
Abstract
Background:
In the intensity-modulated radiotherapy (IMRT) era, the survival benefit of concurrent chemotherapy for locoregionally advanced nasopharyngeal carcinoma (LA-NPC) remains undetermined. This study aimed to evaluate the benefits of IMRT with concurrent chemotherapy compared with IMRT alone for LA-NPC patients with different plasma Epstein–Barr virus (EBV) DNA levels.
Methods:
Patients were identified from a prospectively maintained database in an endemic area between November 2002 and December 2013. Cox proportional hazards models, propensity score matching, and inverse probability weighting models were established for survival analysis. Stratification analysis was performed based on interaction effects analysis. Finally, sensitivity analysis was performed considering unmeasured confounders.
Results:
A total of 1357 eligible patients were enrolled (median follow up 62.4 months; range 3.5–155.8 months). No significant survival differences were observed between groups in the entire cohort. Notably, a significant interaction effect was observed between treatment regimens and EBV DNA levels. In patients with high EBV DNA levels (>4000 copies/ml), all three models showed that IMRT with concurrent chemotherapy significantly improved overall survival [hazard ratio (HR) 2.521, 95% confidence interval (CI) 1.218–5.216], disease-free survival (HR 2.168, 95% CI 1.349–3.483), and distant metastasis-free survival (HR 2.331, 95% CI 1.194–4.551) compared with IMRT alone. No differences were found in patients with low EBV DNA levels. Sensitivity analysis confirmed the robustness of the results.
Conclusion:
In the IMRT era, concurrent chemotherapy treatment of LA-NPC patients with high EBV DNA levels is reasonable. However, the optimal regimen for LA-NPC patients with low EBV DNA levels needs further validation in randomized clinical trials.
Keywords
Introduction
Nasopharyngeal carcinoma (NPC) is a distinct type of head and neck cancer originating from the epithelium of the nasopharynx with high metastatic and invasive potential. NPC is endemic in certain areas of southern China and Southeast Asia, with an incidence of 20–50/100,000. 1 Radiotherapy (RT) with concurrent chemotherapy (CCRT) is recommended as the standard treatment for locoregionally advanced NPC (LA-NPC), which accounts for approximately 80% of NPC cases at the initial diagnosis. 2 In the conventional two-dimensional RT (2DRT) era, CCRT was confirmed to increase the tumour control rate, reduce metastasis and ultimately improve the long-term survival of LA-NPC patients.3,4
However, CCRT is associated with enhanced severe acute and late toxicities compared with radiotherapy alone. For example, CCRT increased acute toxicities and impaired treatment compliance.5,6 With a relatively high cure rate of nonmetastatic NPC and a long survival time, CCRT patients present more generalized and severe late toxicities. Severe late toxicities can reduce the quality of life or even be life threatening. A meta-analysis based on randomized controlled trials indicated that CCRT was associated with a higher rate of late toxicities than RT alone. 7
Over the last two decades, intensity-modulated RT (IMRT) has been widely utilized for the treatment of NPC. Compared with 2DRT, IMRT can significantly improve overall survival (OS) and reduce metastasis and the incidence of toxicities in organs at risk (OARs), 8 especially for tumours located in a complex anatomic site, such as NPC. Previous studies have reported that local and regional control rates have exceeded 95% for NPC patients in the IMRT era.9,10 Recently, several studies have reported that combining concurrent chemotherapy with IMRT does not improve patient survival compared with IMRT alone,8,11,12 although one study reported a positive conclusion. 13 Thus, a reasonable question is whether concurrent chemotherapy remains necessary and beneficial for the treatment of NPC in the IMRT era despite chemotherapy-induced toxicities in a real-world setting.
Quantification of pretreatment plasma Epstein–Barr virus (EBV) DNA levels has been shown to be a useful biomarker for risk stratification, monitoring and prediction of the survival of NPC patients. 1 Based on previous studies, the plasma EBV DNA level has become a key complement for traditional TNM staging.14–17 This study aimed to investigate the benefit of CCRT for NPC patients with different plasma EBV DNA levels in the IMRT era.
Materials and methods
Study patients
This study was reviewed and approved by the Institutional Review Board and Ethics Committee of Sun Yat-sen University Cancer Center (SYSUCC), Guangzhou, China (approval number: GZR2016-210). Written informed consent for the use of clinical data and collected samples for future studies (including retrospective studies) was obtained when the patients were admitted to receive treatment as a general standard procedure for patients treated in our centre. All patient records were anonymous and de-identified before the analysis.
