
Abstract
Introduction:
Congenital anomalies of the kidney and urinary tract (CAKUT) represent a wide range of disorders that result from developmental abnormalities of the kidneys, urinary collecting tract, and lower urinary tract. There has been extensive development in approaches to the management of stones in normal kidneys with the advent of retrograde intra-renal surgeries (RIRS)/ureteroscopies, extracorporeal shock wave lithotripsy (ESWL) percutaneous nephrolithotomy (PCNL), and minimally invasive surgery (laparoscopy/robotics). However, the management of stones in CAKUT is not straightforward and is often challenging for urologists. There are no clear guidelines available to help navigate stone management in such patients.
Materials and methods:
The aim of this literature review was to focus on stone management in anomalous kidneys. Most common abnormalities were considered. The studies were very heterogeneous with different approaches. The methodology involved evaluating studies looking into individual surgical approaches to the management of stones in these anomalous kidneys as well as looking at different approaches to stone management, in particular renal abnormality.
Results:
We found RIRS is a feasible approach in most stones with sizes <20 mm and PCNL holds the upper hand in stones more than 20 mm. However, ESWL, laparoscopy, and robotics have their places in managing some of these cases.
Conclusion:
We concluded that stones in anomalous kidneys can be challenging but can be managed safely. There is no straightforward answer to the right technique but rather the right planning based on the anatomy of the kidney in terms of vascularity and drainage, stone size and density, and expertise available.
Keywords
Introduction
The management of stones in the urinary tract has evolved rapidly over the last century with surgical techniques becoming more minimally invasive in the shape of ureteroscopies, extracorporeal shock wave lithotripsy, lasers, and laparoscopy. Less than 4% of patients with urinary stones are estimated to undergo open surgery in reference centers. 1 However, managing stones in kidneys with anomalies still poses a challenge even to experienced urologists.
Congenital abnormalities affecting the kidneys or other structures of the urinary tract are referred to as congenital anomalies of the kidney and urinary tract (CAKUT). The abnormalities are broadly classified as abnormalities in structure, renal vasculature, number, position, and renal fusion. In this review, kidneys with abnormalities in terms of position and fusion will be considered. In terms of position, abnormalities include non-rotation, mal-rotation, and ectopia (under-ascent or over-ascent). Renal fusion anomalies include horseshoe kidneys and crossed renal fused ectopic kidneys. It is noteworthy that these kidneys often have a higher stone formation rate as compared to normal kidneys due to aberrant renal anatomy, altered drainage (renal pelvis in abnormal location, ureter being inserted in high position), and recurrent infections. 2 Stones in anomalous kidneys do not differ from normal kidney stones and calcium oxalate is present as a major constituent of these. 3
The approaches to managing these kidney stones are not straightforward and often can be confusing as there are no specific algorithms and often the surgeon needs to manage each case individually.4,5 In this review, the main aim was to perform a narrative review of stone management in common types of anomalous kidneys.
Materials and methods
Evidence acquisition
Inclusion criteria included – stone management in anomalous kidneys including
Horseshoe kidneys (HSK),
Crossed fused renal ectopia (CFRA),
Mal-rotated kidneys (MRK), and
Pelvic kidneys (PK).
Exclusion criteria included the following:
Stone management in other CAKUT anomalies other than the above four.
Studies with less than 20 patients, and
Studies with patients aged less than 18.
Search strategy
We followed the Preferred Reporting Items for Systematic Reviews and Meta-analyses (PRISMA). National Library of Medicine (PubMed/Medline), Elsevier, and Google Scholar databases were electronically searched with the terms ‘Anomalous Kidneys’, ‘Stones’, ‘Horseshoe kidneys, ‘Malrotated kidneys, ‘pelvic ectopic kidneys’, ‘crossed ectopic kidneys’, ‘crossed fused renal ectopia’, ‘Percutaneous Nephrolithotomy’, ‘Ureteroscopy’, ‘Extracorporeal shockwave lithotripsy’, ‘Laparoscopy’. Boolean operators were used including and/or.
Study selection
We used Rayyan software (a free web tool designed to help researchers speed up the process of screening and selecting studies) to aid in the process of duplicate removal, and initial screening, and facilitate author collaboration. After deleting duplicates, following the inclusion and exclusion criterion, studies were shortlisted. Full-text papers of the shortlisted studies were reviewed by the SQ3R (Survey, Question, read, recite, review) technique.
Data extraction
The data extraction was carried out in two parts: surgical procedures and stone management in anomalous kidneys and different approaches to stones in a particular abnormality.
