency can effectively prevent TNBC metastasis in vivo. 162 CTC–neutrophil association leads to gene expression modification and over-expression of some proteins on the cells and can be good candidates for CTC and CTC cluster characterization. 163 As neutrophils have a high extravasation potential, their contribution to cluster formation may regulate immune surveillance activities and facilitate WBC-CTC cluster attachment to the target organ’s vascular and homing.
Tumor-associated macrophages originate from the main tumor site and cause CTC seeding in the secondary organ. The association between macrophages and cancer cells comes with several names in the literature depending on the cancer type, the formation mechanism, and various expressing markers. Adams et al. isolated circulating cancer-associated macrophage-like cells (CAMLs) from breast, pancreatic, or prostate cancer samples. These clusters were expressing epithelial, endothelial, and monocytic markers simultaneously. 164 CAMLs were comprised of gigantic myeloid cells (CD14+/CD11c+) with enlarged nuclei that were positive for CD45 but also expressed epithelial markers, including CK8/18 and 19 and EpCAM. According to their findings, CAMLs in the circulation could interact with CTCs by attaching to or engulfing them. CD47 on the CTCs interacts with the signal regulatory protein alpha (SIRPα) on macrophage surfaces, resulting in downstream inhibitory regulation that reduces phagocytic capability. 165
Another study found that after phagocytosis of apoptotic cancer cells, macrophages could express epithelial markers (keratins and EpCAM) as well as stem cell markers (Oct4). These tumor–macrophage fusion cells were undetectable in the blood of healthy donors, indicating their clinical utility as a cancer diagnostic.166,167 Various types of macrophages and CTCs fusions reveal that they are M2 meaning that they could contribute to reshaping the target tissue to generate new tumors and suppressing the immune system. 168
As innate immune cells, NK cells have high cytolytic activity against tumor cells and virus-infected cells. NK cells have a diverse tissue distribution and phenotypic heterogeneity. NK cells produce multiple activating and inhibitory receptors that recognize abnormal protein expression on target cells and regulate cytolytic action. 169
While recent studies showed NK cells can kill CTCs, CTC clusters have indicated increased resistance to NK cytotoxicity function. 170 However, during the metastatic cascade, activation of EMT in tumor cells results in altered cell-surface ligands that can be detected by NK cell-activating receptors, increasing sensitivity to NK cells. 171 Chockley et al. have reported that the balance of activating and inhibitory receptors activated by various ligands is crucial for NK cells to eliminate metastatic tumor cells. For instance, NK cells express killer lectin-like receptor G1 (KLRG1), which transmits an inhibitory signal via E-cad as a ligand. During EMT, the downregulated E-cad loosens its inhibitory effect on KLRG1, leading to NK cell activation. Furthermore, EMT enhances the expression of cell adhesion molecule 1 (CADM1), an NK activator that binds to the cytotoxic and regulatory T-cell-associated molecule receptor on NK cells. 172
Overall, increasing the number of NK cells is extremely favorable to cancer patients’ survival. However, in CTC-positive metastatic patients with a variety of tumor types, the cytotoxic and cytolytic capabilities of NK cells are frequently compromised. 173 In addition, there is often a negative correlation between the quantity of CTCs and the total count of NK cells in the blood of cancer patients. 174
Lymphocytes are composed of T cells, B cells, and NK cells. These cells control the immune response, produce antibodies, and kill tumor and virus-infected cells. 175 Tumor cells consistently try to hide from being detected by the immune system. 176 The cancer-immune evasion mechanism mostly relies on the programmed cell death-1 (PD-1) receptor, a negative immune regulatory checkpoint expressed on activated T cells.177,178 When the PD-1 ligand (PD-L1) binds to PD-1, a robust inhibitory signal is transmitted into the T lymphocyte, which affects cytokine production and T-cell proliferation. 178 The expression of PD-L1 on CTCs and CTC clusters as an immune evasion strategy has been reported in several studies.179,180 Likewise, an inverse relationship between CD3+, CD4+, and CD8+ peripheral T-lymphocytes and CTCs in NSCLC and between CD8+ peripheral lymphocytes and breast cancer has been investigated recently. 181 Few studies generally focus on direct interactions between CTCs, CTC clusters, and lymphocytes. However, T CD4+ and CD8+ cells can interact directly with CTCs via the FAS-FASL, PD1-PDL1, and CTLA 4, activating immunosuppressive responses, resulting in increased tumor cell survival. 182
Genomic characterization
Tumor resistance and evolution are heavily reliant on genetic instability. 104 Genomic analysis of CTCs gives valuable information on the metastatic process and the emergence of tumor subclones, as well as monitoring therapy response and promoting personalized therapeutic approaches. 183 Despite the availability of numerous effective CTC enrichment and isolation techniques, their scarcity in blood samples has limited comprehensive molecular investigation. This issue can be addressed by analyzing CTCs from the same patient using larger volumes of blood. However, the samples may contain residual lymphocytes, decreasing molecular resolution. 153 Until recently, fluorescence in situ hybridization (FISH), digital PCR, BEAMing PCR, and RT-qPCR were the standard procedures for molecular analysis of specific genes in CTCs.99,184,185 More sensitive methods, such as whole genome sequencing (WGS) and whole exome sequencing (WES), are currently being explored as more precise tools for the genomic characterization of individual cells (Figure 3 and Table 2).