Using a prospectively created database, this study collected 11,558 consecutive patients with NPC at the SYSUCC between November 2002 and December 2013. The disease was restaged according to the International Union Against Cancer/American Joint Committee on Cancer (UICC/AJCC) TNM classification (seventh edition, 2011) based on clinical and radiographic data. The inclusion criteria included the following: (a) histologically confirmed NPC; (b) disease classified as stages II–IVB; and (c) the radiation delivery technique was IMRT. The main exclusion criteria were as follows: (a) a previous malignancy or concomitant malignant disease; (b) the use of adjuvant or induction chemotherapy or additional concurrent systemic therapy; (c) the radiation delivery technique was 2DRT; and (d) missing or incomplete clinical data. A total of 2875 newly diagnosed NPC patients with stage II–IVB disease were identified. Figure 1 shows detailed information for the study patients. Ultimately, 1357 patients were enrolled in this study for the analysis.
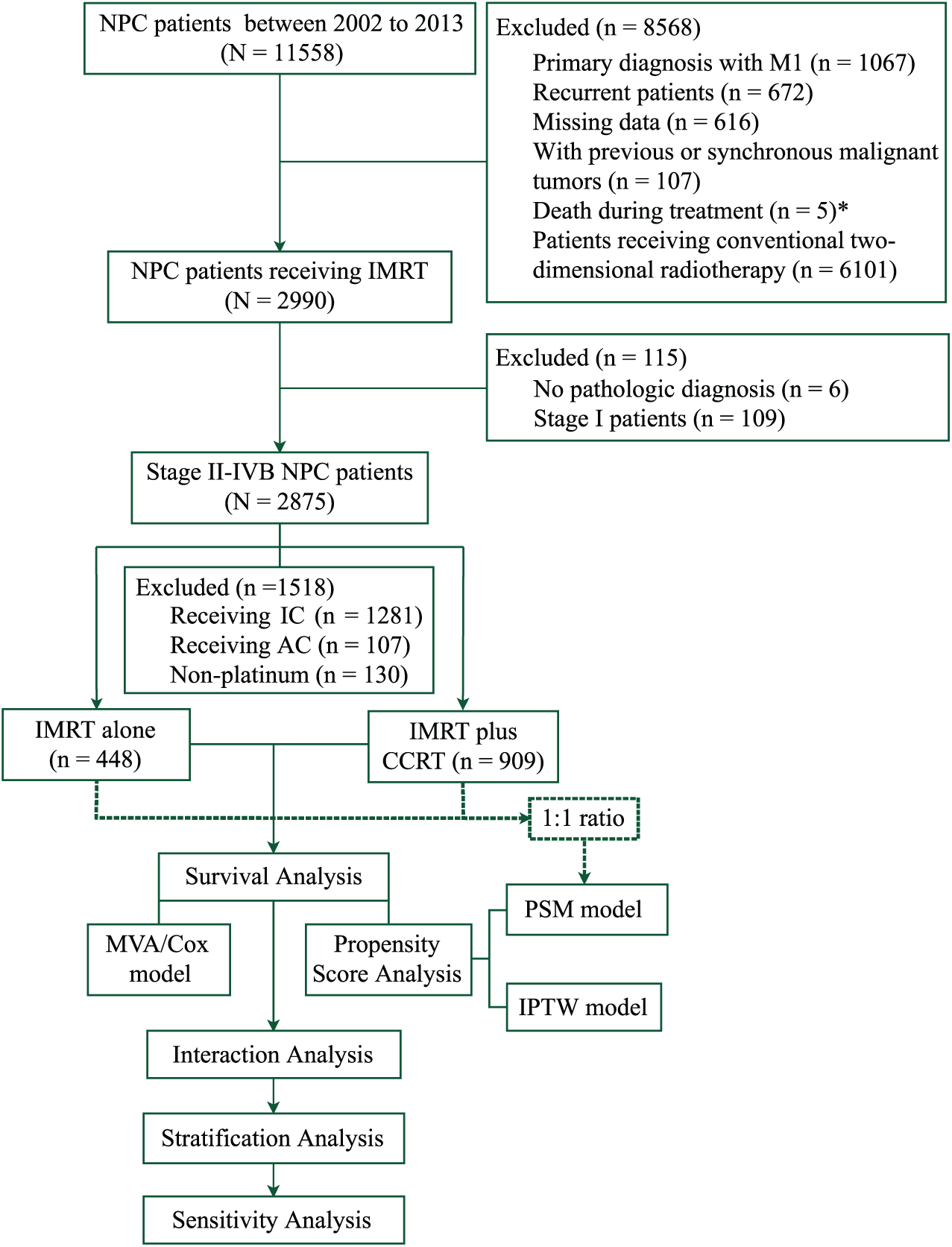
STROBE flow diagram. *Among the five patients who died during the treatment, three patients received two-dimensional conventional radiotherapy, one received induction chemotherapy, and one died from massive haemorrhage of the gastrointestinal tract after the 6th fraction of radiotherapy and one cycle of concurrent chemotherapy.