Results
Study selection results
In the initial search, 327 studies were identified. After removing duplicates and unrelated studies, a total of 186 studies were shortlisted. Finally, 51 studies were screened, 28 were excluded, and 23 were assessed for eligibility. After applying the exclusion criterion, 11 studies were included in the review. The PRISMA flow chart is provided in Figure 1.
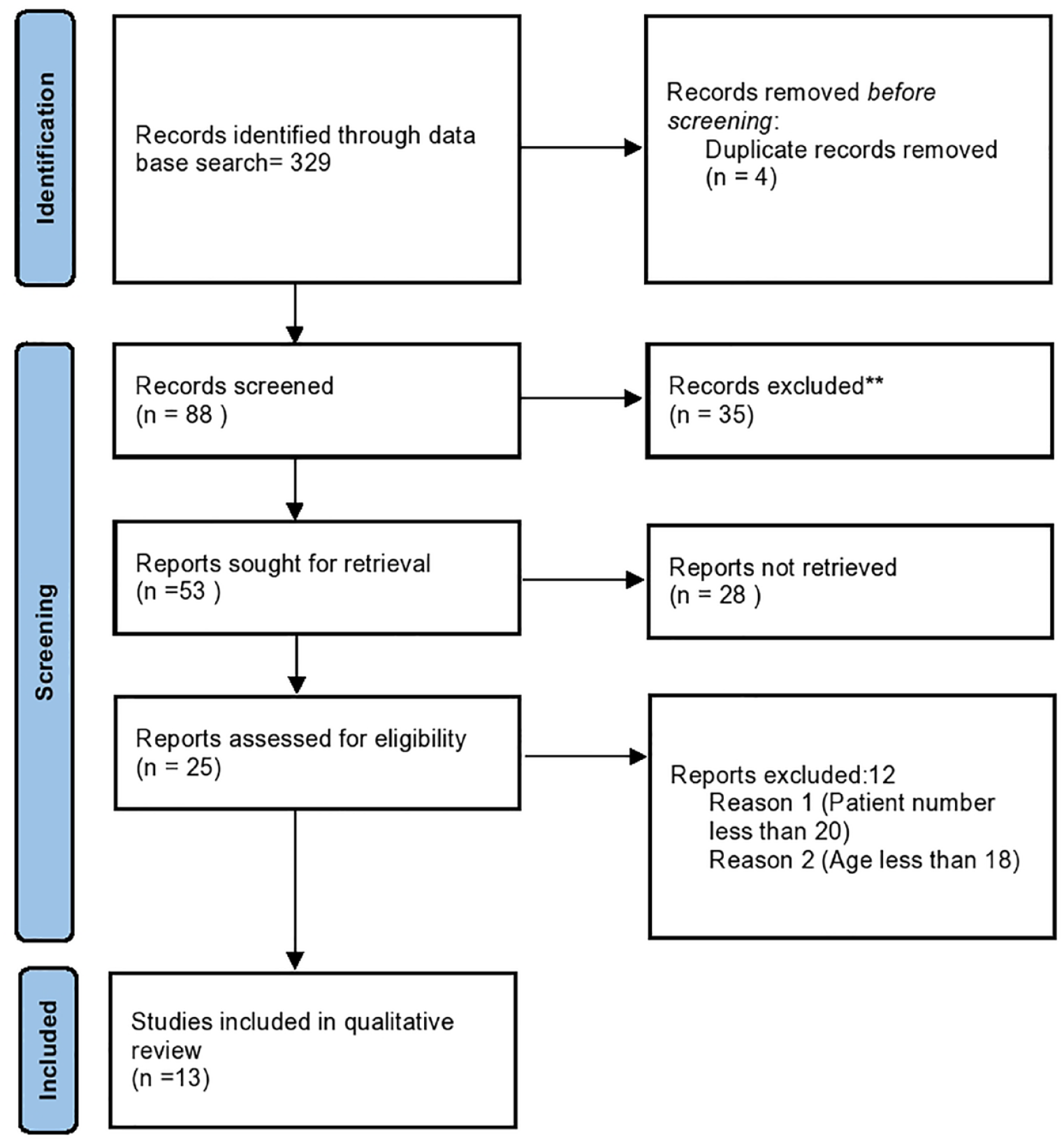
PRISMA flowchart.
Study characteristics
Studies were grouped based on the study’s aim, methodology used, and total number of studies. The summary is given in Table 1.
Study characteristics.