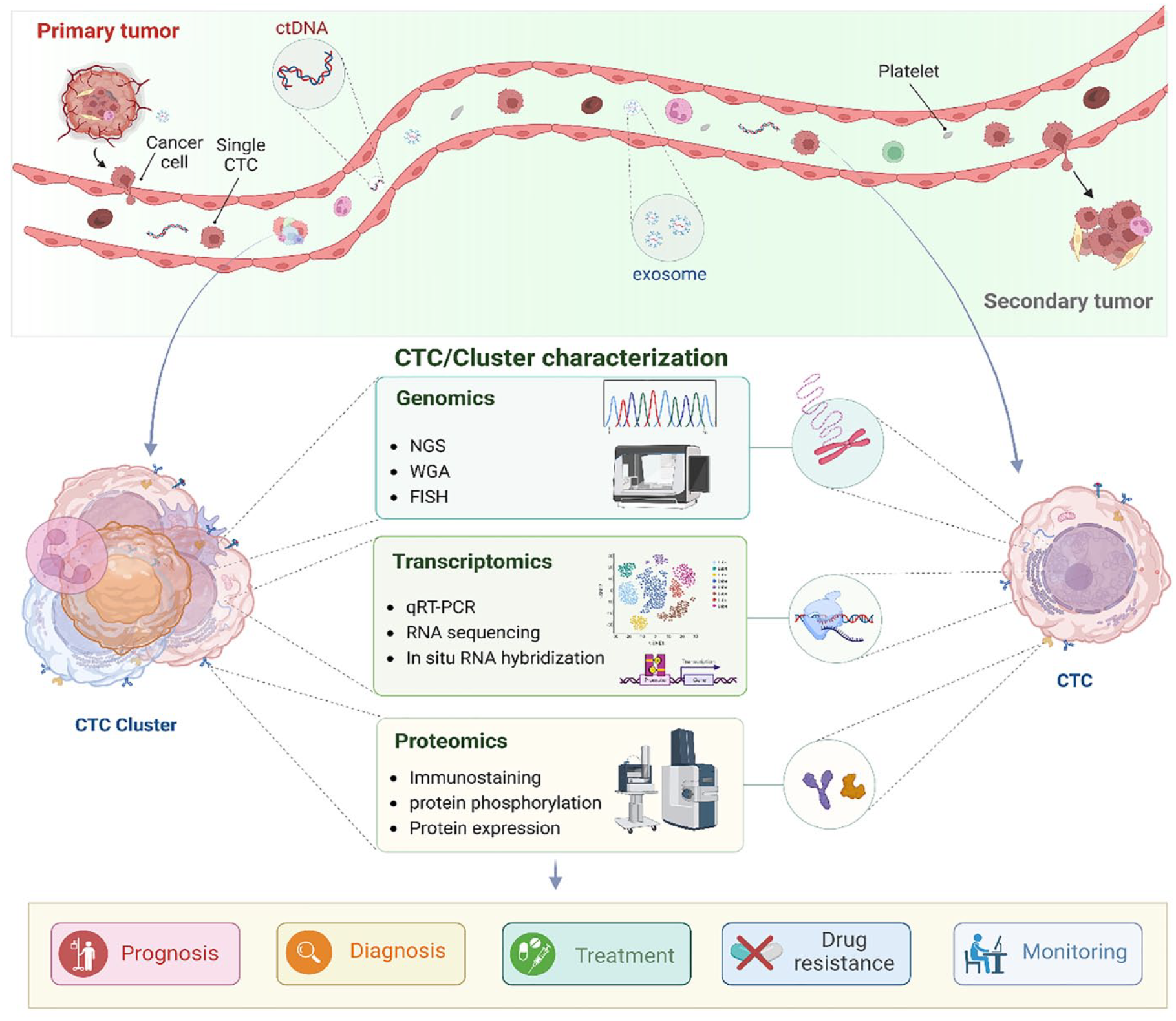
Molecular characterization of circulating tumor cells (CTCs) and CTC clusters. CTC and CTC clusters genome analysis can be evaluated by identifying different genomic abnormalities with techniques such as FISH, WGA, and NGS. By dissociating clusters into single CTCs, the same analysis can be done on them. CTC/Cluster gene expression and CTC-specific isoforms can be demonstrated by qRT-PCR, RNA-sequencing, and in situ RNA hybridization. Immunostaining assays, on-chip western blotting, microfluidic qPCR, and imaging mass cytometry can be used to investigate the proteome of CTCs.
Single-cell sequencing
Single-cell sequencing has influenced research in various fields, including cancer research. Recent cancer genomic, transcriptomic, and proteomic studies have considerably improved our understanding of tumorigenesis, metastasis, and recurrence.15,186 Although bulk analysis is still common, precise diagnosis and personalized therapy must evolve around tumor heterogeneity. Numerous studies suggest that only specific subpopulations of cancer cells cause the disease showing how effective single-cell analysis could be.14,97 As cell-sequencing technology improves, more precise and defined biomarkers can be employed for improved cancer staging and prognosis.117,187
Every cell has only 6–7 pg of DNA, which is significantly less than the WGS requirement. Whole genome amplification (WGA) allows for single-cell molecular profiling to analyze the differences in gene activation at various disease stages, thereby guiding therapy decision-making.146,184 WGA is performed using three main techniques: First, PCR amplification, which includes long and accurate PCR (LA-PCR), primer extension preamplification PCR (PEP-PCR), degenerate oligonucleotide primer PCR (DOP-PCR), tagged random primer PCR (T-PCR), ligation-mediated PCR (LM-PCR), and interspersed repetitive sequence PCR (IRS-PCR). 188 Second, linear amplification via transposon insertion (LIANTI) and multiple displacement amplification (MDA). Third, the multiple annealing hybrid method that involves looping-based amplification cycles (MALBAC) generates extremely uniform amplification over the whole genome. In common practice, MDA, DOP-PCR, and LIANTI are the most common methods for WGA. 100
DOP-PCR is the most effective approach for amplifying low-copy genomic DNA. 189 DOP-PCR can be used for genotyping polymorphism insertion and deletions, single nucleotide polymorphism, and single-stranded conformation polymorphism. 190 The most common WGA method for high amplification throughput is multiple MDA. LIANTI detects micro-copy number variation at the kilobase level with high resolution. Using this method, Chen et al. directly observed cell-to-cell differences in the origins of DNA replication. 191
WGA addresses primer annealing kinetics, enzyme consistency, and insufficient amplification throughput. However, there are still some issues with adequate coverage, amplification variations, and allele deletion, which might result in single-nucleotide variation (SNV) and false-positive results. 192 Following DNA amplification, single CTCs genotyping can be performed by Sanger sequencing, NGS, SNV, and comparative genome hybridization (CGH).126,193–195 Mutation or copy number variation of some cancer-related genes (ALK, RB1, SMAD4, MYCN) reported using single-cell sequencing on CTCs in neuroblastoma (NB) patients. 196
Sanger sequencing
The Sanger dideoxynucleotide sequencing method was first developed over 40 years ago as an enzymatic technology for DNA sequencing. 197 The Sanger reaction has two major phases: assembling template-directed ladders and electrophoretic separation, followed by a sequence detection step. It is the gold standard of sequencing technology and is a common approach for detecting point mutations, deletions, SNVs, mosaic mutations, and duplications and is primarily suitable for a single cell or a small number of cells. 198
A study by Xue et al. shows a high consistency between the tissue-NGS and CTCs-Sanger sequencing. They reported that more than 85% of the mutations detected by NGS could be detected by Sanger sequencing. 199 Nevertheless, the sensitivity of Sanger sequencing is limited to detecting low levels of mutation. Several research studies have concluded that a minimum of 10–25% of mutated DNA within a sample is required for accurate detection, therefore limiting its applicability in clinical environments. 200
Next-generation sequencing
This approach was developed by merging biochemistry, optics, and engineering, offering valuable genetic information in less time and at a lower cost than the traditional Sanger method. Initially, NGS was used for bulk DNA and RNA sequencing. 101 Although bulk NGS can scan millions of cells at once, it cannot provide helpful information on cellular heterogeneity, CTCs, or ctDNA. 201 As a substitute, single-cell NGS (scNGS) has recently attempted to sequence single cells by generating genomic, transcriptomic, and proteomic data. However, although scNGS can resolve bulk NGS noise, single-cell sequencing is still considerably more expensive than typical bulk NGS due to technical complexities such as sampling and insufficient sensitivity. 202
De Luca et al. discovered 51 sequence variations in 25 CTCs using NGS. They also discovered a high amount of intra- and inter-patient variability and heterogeneity in the mutational condition of CTCs and primary tissue. 203 Another recent study used NGS to demonstrate that various metastatic sites in the CTCs genome have matching mutation genes. 204 He et al. and colleagues employed NGS for 6 CTCs and identified 44 mutant cancer-related genes in CTCs, including KIT, SMARCB1, and TP53 genes. 205
Using NGS-based methods has been associated with some limitations, though. NGS is susceptible to sequencing errors due to its strand synthesis nature and PCR amplification. 206
As the NGS read lengths are often shorter (35–700 bp) than classic Sanger sequencing platforms, a detailed evaluation of the results is necessary, especially for variant detection and clinical purposes. Although length limitations have been resolved by long-read sequencing, NGS is still significantly more expensive and has low throughput. In addition, sample preparation and preparation and sequencing chemistry can all cause sequencing bias and noise, affecting the accuracy and reproducibility of the NGS results. 207
Furthermore, obtained dataset requires to be comprehensively analyzed to extract clinically important information. 208 Additional players will strive to further improve the field with unique sequencing solutions in the coming years. These existing and upcoming NGS methods can potentially enable transformative science, such as direct RNA or protein sequencing and personalized medicine based upon individual genome sequencing.