Real-time quantitative measurement of plasma EBV DNA
Pretreatment plasma EBV DNA was extracted and subjected to real-time quantitative polymerase chain reaction as described previously with the same measurement for all the measured patients.18,19 The pretreatment plasma EBV DNA levels were routinely assessed for 940 of the 1357 patients prior to treatment. Overall, two groups containing low or high levels (defined by a cut-off level of 4000 copies per ml) were analysed in this study. This cut-off level was chosen because it was previously confirmed to be a prognostic threshold in NPC studies using the same measurement system in the same endemic area.14,17,20 Meanwhile, four groups defined by magnitudes of 10 were used to objectively create the survival analysis curves provided in the Supplementary Material [Supplementary Figure 1(a–d)].
Treatments and follow up
The pretreatment evaluation is presented in the Supplementary Material. All NPC patients were treated with IMRT according to the principle of treatment for NPC at SYSUCC. The patients were examined every 3 months during the first 3 years and then every 6 months thereafter or until death after treatment. Detailed information for the treatment and follow up is presented in the Supplementary Materials.
Clinical outcome definitions
The primary endpoint was OS, which was calculated from the date of histological diagnosis to the date of death from any cause. The secondary endpoints were disease-free survival (DFS), which was calculated from the date of diagnosis to the date of death or relapse due to the tumour, and distant metastasis-free survival (DMFS) or locoregional relapse-free survival (LRFS), which was calculated from the date of diagnosis to the date of distant metastasis or locoregional failure, respectively.
Statistical analysis
The Chi-square test was used to assess differences between two groups. Survival rates were estimated using the Kaplan–Meier method with the log-rank test. We used the following four complementary approaches to adjust our comparison of survival rates among patients receiving two regimens based on differences in baseline characteristics: a standard Cox proportional hazards model; the propensity score matching (PSM) model; the inverse probability of treatment weighting (IPTW) model; and a sensitivity analysis. All statistical tests were two sided, and p < 0.05 was considered significant. All statistical analyses were performed in R (R Foundation for Statistical Computing, Vienna, Austria; version 3.2.2).
In the multivariable analysis (MVA) with standard Cox proportional hazards models using the forward likelihood ratio method, we included all observed variables with clinical significance or a significant association with survival. 21 Then, we performed an interaction effect analysis between the treatment regimen and other variables. The stratification analysis was further performed based on the significant interaction effects.
Propensity score analysis
The propensity score analysis (PSA) adjusts for the bias induced by nonrandom treatment assignment by comparing patients who have a similar likelihood of receiving one treatment but who receive another treatment. We estimated the effect of treatment on survival using the following two PSA approaches: PSM and IPTW. Prior work has verified that both approaches allow for estimation of marginal hazard ratios (HRs) with minimal bias. 22
For the PSM analysis, we matched each patient who received IMRT alone with one patient who received IMRT with concurrent chemotherapy using the logit of the propensity score, using callipers of a width equal to 0.2 of standard deviations of the logit of the estimated propensity score. 23 To compare the groups, a marginal Cox model was applied using maximum partial likelihood estimates of regression parameters and a robust sandwich covariance matrix.24,25 The main limitation of PSM is that it limits the analysis to the matched cohort and thus reduces the statistical power. The IPTW model does not carry this limitation and instead uses the inverse probability of the treatment weights. For the IPTW model analysis, each observation was weighted using the inverse probability of receiving the treatment based on the propensity score. Then, a Cox proportional hazards model was fitted with the chemotherapy regimen as the only predictor variable. A robust sandwich variance estimator was used to account for the weighted nature of the sample. 26
Sensitivity analysis
Although propensity scores can address biases caused by observed variables, unknown or unmeasured variables (i.e. performance status and economic status), may also be associated with the receipt of chemotherapy and the prognosis. We performed a sensitivity analysis for the unmeasured variables in the aforementioned analysis to measure their potential confounding effects on our results and to validate the robustness of our analysis. 27 We varied the prevalence of a poor performance status and the adjusted mortality HRs in the two different regimens using estimates from prior studies of patients. 28 Based on these studies, we assumed that a performance status of 2 or greater would be associated with an HR of 1.2–2. Using these data, we calculated adjusted HRs and 95% confidence intervals (CIs) for the IMRT-alone regimen.
Results
Patient characteristics and follow up
The characteristics of the 1357 NPC patients, including 909 patients (67%) who received IMRT with concurrent chemotherapy and 448 patients (33%) who received IMRT alone, are presented in Table 1. The percentages of patients with clinical stage II, III, and IVA–B tumours were 25.9%, 54.7%, and 19.4%, respectively. No significant differences were found in the sex, body mass index (BMI), education, smoking, drinking, and comorbidity distributions (all p > 0.05), but differences were observed in the ages, EBV DNA levels, tumour and node stages, clinical stages, and year of diagnosis. Older patients (p < 0.001) and patients with earlier-stage tumours (p < 0.001) were more likely to receive IMRT alone than CCRT.