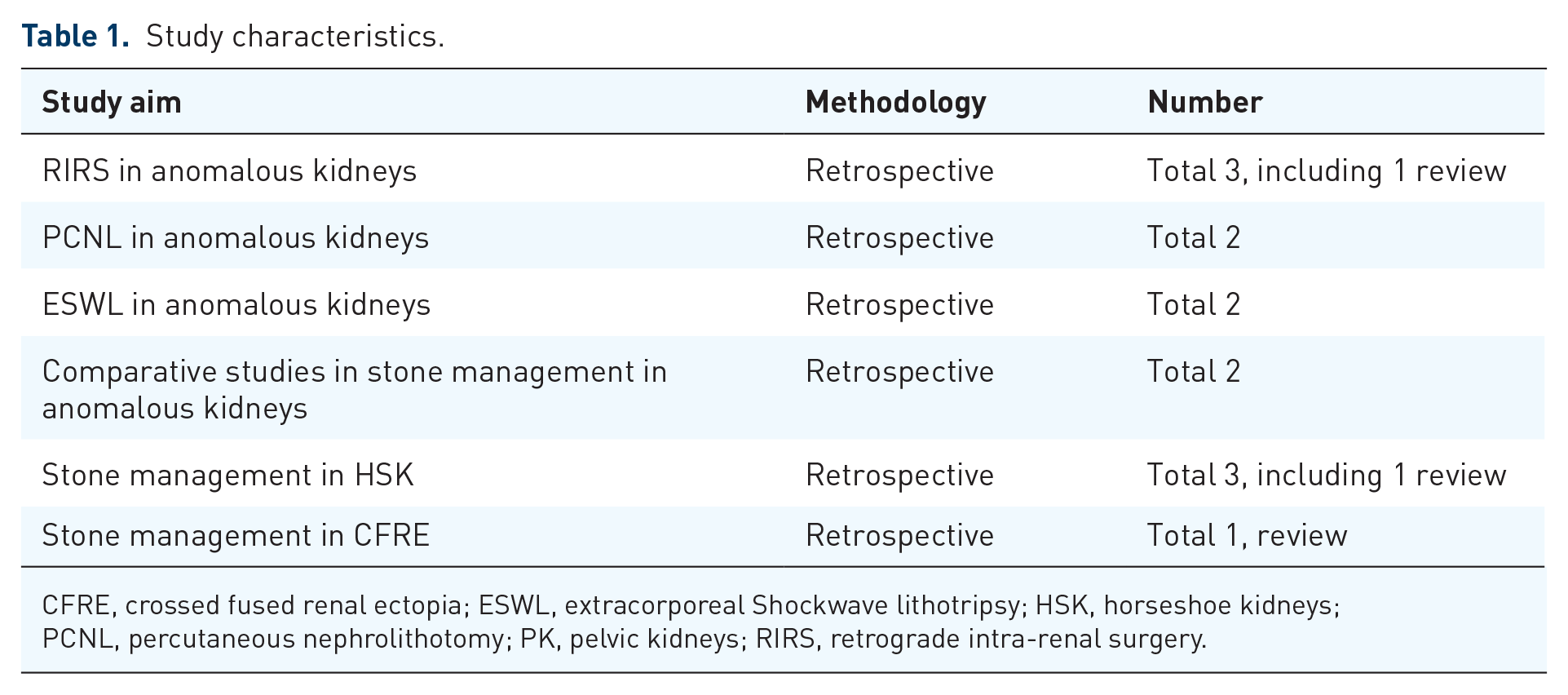
CFRE, crossed fused renal ectopia; ESWL, extracorporeal Shockwave lithotripsy; HSK, horseshoe kidneys; PCNL, percutaneous nephrolithotomy; PK, pelvic kidneys; RIRS, retrograde intra-renal surgery.
Surgical approaches to stone management in anomalous kidneys
RIRS in anomalous kidney stone management
A recent study of 414 patients has found that retrograde intra-renal surgery (RIRS) in patients with anomalous kidneys is a safe and effective treatment with an acceptable complication rate in experienced hands. 6 A review including 14 studies, with 413 patients has found that RIRS was able to achieve an initial stone-free rate (SFR) in the range of 76.6% (n = 322) and a final SFR in the range of 82.3% (n = 340), associated with the low risk of major complications (only 2.4% were Clavien–Dindo ⩾ III). 7 In another study, including 25 patients, the results were similar with good SFR and minimal complications. 8 Table 2 summarizes these results.
RIRS/ureteroscopy in anomalous kidney stone management.