Comparative genome hybridization
CGH was used for the first time in the early 1990s for analyzing whole genome chromosomal gain and loss. It has since improved in modern iterations, with the most recent version of this technology being array microarray CGH (aCGH), which enables the analysis of single-cell WGA output for CNAs in a manageable and standardized analysis workflow (Table 2).195,209,210
Following aCGH, CNA data analysis includes measurement of the fluorescent intensity ratios of the signals produced by the hybridization of patient samples compared to reference genomic DNA to an array of DNA probes. Millions of DNA probes are distributed across the genome on the aCGH array. Using a specific software, the data are normalized and the genome is segmented into regions with comparable CNAs to identify accurate copy number changes. Following that, the data are subjected to evaluation to figure out particular genomic regions that show alterations in copy number, as well as determine the scale and position of these modifications.104,188
Polzer et al. and his team assessed the CNA in breast cancer patients using aCGH. Although all patients had the same kind of tumor, they had heterogeneous CNAs, implying that breast cancer can have a novel typology based on CNA patterns. 211 ACGH analysis of CNA in CTCs of CRC indicates a similarity with the primary and metastases tumor.113,212 Using aCGH, CTCs and accompanying leukocytes from metastatic castration-resistant prostate cancer (mCRPC) patients showed PTEN loss, genetic changes in the chromatin network, and proliferative pathways. 213 Another study on signaling pathways by Magbanua et al.’s group discovered gains and losses in 8q and 8p, respectively, as well as gains in the AR region of chr X of CTCs. 214 Ferrarini et al. found a large copy number of the c-MYC gene and loss of copy number in the BRCA2 locus in lung cancer CTCs. The utility of CGH is disadvantaged by poor resolution (5–10 Mb), labor intensity, and lengthy protocol.215,216
Single nucleotide variation
SNVs can be inherited by daughter cells during DNA replication, making it a useful approach for describing tumor cell heterogeneity and evolutionary development (phylogenetic) connection.217,218 Detecting SNVs using WGS or WES can provide the clonal architecture of tumors. 219 Assessing how heterogeneous and aggressive the different clones are in the tumor microenvironment not only allows easier monitoring but also helps guide treatment decisions.
However, large-scale adoption of SNVs has been limited because tumor cell genome distribution is sparse, making SNVs detection difficult. 220 Rossi et al. discovered that more than half of CTCs in breast cancer patients had two clinically significant mutations. PIK3CA and MLH1 genes were altered in 13 of 23 CTCs. In their analysis, they discovered a nonsynonymous SNV in AKT1 as well as alterations impacting the TP53 sequence. 221 According to recent studies, the most affected genes in hepatocarcinoma cancer (HCC) patients contributing to signaling pathways are PI3K/AKT/mTOR (PTEN, PIK3CA, KRAS), chromatin remodeling pathway (ARID2, ARID1A, NCOR1), and Wnt/b-catenin pathway (CTNNB1, AXIN1, APC).203,222,223
DNA methylation in CTCs
DNA methylation is an epigenetic process that enables cells to regulate their genes. 224 The study of how DNA methylation occurs and its influence on gene expression in cancer has received much attention in recent years, indicating that some changes in DNA methylation are more common in certain types of cancer. 225 DNA methyltransferases (DNMTs) catalyze this process to generate a tissue-specific DNA methylation pattern. This process has diverse results depending on where DNA methylation occurs.
In the context of CTCs, the DNA methylation profile allows for a molecular and biological perception of CTCs’ nature and tumor metastasis. 132 Zhao et al. assessed CTC DNA methylation in lung cancer patients. They characterized CTCs by comparing the methylation status of matched primary cancers with normal tissues. 25 In a separate study, Zavridou et al. and colleagues focused on the methylation of GSTP1 (a cell cycle regulator) and RASSF1A (a tumor suppressor gene) in EpCAM-positive prostate cancer CTCs and exosomes. Hypermethylation of GSTP1 and RASSF1A in CTCs was significantly associated with poor OS in prostate cancer patients. 226
CTC methylation signatures have proven to be an incredibly reliable way of characterizing CTCs in lung adenocarcinoma (LUAD) and squamous cell carcinoma (SCC) (LUSC). Jiang et al. performed WGS on CTCs from samples of six NSCLC patients, and they matched the CTCs to healthy lung tissues and white blood cells. They discovered two inheritance and evolution methylation patterns for CTCs during migration, providing a new understanding of NSCLC metastasis. 227 These findings suggest that studying the epigenetic state of CTCs could be useful for understanding the genomic modification of CTCs. This could considerably impact clinical outcomes by improving treatment in patients who do not respond effectively to traditional medicine.
Transcriptomic characterization
Single-cell RNA sequencing
Every tumor cell has its own set of somatic abnormalities, transcriptional architects, and epigenetic alterations. Tumor cell differences are considerably more pronounced at the RNA level, where these changes and their combinations are seen. 228 Bulk RNA collected from large-cell populations or homogenized tissue biopsies is used in standard RNA sequencing (RNA-seq) workflows to ensure sufficient RNA strands are present in the sample. Since it is performed in a pooled cell population with great diversity, bulk RNA sequencing can offer an unspecified quantity of gene expression. 229 On the other hand, single-cell RNA sequencing (scRNA-seq) can do transcriptome analysis on each individual cell with great throughput and resolution. It is possible to extract transcripts from isolated single cells, construct sequencing libraries, and then investigate the function and development of single cells using this unique approach (Table 2). 230
A few established mechanisms for explaining CTC formation, release, and metastasis could be identified using scRNA-seq.98,104 Aceto et al. used scRNA-seq for human breast cancer CTC clusters. They recognized that plakoglobin (a cytoplasmic component involved in adherent junction structures) is the key participant in CTC cluster formation, demonstrating the heterogeneous expression profiles in the primary tumor. In a mouse model, blocking plakoglobin prevented the formation of CTC clusters. CTC clusters wrap original tumor cells inside themselves, protecting them and helping them spread. Thus, RNA-seq can assist in understanding how changes in the expression of specific biological components can reflect CTC and CTC cluster metastatic potential. 75 They also identified CTC-WBC clusters in mice models and used RNA-seq to investigate the relationship between CTCs and neutrophils in CTC-WBC clusters. This group discovered that CTCs in clusters with WBCs express multiple genes at different levels, aligning the cell cycle process and promoting metastasis. 128
Another study showed that CTCs in HCC employ various strategies for immune evasion, such as EMT, immunosuppressive chemokines production, and cloaking clusters with platelets. CCL5 is the most upregulated gene in CTCs and is associated with immunity. CCL5 is typically involved in recruiting regulatory T cells (Tregs) in many malignancies. Patients with a high proportion of Tregs and increased CCL5 CTCs had a lower chance of remission and OS. The results of scRNA-sequencing in vivo and in vitro models indicated that CCL5-secreting CTCs could enhance immune-suppressive reactions. They also found that blocking the p38-Max signaling pathway considerably reduced tumor development and spread in HCC patients. 231 Thus, scRNA-seq is a useful tool for analyzing metastasis at the transcriptome level, assisting in developing anti-metastasis medication.