Baseline patient characteristics according to treatment in the entire cohort and in the propensity score-matched cohort.
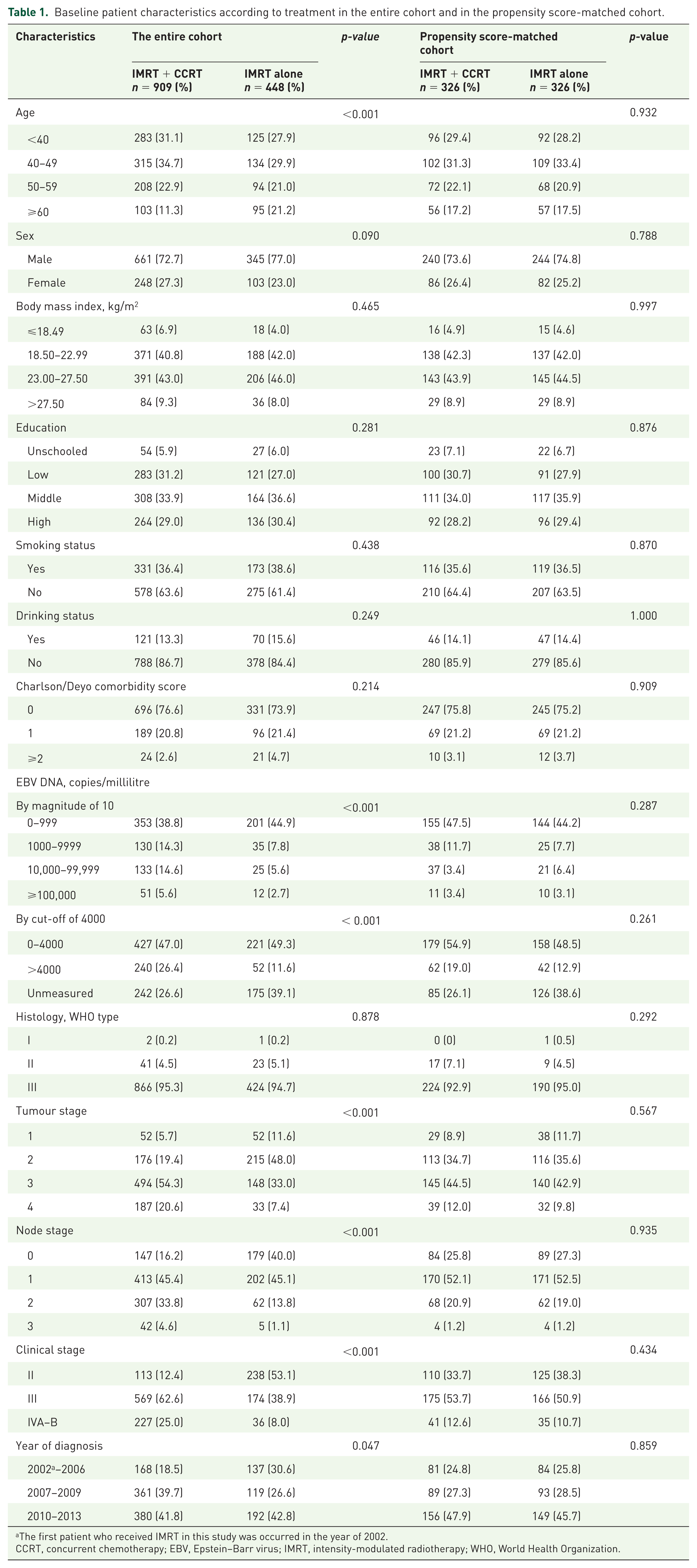
The first patient who received IMRT in this study was occurred in the year of 2002.
CCRT, concurrent chemotherapy; EBV, Epstein–Barr virus; IMRT, intensity-modulated radiotherapy; WHO, World Health Organization.
With a median follow-up time of 62.4 months (range 3.5–155.8 months), 145 (10.7%) of the 1357 patients developed a distant metastasis, 100 (7.4%) patients developed local regional recurrence, and 159 (11.7%) patients died. The 5-year OS, DFS, DMFS and LRFS rates in the entire cohort were 89.9%, 80.0%, 89.7%, and 92.7%, respectively.
Prognostic value of the plasma EBV DNA level
The plasma EBV DNA level was routinely assessed for 940 of the 1357 patients prior to treatment. Weak positive correlations were found between the EBV DNA levels and primary tumours (Supplementary Table 1). Patients with high EBV DNA levels tended to receive CCRT rather than IMRT alone (p < 0.001; Table 1). Kaplan–Meier estimates showed that the differences in survival rates between these EBV DNA levels were significant. Patients with low and high EBV DNA levels had 5-year OS, DFS, DMFS and LRFS rates of 94.4% versus 4.3% (p < 0.001), 85.5% versus 67.1% (p < 0.001), 93.6% versus 82.2% (p < 0.001), and 94.1% versus 89.0% (p = 0.004), respectively [Supplementary Figure 1(e–h)].