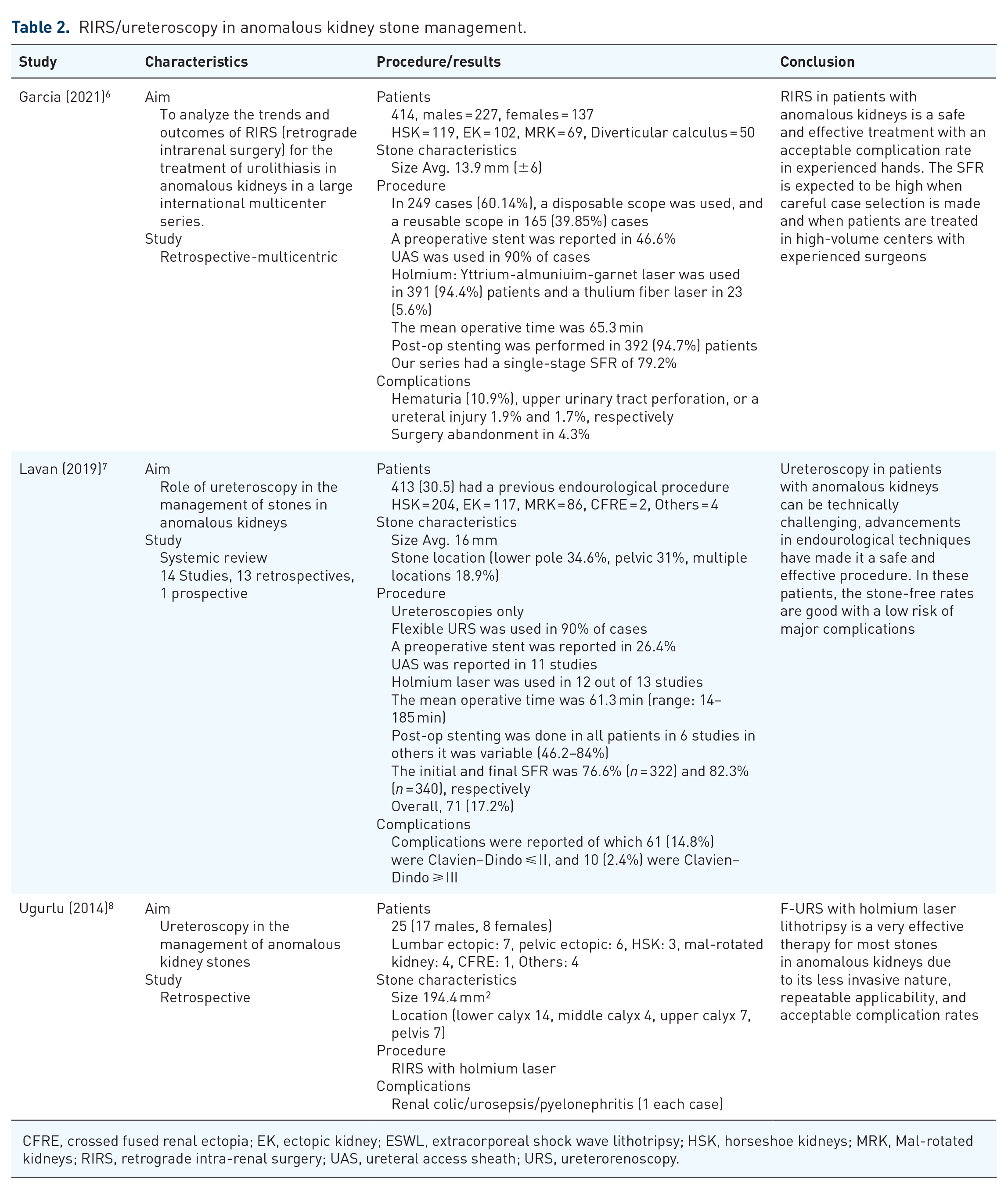
CFRE, crossed fused renal ectopia; EK, ectopic kidney; ESWL, extracorporeal shock wave lithotripsy; HSK, horseshoe kidneys; MRK, Mal-rotated kidneys; RIRS, retrograde intra-renal surgery; UAS, ureteral access sheath; URS, ureterorenoscopy.
PCNL in anomalous kidney stone management
Percutaneous nephrolithotomy (PCNL) is often used in surgical procedures in patients with anomalous kidneys; however, it often requires careful preoperative planning and may even need close collaboration with other branches like radiology. Although the complication rate may be more than RIRS and in PKs, laparoscopic-assisted PCNL may be indicated, PCNL is the choice of treatment in stones with sizes >2 cm.9,10 Summarized results are shown in Table 3.
PCNL in anomalous kidney stone management.