One of the most recent innovations in this field is hydrodynamic scRNA-seq (Hydro-seq), which addresses the weakness of existing scRNA-seq methods, such as limited throughput and poor cell capture efficiency (Table 2). This technology traps the cells based on their size, allowing us to collect more than 70% of CTCs. In the context of CTCs, hydro-seq can uncover transcriptome heterogeneity of biomarkers in many cancers, allowing targeting the metastasis and follow-up on specific therapies in patients.
Proteomics
Proteomics is the study of protein structures, location, function, and interactions. Proteins undergo post-translational or transient concentration changes in every cell based on their function. Although human cells have comparable genomic sequences, several cell types and subpopulations have phenotypic and functional differences, particularly in cancer cells. Therefore, single-cell level proteomics could pave the way for a comprehensive assessment of heterogeneity in cancer cells. 232
Developed instrumentation and sample handling techniques in mass spectrometry have facilitated the development of extensive single-cell proteomics analysis systems. 23 Multiplexed and quantitative calculations of proteins and their changes are possible using mass cytometry via inductively linked plasma time-of-flight mass spectrometry (CyTOF). This method allows for the quantitative measurement of more than 35 proteins within a single cell. 233 Herr et al. developed a single-cell resolution western blot (scWB) technology that detects a group of proteins in primary estrogen receptor-positive (ER+) breast cancer. Single-cell scWB can detect intracellular and surface signaling proteins, as well as alterations in their expression profiles of CTC populations. Thus, scWB enables a wide range of single-cell protein studies, from CTC biology to tracking a patient’s response to therapy (Table 2). 234
High-definition single-cell analysis (HD-SCA) is another mass cytometry technique that facilitates subsequent multiplex proteomic analysis. 235 Aside from minor limitations, the biggest barrier to HD-SCA is the low number of proteins that are evaluated using this technology. To address this, serum and blood proteins are analyzed using the proximity extension assay. This technology has demonstrated excellent readout specificity and sensitivity, allowing higher multiplex assays with coverage across a broad range while using a small volume of samples. 236
Circulating tumor DNA
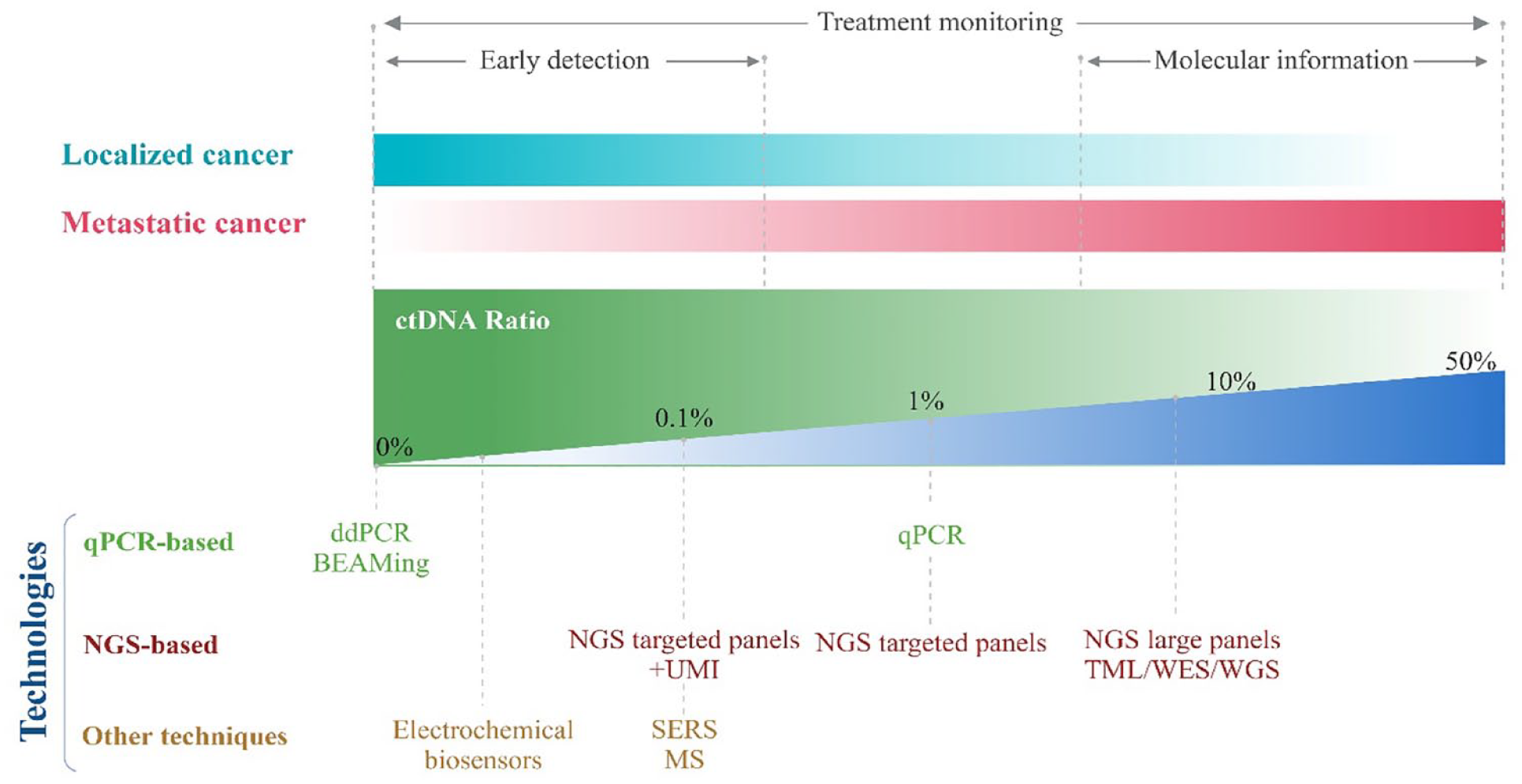
Circulating cell-free DNA (cfDNA) is shed actively and passively from cells and detected in biofluids such as serum, plasma, urine, cerebrospinal fluid, and pleural fluid. These are double-stranded short extracellular DNA (70–200 base pairs), a small percentage of cfDNA (0.01% of total non-cell DNA), known as circulating tumor DNA (ctDNA), which carries tumor-specific molecular changes and has been explored for detection of cancer-specific markers in cancer samples.237,238 ctDNA is highly fragmented, associated with nucleosomes and is released into circulation through apoptosis, necrosis, secretion of tumor cells and CTCs or metastatic lesions. 239 The staging and type of cancer are prominent determinants of circulatory ctDNA levels. Studies have established that ctDNA levels are significantly elevated in cancerous samples compared to healthy populations and vary with cancer progression stages. Factors like tumor size, metabolism and proliferation also correlate with the amount of ctDNA in plasma. 240 In the context of liquid biopsy, ctDNA is one of the more preferred tumor biomarkers because of its accuracy, sensitivity, and is also a valuable tool for early-stage cancers. 241
Despite this, implementing ctDNA analyses in clinical settings experiences critical challenges, including very low concentrations and differentiation from cfDNA to detect rare mutations precisely. The ratio of ctDNA is as low as 1–10% of cfDNA at advanced diseased stages and <0.1% at early stages. 238 The variability in concentrations of ctDNA in circulation also hinders the definition of a concentration range for detection. 242 The half-life of ctDNA is short, indicating that the ctDNA concentration in the biofluids reflects the tumor’s dynamic changes in real time. 243 Cancerous patients typically witness a cascade of genetic alterations, including the activation and inactivation of multiple oncogenes and tumor suppressor genes, which are reflected in ctDNA released into circulation. ctDNAs reflect tumor heterogeneity and are crucial for detecting genetic alterations in real time, including point mutations, insertions, deletions, and epigenetic modifications. 244 Studies have also established the relevance of ctDNA in monitoring the efficacy of treatments and identifying acquired resistance mutations allowing for the assessment of disease progression, minimal residual disease (MRD), and early detection of disease and recurrence. 87
Conventional strategies for ctDNA analysis
Several approaches have been explored for the isolation and analysis of ctDNA. The main conventional techniques for ctDNA analysis are PCR, including digital PCR (dPCR) and Amplification Refractory Mutation System (ARMS), beads, emulsions, amplification and magnetic analysis (BEAMing), and NGS.245,246 Digital and Quantitative PCR (qPCR) are the most commonly used methods for detecting rare and allele-specific mutations. 247 The more recently developed ARMS is also integrated with qPCR to detect low concentrations of mutant alleles. 248 NGS provides a full profile of genetic modifications caused by tumor evolution without needing prior knowledge. Common NGS panels cover a high number of targeted genes and are able to reach a detection threshold of ~1–2%. ctDNA can also be analyzed by covering the total genome using WGS. 249
Robust qPCR and sequencing strategies have facilitated ctDNA-based detection of variants and phenotypic characterization of key driver genes like KRAS, BRAF, ALK, and identify key mutations like L858R and T790M (linked to resistance) to predict targeted therapeutic options for non-small-cell lung cancer patients (NSCLC).250,251 KRAS mutations occur in >90% of pancreatic cancer and increasing levels of these mutations during and post-treatment are associated with worse PFS and OS.252,253 For prostate cancer screening, integrating the detection of KRAS mutations with an NGS-based panel for some mutations such as BRAF, CDKN2A, SMAD4, ROS1, and TP53 could enhance ctDNA detection and reliably reflect the response to therapy.254,255