Survival analysis based on the treatment regimens
In the unadjusted analysis, the following factors were all significant prognostic factors for poor OS: an older age, male sex, lower BMI, lower education, smoking, Charlson comorbidity score of 2 or greater, higher EBV DNA levels, higher tumour or node stage, and advanced clinical stage. The 5-year OS, DFS, DMFS, and LRFS rates for patients receiving IMRT alone compared with patients treated with CCRT were 91.8% versus 88.7% (HR 0.790, 95% CI 0.562–1.111, p = 0.175), 84.7% versus 77.8% (HR 0.814, 95% CI 0.630–1.051, p = 0.114), 92.6% versus 88.3% (HR 0.702, 95% CI 0.486–1.014, p = 0.059), and 94.7% versus 92.3% (HR 0.795, 95% CI 0.515–1.226, p = 0.300), respectively.
The results of the multivariate analysis using the standard Cox proportional hazards model are shown in Table 2. After adjusting for all observational factors, the survival rates were not significantly different between the CCRT and IMRT-alone groups in terms of OS (HR 1.371, 95% CI 0.946–1.988, p = 0.095), DFS (HR 1.108, 95% CI 0.832–1.475, p = 0.483), DMFS (HR 1.225, 95% CI 0.827–1.816, p = 0.312), and LRFS (HR 1.030, 95% CI 0.651–1.630, p = 0.898).
Multivariable analysis of prognostic factors for survival.
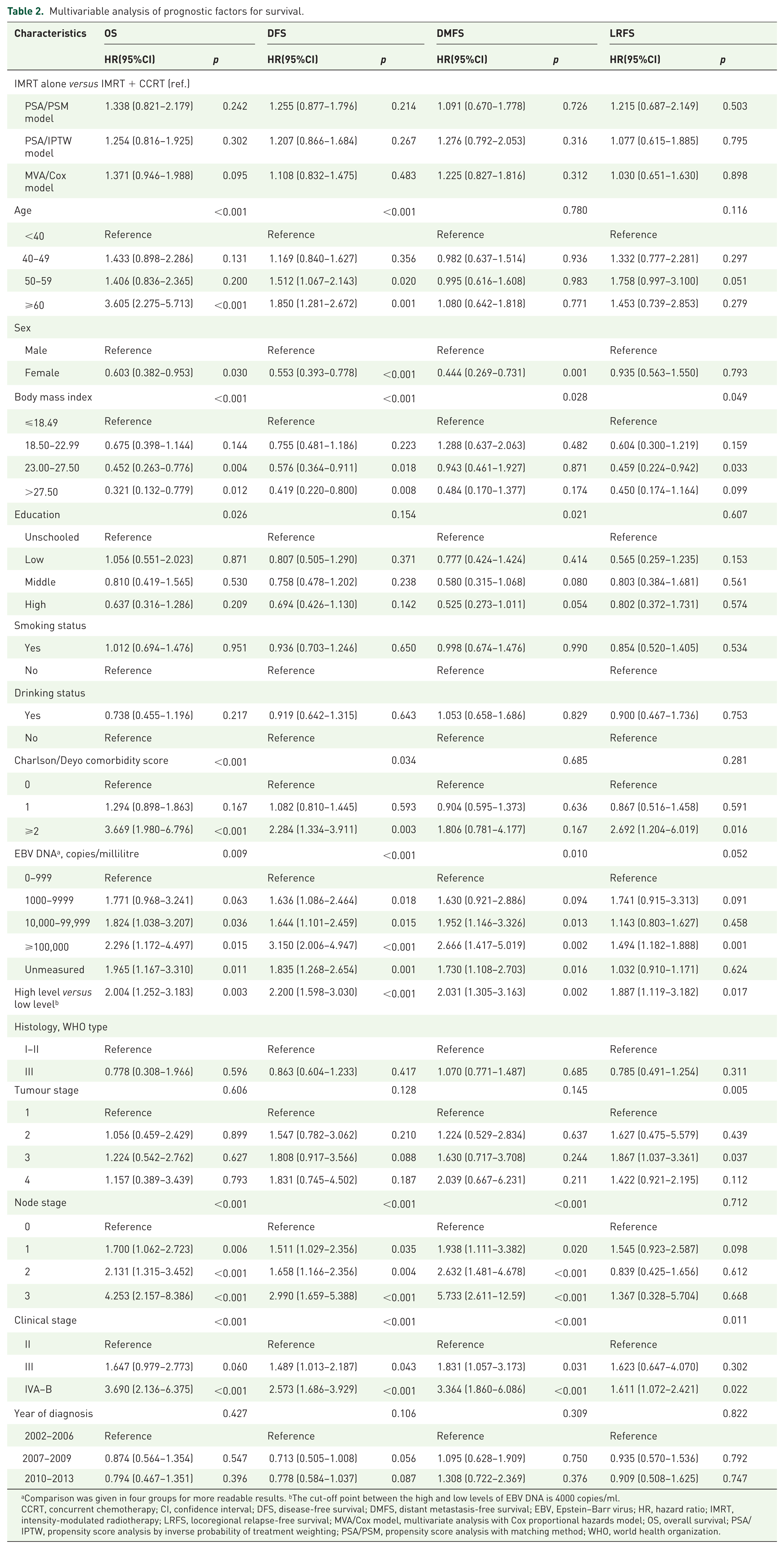
Comparison was given in four groups for more readable results. bThe cut-off point between the high and low levels of EBV DNA is 4000 copies/ml.