These technologies have enabled the deployment of ctDNA analyses in clinical settings due to their development and improvement. In this regard, the FDA has approved a few products for clinical usage. These include two PCR-based approaches – Therascreen PIK3CA PCR kit (Qiagen, Hilden, Germany) for breast cancer samples and Cobas EGFR Mutation Test V2 (Roche Molecular Systems, CA, USA) for NSCLC patients and two NGS-based kits – FoundationOne Liquid CDx test (Foundation Medicine, Cambridge, MA) for solid malignant neoplasm patients and Guardant360 CDx (Guardant Health, California, USA) for NSCLC patients.256,257
Targeted techniques, such as digital PCR, offer greater sensitivity but require prior knowledge of the mutational profile of patient tumors. In contrast, non-targeted techniques, such as WGS, assess genome-wide genetic abnormalities. However, the latter requires more ctDNA than targeted techniques, which is impractical for cancer detection at an early stage. 258 While techniques like PCR and NGS offer limited sensitivity, deep sequencing strategies like Cancer Personalised Profiling by Deep Sequencing (CAPP-Seq) offer ultra-sensitive detection; however, the system is not cost-effective or time-efficient. 259 Despite the potential of ctDNA, technical challenges restrict the development of liquid biopsies based on ctDNA. Significant barriers include its intrinsic scarcity and the absence of pre-analytical sample preparation and purification. 260 Current technologies are focused on developing one-step integrated approaches for isolating ctDNA without causing ctDNA degradation or cell lysis.
Microfluidics-based ctDNA analysis
Although focused methods such as NGS, BEAMing, and dPCR have improved the sensitivity of detecting low-frequency changes in ctDNA, the lack of standards for the best DNA extraction precludes their use in clinical procedures. 261 Miniaturization of these procedures into a single device will allow for simpler and faster isolation of nucleic acids. Microfluidic systems allow for fluid manipulation at a micrometer scale, potentiating detection at the single molecule level (Figure 4). 262 Moreover, microfluidic platforms facilitate enhanced automation and high-throughput screening so that many patient samples can be screened in a short time frame. 263 Several studies have designed microfluidic platforms that have allowed for the isolation, detection, and characterization of ctDNA. 264
Conventional technologies implemented for ctDNA analyses and their feasibility toward clinical applications.
Enrichment and isolation of ctDNA
Solid phase extraction
Microfluidic devices have been created to capture nucleic acids via solid phase extraction based on functionalized surfaces, silica membranes, and beads. 265 Campos et al. designed a UV/O3-activated solid phase extraction microfluidic device (SPE) with surface-bound carboxylic acid capabilities. The technique used micropillars and an immobilization buffer to induce cfDNA condensation onto the active microchip’s surface. The device achieved ~70–90% recovery of DNA fragments and also successfully detected KRAS mutations in plasma samples of NSCLC patients. 266
In a similar concept, Jin et al. integrated a microfluidic system with Sanger Sequencing to identify mutation profiles in CRC patients. The system is composed of a dimethyl dithiobispropionimidate (DTBP)-based microchannel platform that enabled the capture of cfDNA without cellular background. The platform identified 71.4% of mutations of KRAS and BRAF from CRC of patients within 15 min. 267 Magnetic beads have also been used for ctDNA isolation. These particles are used because of their high surface area to volume ratio and ease of manipulation in stationary or laminar liquid flow under a magnetic field. The surface of these particles is commonly functionalized with silica or cationic polymers and/or specific oligonucleotide sequences to interact with negatively charged ctDNAs. 268 Gwak et al. created an integrated microfluidic platform that uses magnetophoresis to boost the likelihood of DNA fragments adhering to silica-coated magnetic particles. 269
Liquid phase extraction
Liquid phase separation chips rely on nucleic acid mobility as a result of electrophoresis principles or chemical solutions. 263 In dielectrophoretic (DEP) microchips, charged particles are dielectric or uncharged and move under the influence of a non-uniform electric field. 62 To extract circulating cfDNA from the plasma samples of patients suffering from chronic lymphocytic leukemia, Manouchehri et al. created a dielectrophoresis microarray chip. Within 20 min, the experiment successfully identified cancer-specific mutations in the SF3B1, NOTCH1, and TP53 genes from as little as 25 ul of plasma. 270 More recently, a microfluidic pressure immiscibility-based extraction system was reported to extract cfDNA from the blood plasma of HER-2 type breast cancer samples and detect mutation fractions in PIK3CA. The system’s silica membrane allowed it to function at a low vacuum pressure and achieve recovery rates comparable to traditional extraction kits while greatly lowering processing time by doing away with the need for repeated centrifugation procedures. 271
Quantification and detection of ctDNA
The absolute concentration of ctDNA and identifying specific mutations in its genetic profile is a potential technique for tracking cancer progression and detecting drug-resistant mutations to provide personalized medicine. 263 Toward this, several studies have integrated microfluidics with digital PCR-based techniques to enhance the detection of mutation rate and overall sensitivity of circulating nucleic acids. 272 Digital microfluidic approaches have also been implemented toward detecting and assessing intermolecular heterogeneity of DNA methylation, achieving higher analytical sensitivity than other PCR assays, thus facilitating a simple and cost-effective medium for quantifying DNA methylation. 271
Droplet digital PCR (ddPCR) is the most prevalent microfluidics technique for ctDNA analysis. A microfluidic chip facilitates preparing the sample by water–oil emulsion and partitioning the PCR into individual nanoliter-sized droplets. This strategy achieved a detection limit (LOD: 0.001%) lower than conventional PCR methods and more precise and reproducible results. 263 Microfluidic ddPCR technology has also been implemented to monitor the evolution of EGFR alterations by detecting T790M mutations in NSCLC patients receiving tyrosine kinase inhibitors (TKI) therapy. 273 In a similar work, Zhang et al. performed a clinical trial comparing EGFR T790M mutation detection in NSCLC patients using ARMS and ddPCR. Both methods achieved an overall concordance of 78.3%, with ddPCR reporting higher sensitivity. 274
For sensitive ctDNA analysis, Wu et al. recently developed a PCR chip with embedded microwells and a self-powered bidirectional partition network. The bidirectional delivery network facilitated the rapid and random distribution of targets. With a sensitivity of 85.71% and specificity of 94.4% for L858R mutations and 100% sensitivity and 86.96% specificity for T790M mutations, the microfluidic chip detected EGFR modifications in blood samples. 275 Targeting the same EGFR T790M mutations, studies have also reported developing fully automated and integrated ‘sample-to-answer’ ctDNA-based liquid biopsy platforms using ddPCR. These strategies integrated both ctDNA isolation and detection of specific mutations in a single system facilitating rapid, point-of-care ctDNA analysis that can be implemented in routine clinical settings. 276
Apart from microfluidic dPCR, several other strategies have been reported for ctDNA analysis. Electrochemical methods have been explored to detect and analyze multiple cancer-specific circulating nucleic acids and detect DNA methylations and mutations. 277 Electrochemical biosensing applications like Differential Pulse Voltammetry and Electrochemical Impedance Spectroscopy have been implemented toward the detection of ctDNA (KRAS and PIK3CA genes) while achieving a low detection limit and rapid response, potentiating their application in point-of-care settings. 278
Koo et al. designed an integrated approach that allows the targeted study of numerous prostate cancer genetic abnormalities.279,280 The integrated biochip allowed for the electrical release of cellular contents, allowing for quick, one-step target capture and isothermal amplification. In the system for electrochemical measurements, superparamagnetic iron oxide particles were used as stable nonbiological peroxidase-mimicking nanozymes, allowing multifunctional cancer risk prediction and cancer relapse monitoring. 280 Surface-enhanced Raman scattering (SERS) has also emerged as a viable medium for biomarker detection. It has a restricted bandwidth and a particular molecular spectrum, allowing for strong amplification of the Raman scattering effect. 281 The amplification is driven by areas of significant electromagnetic field enhancement (referred to as ‘hot spots’) formed at connections between metallic nanostructures via localized surface plasmon resonance. 282 SERS-based sensors integrated with specific nanomaterials and amplification techniques like PCR have shown promise for detecting ctDNAs, including BRAF and KRAS. 283
Using a similar strategy, Cao et al. developed a high-throughput microfluidic system for highly sensitive SERS-based detection of gastric cancer-associated ctDNA. In the reaction region of the chip, products generated by the target triggered CHA (catalytic hairpin assembly) initiated the hybridization chain reaction (HCR), forming dsDNAs on the Au nanobowl array to which numerous SERS probes were attached. This generated numerous ‘hot spots’ around the nanobowl surface, significantly enhancing the SERS signal intensity. The system achieved an ultrasensitive detection limit of 1.26 aM for PIK3CA E542K and 2.04aM for TP53 genes and the process was completed in 13 min with results comparable to qRT-PCR. 284 A recent study implemented a similar concept where a SERS microfluidic chip integrated with CHA to detect NSCLC-related ctDNAs (TP53 and PIK3CA-Q546K) simultaneously. The reaction was completed within 5 min and achieved a detection limit of 2.26 aM for TP53 and 2.34 aM for PIK3CA-Q546K in human serum. The results were also validated and comparable to conventional qRT-PCR assays. 285 These results demonstrate the promise of SERS-based microfluidic chips for rapid, cost-effective, and highly sensitive ctDNA detection, as well as the possibility for deployment toward dynamic cancer staging monitoring and a viable clinical tool for early cancer screening (Figure 5).
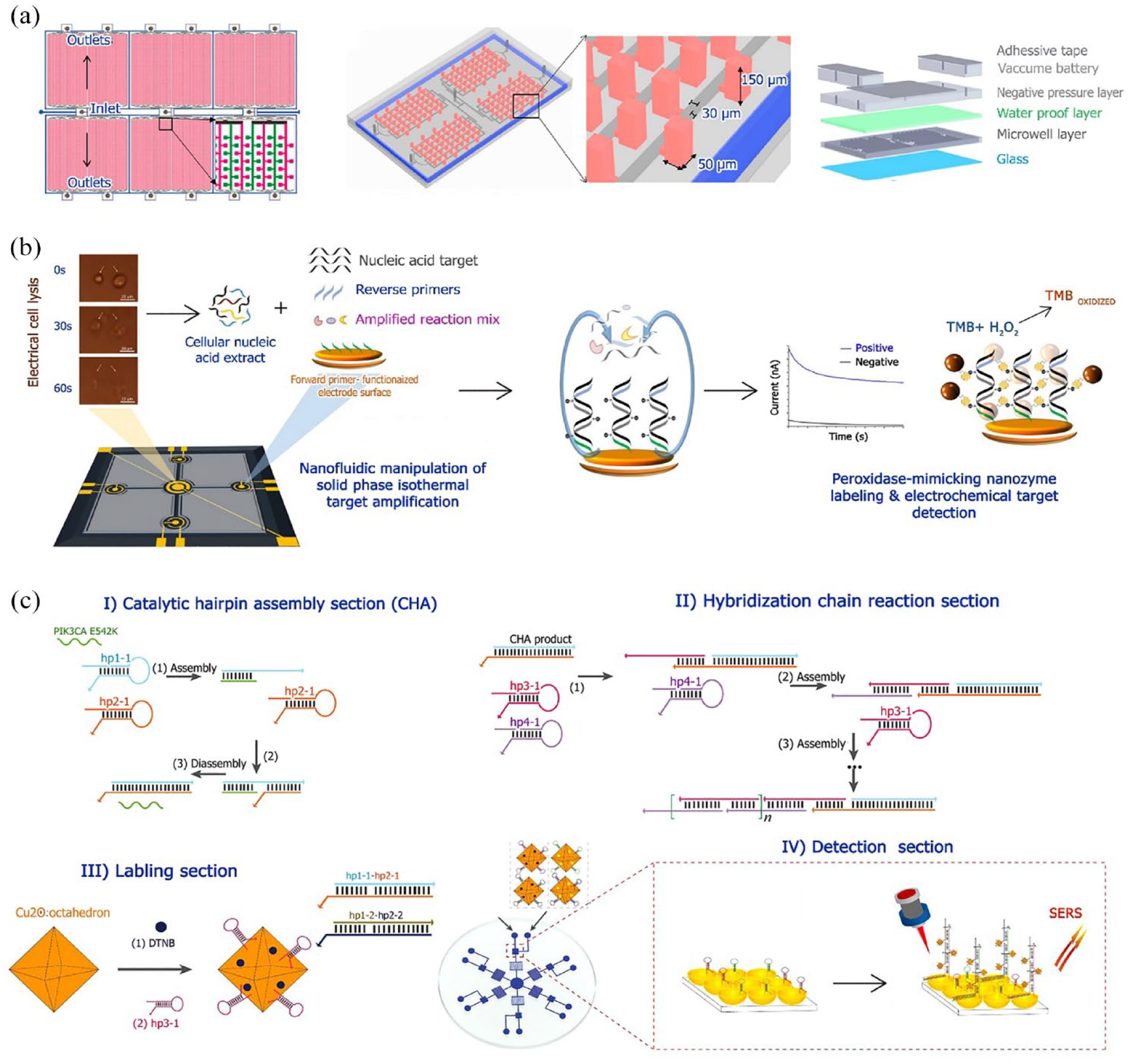
Novel strategies for integrated detection and quantitation of ctDNA. (a) Schematic of self-powered bidirectional partition microfluidic chip with embedded microwells. A layered microfluidic chip was designed such that the sample was loaded into the chip through the inlet and distributed into microwells in two directions. The microchannels connected to the red channel are alternatively embedded in the row of microwells linked to the channel. The embedded microwells allow decreasing of the blank area on the chip without shortening the interval of alternate microwells. The blue line around the array denotes the hydration channel. Reproduced with permission from Geng et al. 276 under open Creative Commons Attribution License. (b) Integrated biochip equipped with central lysis and four amplification/detection chambers linked by the fluidic channels for targeted ctDNA analysis. The on-chip electrical cell lysis releases cellular targets and the nanofluidic manipulations are under an AC field to enhance isothermal solid phase amplification. Superparamagnetic iron oxide particle nanozyme-mediated redox reaction allows for electrochemical detection of surface-immobilized amplicons. Reproduced with permission from Koo et al. 280 Copyright 2020 American Chemical Society. (c) Schematic illustration of the pump-free, high-throughput microfluidic chip-based SERS assay for ctDNA detection. The chip was developed with Cu2O octahedra and an AuNB array as the SERS-active substrate and CHA-HCR as the dual amplification strategy. Reproduced with permission from Cao et al. 284 under open Creative Commons Attribution License.