CCRT, concurrent chemotherapy; CI, confidence interval; DFS, disease-free survival; DMFS, distant metastasis-free survival; EBV, Epstein–Barr virus; HR, hazard ratio; IMRT, intensity-modulated radiotherapy; LRFS, locoregional relapse-free survival; MVA/Cox model, multivariate analysis with Cox proportional hazards model; OS, overall survival; PSA/IPTW, propensity score analysis by inverse probability of treatment weighting; PSA/PSM, propensity score analysis with matching method; WHO, world health organization.
PSA
Propensity score matching and weighted models with observational confounders were established to confirm and recalculate the effects of the two regimens using various algorithms to reduce confounding. For the matched analysis, 652 patients were identified. This analysis eliminated differences in all of the observed baseline characteristics in the larger cohort (Table 1) and revealed similar survival benefits for the two regimens. The PSA/IPTW model results were consistent with the multivariate analysis results obtained using the Cox proportional hazards model (Table 2).
Stratification analysis based on interaction effects
The interaction effects were examined for the EBV DNA level (categorized by a cut-off of 4000 copies per ml), N stage (categorized as N0–1 or N2–3), and clinical stage using standard Cox regression analysis of the treatment groups (Figure 2). A significant interaction was found for the EBV DNA level (p = 0.025) but not for the N stage or clinical stage (p = 0.404 and p = 0.763, respectively). The stratification analysis demonstrated the following differences between the treatment regimens: the mortality risk was more pronounced in the patients with higher EBV DNA copy numbers who received IMRT alone (Figure 3).

Forest plots for the interaction and stratification analyses based on the EBV DNA levels, clinical stages, and node stages for OS, DFS, DMFS, and LRFS.

Kaplan–Meier survival curves for OS, DFS, DMFS, and LRFS for treatment regimens in NPC patients with high EBV DNA levels (A, B, C, and D, respectively) and low EBV DNA levels (E, F, G, and H, respectively). A cut-off of 4000 copies per millilitre was selected.
Based on the strong significant interaction effect for DMFS between the treatment regimens and the clinical stages (p = 0.010; Figure 2), a stratification analysis of the treatment regimens was utilized to analyse the clinical stage (categorized as clinical stage II–III or IVA–B) with the EBV DNA level (Table 3). Compared with the CCRT group, significantly worse DMFS was found for the IMRT-alone group in stage IVA–B patients (HR 2.552, 95% CI 1.356–4.803, p = 0.004). A further stratification analysis found that stage IVA–B patients with high EBV DNA levels contributed to the difference in DMFS between the two regimens (HR 4.134, 95% CI 1.586–10.778, p = 0.004), whereas no difference was found in stage IVA–B patients with low EBV DNA levels (HR 2.340, 95% CI 0.418–13.087, p = 0.333). Additionally, no difference was found in patients with stages II–III regardless of the EBV DNA level. Similar results were obtained for OS and DFS but not for LRFS regardless of the nonsignificant interaction effects between the treatment regimens and the clinical stages (Table 3). Similar stratification results were obtained using the IPTW and PSM methods (Supplementary Table 2).
Stratification analysis between treatment regimens and EBV DNA Levels with Clinical Stage a .

There were significant interaction effects between treatment regimens and EBV DNA levels with clinical stage for distant metastasis-free survival, but not for overall, disease-free, or locoregional relapse-free survivals, and detailed interaction information was presented in Figure 3.
Due to small numbers of cases in these subgroups, CIs were extremely wide but NS.
CI, confidence interval; EBV, Epstein–Barr virus; HR, hazard ratio; NS, nonsignificant.
Sensitivity analysis
For patients with a high EBV DNA level, the advantage of CCRT was relatively robust for the survival benefit of patients with a poor performance status (Table 4). For instance, assuming an HR of 1.2, a poor performance status could not eliminate the significant survival benefit of CCRT even if we assumed that none of the patients presented with a poor performance status in the CCRT group and 100% of the patients presented with a poor performance status in the IMRT-alone group. However, assuming an HR of 2, the performance status eliminated the significant survival benefit of CCRT. The sensitivity analysis indicated that our analysis results were robust.