Studies looking at ctDNA-guided MRD assessments often use tumor-informed next-generation sequencing-based techniques. In trials attempting to assess MRD in individuals with early-stage CRC, three major ctDNA assays have been described. Signatera is the latest tumor-informed customized test 286 plus droplet digital PCR-based assay (ddPCR) and safe sequencing (SafeSeq). 287 The tumor-informed assays involve sequencing the tumor to identify specific alterations recorded in the plasma using ctDNA. While there is no clear superiority between these assays, ctDNA assays utilized for MRD evaluation are predominantly tumor-informed and exhibit strong analytical sensitivity, with a lower detection limit of 0.01%. This represents that these assays are capable of detecting a single DNA fragment derived from the tumor within a mixture of 10,000 DNA fragments.286,288,289 A study was done using a personalized and tumor-informed multiplex PCR assay, known as the Signatera™ bespoke mPCR NGS assay, to detect and quantify ctDNA. Among 258 patients, 67 (26%) samples were positive for ctDNA in their plasma. Thus, they concluded that there is a statistically strong correlation between the stage of disease, the number and location of metastases, and the rate of ctDNA positivity. In contrast with locoregional tumors (i.e. stage I–III), which exhibited a ctDNA positivity rate of approximately 20% in postoperative samples, stage IV GI cancers demonstrated 44% positivity. 290
In recent years, new techniques have been designed that involve supplementary features of cfDNA, besides mutations, that help with the identification of ctDNA. A beneficial method is to look into the length of cfDNA fragments, focusing on the fact that ctDNA is comparatively shorter than cfDNA from the main tumor.291,292 This approach has been employed to discover a fragmentation-based classifier at the patient level using shallow WGS data.293,294 In addition, it has aided in distinguishing mutation calls derived from tumors from others originating from clonal hematopoiesis in hybrid capture sequencing data.295,296 Increasing evidence suggests that the application of fragment length analysis may serve as a complementary approach to the conventional variant-based detection of MRD. The combination of fragment length analysis and variant tracing offers an opportunity to enhance the sensitivity of detecting MRD, as these two methods serve as independent read-outs for the presence of ctDNA. Vessies et al. reported the variations in fragment lengths between ctDNA and non-tumor cfDNA. ctDNA fragments were identified as those that included a tumor tissue-informed mutation, and 21,705 fragments were found in the plasma of 36 individuals. Consistent with prior research, the ctDNA fragments show shorter lengths compared to the cfDNA. As per previous research, the ctDNA fragments were observed to be shorter compared to cfDNA fragments from the control group. This includes both mononucleosomal and dinucleosomal fragments. Analyzing the relative prevalence of each fragment length between ctDNA and non-tumor cfDNA fragments helps determine if the fragment originated from a tumor cell or a non-tumor cell. 297
The potential of ctDNA in cancer diagnosis and treatment: clinical trials
In a clinical trial named BOLERO-2 (NCT00863655), the frequency of ESR1 mutations was assessed in extracted ctDNA from 541 metastatic breast cancer (BRCA) samples. In contrast to patients with wild-type ESR1, the authors attributed mutations to a less OS. Furthermore, D538G mutations are related to a shortened PFS compared to patients with wild-type ESR1. This shows that BRCA patients who have previously received Aromatase inhibitor have ESR1 mutations in ctDNA are likely to suffer from more aggressive tumors. 298 This research revealed that the PIK3CA mutational status showed a rate of 70.4% between paired archival tumor and cfDNA samples. Notably, a greater concordance of 81.6% was observed for metastatic lesions. 299
The main purpose of the PALOMA-3 trial (NCT01942135) was to reveal the advantage of palbociclib in conjunction with fulvestrant (Faslodex) compared to fulvestrant alone in terms of extending PFS in HR+, HER2− metastatic BRCA patients, who had experienced tumor progression following previously endocrine therapy. 300 The objective of the study was to assess the ctDNA mutations of PIK3CA and ESR1 in a set of patients before, during, and post-treatment with a CDK4/6 inhibitor. A combination of ddPCR, WES, and targeted sequencing collectively revealed a higher incidence of mutations in the post-treatment samples compared to the initial samples. Notably, at least one newly acquired mutation was detected in 30.8% of the post-treatment samples. The latest findings from the PALOMA-3 clinical trial indicate patients with significant levels of ctDNA have a worse PFS. The results suggest that the analysis of cfDNA might assist in making clinical decisions for patients with BRCA who are unresponsive to treatment. 301
The majority of lung cancer cases are not detected until they start showing symptoms, frequently when the disease is advanced and the chances of successful therapy are minimal. Regarding this, the MILD trial (NCT02837809) was started. It was prospective randomized controlled research with 4099 participants (aged 49–75) and a smoking history within the previous 10 years. This study combined quitting smoking with early diagnosis and biological evaluations. The findings show that lung cancer, regardless of stage, is strongly correlated with elevated levels of cfDNA. Surprisingly, measuring the ctDNA was unable to distinguish healthy controls or patients with additional tumors in small lung cancers. CtDNA levels have been found to be associated with disease aggressiveness and a poor prognostic predictor for survival. Furthermore, for tumors in Stage II–IV, the measured ctDNA was much higher than the baseline level and after surgery. According to these findings, ctDNA levels can be used to predict lung cancer prognosis at any stage of the disease. 302
As a prospective study, ECLIPSE (NCT04136002) assessed the efficacy of the LUNAR test within the population with an average risk of CRC. LUNAR can identify the genome and epigenome alterations by analyzing plasma samples in a single assay. ECLIPSE employs a comprehensive approach that effectively integrates somatic variant identification, epigenomic assessment, and bioinformatic classifying to exclude non-tumor variants. The results revealed that detecting ctDNA in patients with stages I–III of CRC exhibited 94% specificity. Furthermore, epigenomic investigation substantially improved the detection of ctDNA compared to applying only somatic mutational analysis. 303
Clinical application of ctDNA
Regarding current literature, the clinical utility of ctDNA can be divided into two main categories: qualitative and quantitative analyses. Although much research has been done on quantitative evaluation, clinical applications have mostly relied on qualitative aspects of ctDNA. The employing of qualitative features of ctDNA is also employed for the identification of resistance mutations, which function as unfavorable prognosticators of the response to specific therapies. However, quantitative analysis of ctDNA is applied to resistance mutation identification as negative response predictors to therapy. For example, EGFR antibody-based therapies predict the response using KRAS mutation assessment or ESR1 mutations in HR+ BRCAs that indicate resistance to specific endocrine therapies.304,305
It has been observed that around 40% of BRCAs that are positive for and negative for HER2 display mutations in the PIK3CA. These mutations are significant in the administration of alpelisib, a PI3Kα-specific inhibitor, alongside with fulvestrant. 306 The guidelines suggest the evaluation of PIK3CA mutations through tumor tissue or ctDNA. Indeed, the reassessment of PIK3CA within the plasma is crucial, as its mutational status can differ upon the recurrence of the disease. 307
The analysis of ctDNA offers promising potential for coming applications, particularly in the case of prostate cancer patients. Olaparib, a PARP inhibitor, is FDA approved for metastatic, castration-resistant prostate cancer who have deleterious or suspected deleterious germline or somatic homologous recombination repair gene mutations. 308 Rucaparib is also approved for individuals diagnosed with metastatic castration-resistant prostate cancer (mCRPC) who possess deleterious somatic and/or germline BRCA mutations. 309 Plasma ctDNA analysis is expected to be helpful for identifying the subgroup of patients who are candidates for these treatments. Also, ctDNA screening has been used to investigate primary resistance to abiraterone and enzalutamide, along with the molecular changes related to neuroendocrine metamorphosis. 310
It is shown that ctDNA MRD detection is extremely prognostic following definitive therapy for solid tumors and has a high predictive accuracy for the probability of occurrence. The clinical sensitivity, including disease recurrence and ctDNA-positive cases after therapy, approached 100% in most trials. Another significant benefit of the ctDNA MRD test is that residual disease was detected quite earlier than with conventional radiological imaging. 311
Challenges and future directions
Despite ctDNA’s promising future and great momentum as a cancer prevention and therapy tool, several hurdles remain. From the instrumental perspective, the time of turnaround and the cost of operation is still high, while the specificity should also increase. Regarding the technical view, conversely, ctDNA specification for MRD and monitoring of the primary tumor are still challenging. As with other technologies, increasing the speed of NGS and lower costs continue to be the norm. Therefore, these difficulties are likely to be addressed in the near future. 312
However, not detecting ctDNA in the patient samples who are receiving curative treatment cannot be associated with a cure. 313 Moreover, ctDNA can be heterogeneous, as various mutations with different frequencies might happen in distinct regions of the tumor. This can hurdle the disease assessment and also monitor the treatment response. 314 In addition, being contaminated with non-cancerous DNA could be another challenge in using ctDNAs. 315 Overall, developing current methods and inventing new technologies with high sensitivity and resolution can improve the ctDNA application in cancer detection and monitoring.
Machine learning-based detection
The improvement of cancer-based diagnostics has resulted in the generation of large data sets, including genomic and proteomic analyses. 316 Artificial intelligence (AI), including machine learning (ML) algorithms like linear discriminant analysis, principal component analysis (PCA), and deep learning, have been implemented in biomarker discovery and digital pathology. 317 AI-integrated systems allow for complex, multiplexed data analysis that can identify and quantify relevant biomarkers that would be impossible by conventional methods. 258 Toward this, Lim et al. demonstrated the impact of intratumoral heterogeneity in predicting the recurrence of NSCLC. The researchers used a label-free microfluidic single-cell CTC collecting device in combination with sequencing and ML techniques to detect distinct genetic signatures and analyze expression profiles in various cancer patients. 318
Similar concepts have been explored in developing integrated systems that combine machine learning-based models with optimized microfluidic systems to detect CTCs. 319 ML algorithms have also been integrated with microscopy techniques for microfluidic label-free detection of specific CTC populations in the background of blood cells. 320 More recently, Wang et al. implemented a deep convolutional neural network-based ML algorithm for classifying images acquired from patient blood samples to detect rare CTCs. The system required minimal pre-processing of data and achieved high accuracy in identifying rare CTCs. 321 Automated ML platforms have also been implemented to analyze liquid biopsy data from DNA, RNA and proteins in the blood, serum, and plasma patient sample. 322
Cohen et al. developed a blood testing system called CancerSEEK that successfully detected multiple cancer types by integrating AI to assess circulating proteins and mutations in cfDNA. The study achieved a specificity of ~99% and a sensitivity of 69–98% in detecting five types of cancer. 323 Recently, Lee et al. devised a highly sensitive cfDNA detection system integrated with a PCA ML algorithm to allow for improved diagnosis and prognosis of hepatocellular carcinoma (HCC). The study established a cfDNA score (cfDHCC) that integrated total plasma cfDNA levels and cfDNA that expressed AFP into a single score using ML algorithms for improved diagnostic/prognostic accuracy. 324 ML and deep learning methods have also been implemented toward detecting DNA methylation markers in low amounts of ctDNA, allowing for cancer screening and assessment of treatment efficacy. 325 A common limitation in ML-based studies is the limited sample size that does not adequately capture the heterogeneous genome aberrations in liquid biopsy assays. Since training ML algorithms necessitate large data sets to improve their performance, acquiring representative samples of biomarkers to generate highly sensitive tests is essential. 258 Novel systems combining liquid biopsy platforms with AI and ML algorithms allow for the development of accurate, simple to use, and comparatively cheaper diagnostic methods that can potentially enable precision diagnostics and improved cancer management.
Conclusion
Liquid biopsy represents a more reliable cancer diagnostic system with a minimally invasive sampling process compared to traditional tissue biopsies. Toward this, multiple studies have emphasized the prognostic and therapeutic utility of CTC and ctDNA detection, enumeration, and characterization. Despite the progress in CTC and ctDNA-based studies, the translation of current isolation and characterization systems in clinical practice is limited. Patients’ availability, quality, and tumor tissue size have hampered the clinical application of targeted therapies. Furthermore, tumor heterogeneity is a concern because a single biopsy cannot reveal the entire genetic variability of a patient’s tumor. 326 One of the major problems that should be solved before CTC processing is implemented in clinical settings is CTC isolation and enrichment. 327 Inconsistencies in CTC data across similar patient cohorts and numerous CTC detection technologies, as well as the difficulty in repeating CTC investigations, are also concerns to consider as obstacles for CTC clinical trials. 328 Future studies exploring the feasibility of these biomarkers in interventional clinical settings must be prioritized, despite the fact that characterization of CTCs and ctDNAs using genomic, transcriptomic, and proteomic approaches has shed much light on tumor heterogeneity and treatment resistance.