Sensitivity analysis for HR of all-cause mortality adjusted for poor performance status in patients with high EBV DNA level*.

NOTE: Bold font indicates situations where poor performance status was strong enough to influence significance of rules (i.e. lower bound of 95% CI crossed 1). Values based on multivariate analysis in patients with high EBV DNA level adjusted all-cause mortality HR of 2.521 (95% CI, 1.218–5.216).
CCRT, concurrent chemotherapy; CI, confidence interval; EBV, Epstein–Barr virus; IMRT, intensity-modulated radiotherapy; HR, hazard ratio; OS, overall survival.
Discussion
To the best of our knowledge, this study is the first to show that CCRT significantly improves the survival of LA-NPC patients with high plasma EBV DNA levels compared with IMRT alone based on a stratification analysis in a large endemic LA-NPC cohort. Conversely, CCRT and IMRT alone have similar benefits for patients with low plasma EBV DNA levels. This study confirms that the plasma EBV DNA level is a strong prognostic factor for NPC patients and suggests that this measure should be a significant supplement for the clinical stage and an individualized treatment marker for NPC in clinical practice. The combination of concurrent chemotherapy and RT is a recommended treatment regimen for patients with LA-NPC based on evidence from the 2DRT era. However, the benefit of CCRT for LA-NPC patients in the IMRT era may require further validation.
The Intergroup-0099 (INT-0099) trial was the first study to show that adding chemotherapy to RT increased the OS of NPC patients compared with RT alone. 3 However, considering the poor survival of the RT group and the well-differentiated nature of the carcinoma cases, initially there were doubts regarding whether these practices were applicable in endemic areas. Several subsequent studies that directly compared CCRT with RT alone confirmed the effects of this regimen.29–31 CCRT was reported to have potentially advantageous effects, including a reduction in the local tumour burden, elimination of subclinical distant metastases and synergy with RT. The Taiwan-93 trial showed that CCRT improved local control and potentially reduced the rate of distant metastasis. 29 In contrast, no significant differences in the occurrence of distant metastases were found in a study reported by Chan and colleagues 30 Additionally, three meta-analyses primarily containing studies performed in the 2DRT era consistently showed that CCRT improved OS, locoregional control and DMFS compared with RT alone.7,32,33
Notably, CCRT studies restricted to the IMRT era reported that patients receiving IMRT plus concurrent chemotherapy failed to achieve survival benefits compared with patients receiving IMRT alone,11,12,34–36 with the exception of a report by Sun and colleagues 13 However, this positive result was obtained from a small sample of patients with advanced N stages. Although this study was retrospective in design, more than 1000 cases were included, and multiple multivariate analysis methods were conducted simultaneously to confirm the robustness of the results. A key prognostic biomarker (the EBV DNA level) was adjusted in the analysis. Moreover, given that we found no interaction effects between the stage and the treatment regimen, the results from the above positive CCRT study in advanced N stage patients must be interpreted with caution. In our study, a significant interaction effect was observed between treatment regimens and differential EBV DNA levels, indicating that NPC treatment regimens should be more precisely individualized according to the EBV DNA levels in the IMRT era.
The effects of the plasma EBV DNA levels on treatment outcomes have been investigated for prognostic risk assessment, surveillance and treatment stratification.14,15,37–41 Leung and colleagues showed that plasma EBV DNA had better prognostic value when combined with the TNM staging system in the pre-IMRT era and appeared to be a more significant prognostic factor than clinical staging.17,42 Several recent studies have confirmed that the plasma EBV DNA level is a strong prognostic factor for patients with NPC when complemented with TNM staging in the IMRT era.14–16 These data also showed that the plasma EBV DNA level had a higher predictive value than clinical staging.15,16 However, the subgroup analysis results in previous studies need to be interpreted with caution due to the lack of interaction analyses. 43 Our study performed a stratification analysis based on an interaction analysis for the plasma EBV DNA level and clinical staging to objectively obtain homogeneously stratified cohorts and showed that the plasma EBV DNA level appeared to have greater prior treatment stratification value than clinical staging. Based on our study, CCRT benefited NPC patients with high pretreatment plasma EBV DNA copy numbers, whereas IMRT alone was more suitable for patients with low EBV DNA levels. The ongoing NRG-HN001 trial is designed to compare the outcomes of NPC patients who receive different individualized regimens according to their EBV DNA levels; we anticipate that the results of this trial will set an example for individualized treatment guided by EBV DNA levels.
Considering that a high distant metastasis rate is a specific feature of NPC 1 and based on the significant interaction effects on DMFS, we conducted an additional stratification analysis of DMFS to explore the effects of treatment regimens with the clinical stages and EBV DNA levels. Our results showed that clinical stage IVA–B NPC patients with high EBV DNA levels significantly benefited from CCRT with a decreased risk of distant metastasis, whereas CCRT might not benefit the DMFS of stage IVA–B patients with low EBV DNA levels and stage II–III patients.
The limitations of 2DRT, such as failure to achieve adequate coverage and poor OAR sparing, have resulted in unsatisfactory local control and survival rates.44,45 IMRT has overcome the limitations of 2DRT technology 46 and can deliver a higher dose to the tumour while minimizing the exposure of adjacent tissues or OARs, which achieves excellent locoregional control. Naturally, the margin of potential survival benefits gained from additional concurrent chemotherapy in some patient subsets may be reduced in the IMRT era. Furthermore, several studies have shown that CCRT significantly increases acute toxicity reactions and impairs treatment compliance compared with IMRT alone.7,11,12,35,36 Therefore, the benefit of CCRT in LA-NPC patients remains uncertain and further prospective investigations are needed.
We acknowledge that limitations exist in our study. First, the main limitation of our study is its retrospective and single-institute nature, although the cases were extracted from a prospectively maintained database. To minimize bias, we not only adopted different models to confirm our analysis but also performed a sensitivity analysis to estimate the effects of unmeasured confounders and validate the robustness of our results. Second, the quantitative cut-off for plasma EBV DNA levels was selected based on the results of our previous studies conducted in the same epidemic area. However, a cut-off point of more than 6000 copies per ml has also been suggested. 1 Therefore, we objectively analysed four groups using magnitudes of 10 and two groups with conventional cut-off levels in the endemic area. Third, we observed no interaction between the stage and regimens. However, a significant difference in OS was found between regimens in MVA in patients with clinical stage IV, possibly due to an insufficient number of cases. Thus, we concede that this result should be interpreted with caution. Fourth, although we regarded plasma EBV DNA as an extremely significant complement to the clinical staging system, use of this measure in combination with other important biomarkers (i.e. circulating fibrinogen 20 ) could help provide more precise treatment choices. Lastly, EBV DNA has been shown to be an important factor for prediction of the prognosis of NPC patients. However, approximately 30% of patients lacked an EBV DNA measurement in this study due to its retrospective nature. Therefore, a prospective study is necessary to validate our findings.
In conclusion, this study is the first to combine an interaction effect analysis and stratification by plasma EBV DNA levels and show that CCRT can significantly improve the survival rates of NPC patients with high plasma EBV DNA levels compared with IMRT alone; however, CCRT does not significantly benefit patients with low plasma EBV DNA levels. CCRT may benefit DMFS for clinical stage IVA–B NPC patients with high EBV DNA levels but not those with low EBV DNA levels and clinical stage II–III NPC patients regardless of their EBV DNA levels. A well-designed prospective study with a large cohort is required to confirm the role of concurrent chemotherapy in the IMRT era and to explore individualized regimens for various LA-NPC patient subgroups with different plasma EBV DNA levels.
Supplemental Material
T-Supplementary_Material – Supplemental material for The plasma Epstein–Barr virus DNA level guides precision treatment for nasopharyngeal carcinoma in the intensity-modulated radiotherapy era: a large population-based cohort study from an endemic area
Supplemental material, T-Supplementary_Material for The plasma Epstein–Barr virus DNA level guides precision treatment for nasopharyngeal carcinoma in the intensity-modulated radiotherapy era: a large population-based cohort study from an endemic area by Hu Liang, Xing Lv, Lin Wang, Yi-Shan Wu, Rui Sun, Yan-Fang Ye, Liang-Ru Ke, Qin Yang, Ya-Hui Yu, Wen-Ze Qiu, Guo-Ying Liu, Xin-Jun Huang, Wang-Zhong Li, Shu-Hui Lv, Xiang Guo, Yan-Qun Xiang and Wei-Xiong Xia in Therapeutic Advances in Medical Oncology
Footnotes
Acknowledgements
Hu Liang, Xing Lv, and Lin Wang contributed equally to this work. The authors greatly thank Professor Qing Liu and Can-hong Wen, PhD, for statistical assistance during the preparation of this manuscript. The authenticity of this article has been validated by uploading the key raw data onto the Research Data Deposit (RDD) public platform (![]() ) with the approval RDD number as RDDA2018000422.
) with the approval RDD number as RDDA2018000422.
Funding
The authors disclosed receipt of the following financial support for the research, authorship, and/or publication of this article: This study was funded by the National Natural Science Foundation of China (grant numbers 81472525, 81572665, and 81672680).
Conflict of interest statement
The authors declare that there is no conflict of interest.
References
Supplementary Material
Please find the following supplemental material available below.
For Open Access articles published under a Creative Commons License, all supplemental material carries the same license as the article it is associated with.
For non-Open Access articles published, all supplemental material carries a non-exclusive license, and permission requests for re-use of supplemental material or any part of supplemental material shall be sent directly to the copyright owner as specified in the copyright notice associated with the article.