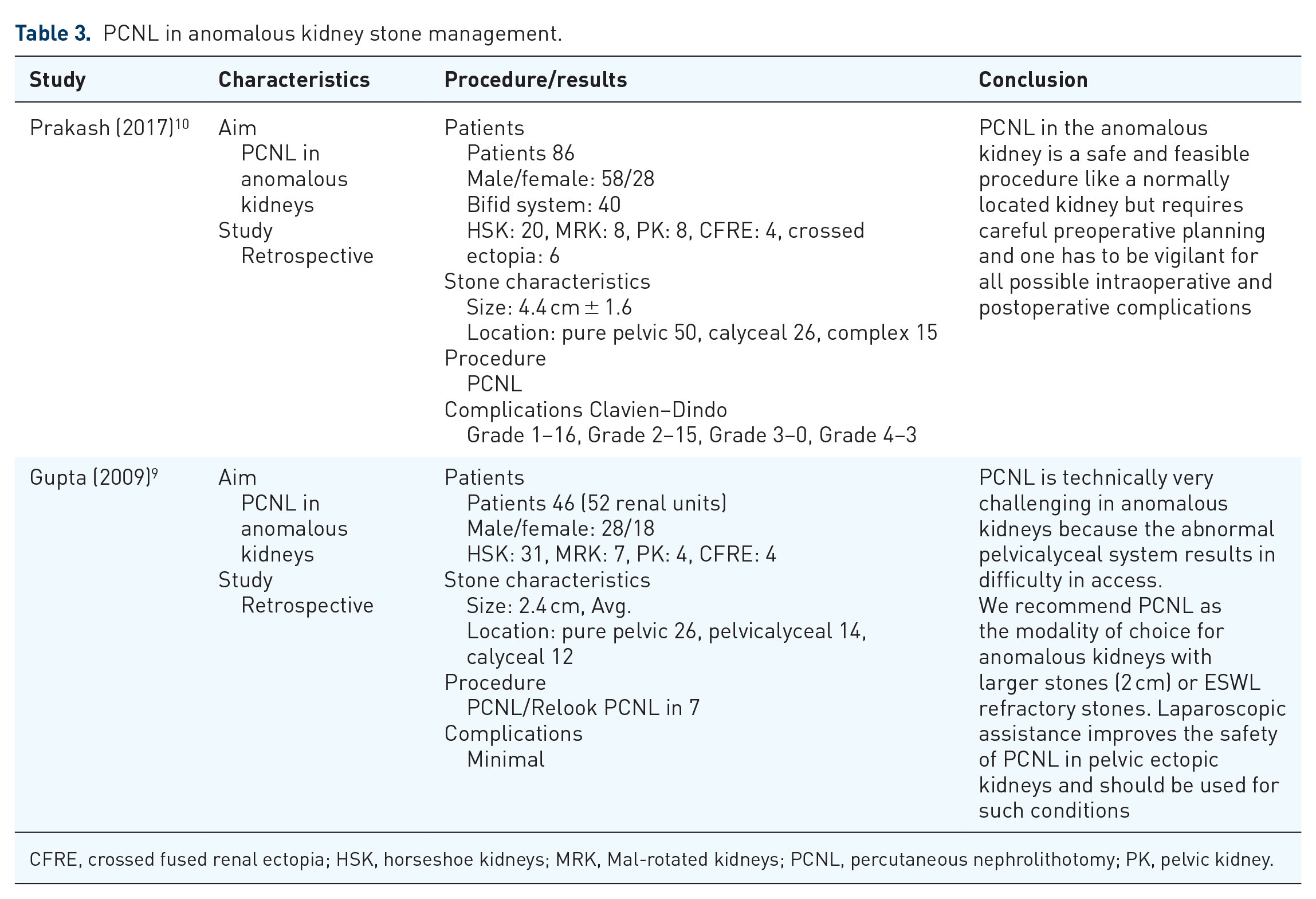
CFRE, crossed fused renal ectopia; HSK, horseshoe kidneys; MRK, Mal-rotated kidneys; PCNL, percutaneous nephrolithotomy; PK, pelvic kidney.
ESWL in anomalous kidney stone management
Extracorporeal shockwave lithotripsy (ESWL) is still one of the modalities being used in patients with stones in anomalous kidneys. Studies have revealed that it can be used effectively in stones with <20 mm but the number of sessions may range somewhat between 1 and 6.11,12 Renal colic was reported to be the most common complication in these two studies. In addition to stone size, stone burden, and location, drainage along with the degree of the anomaly has been found to impact treatment success with ESWL.11,12 Summarized results are given in Table 4.
ESWL in anomalous kidney stone management.
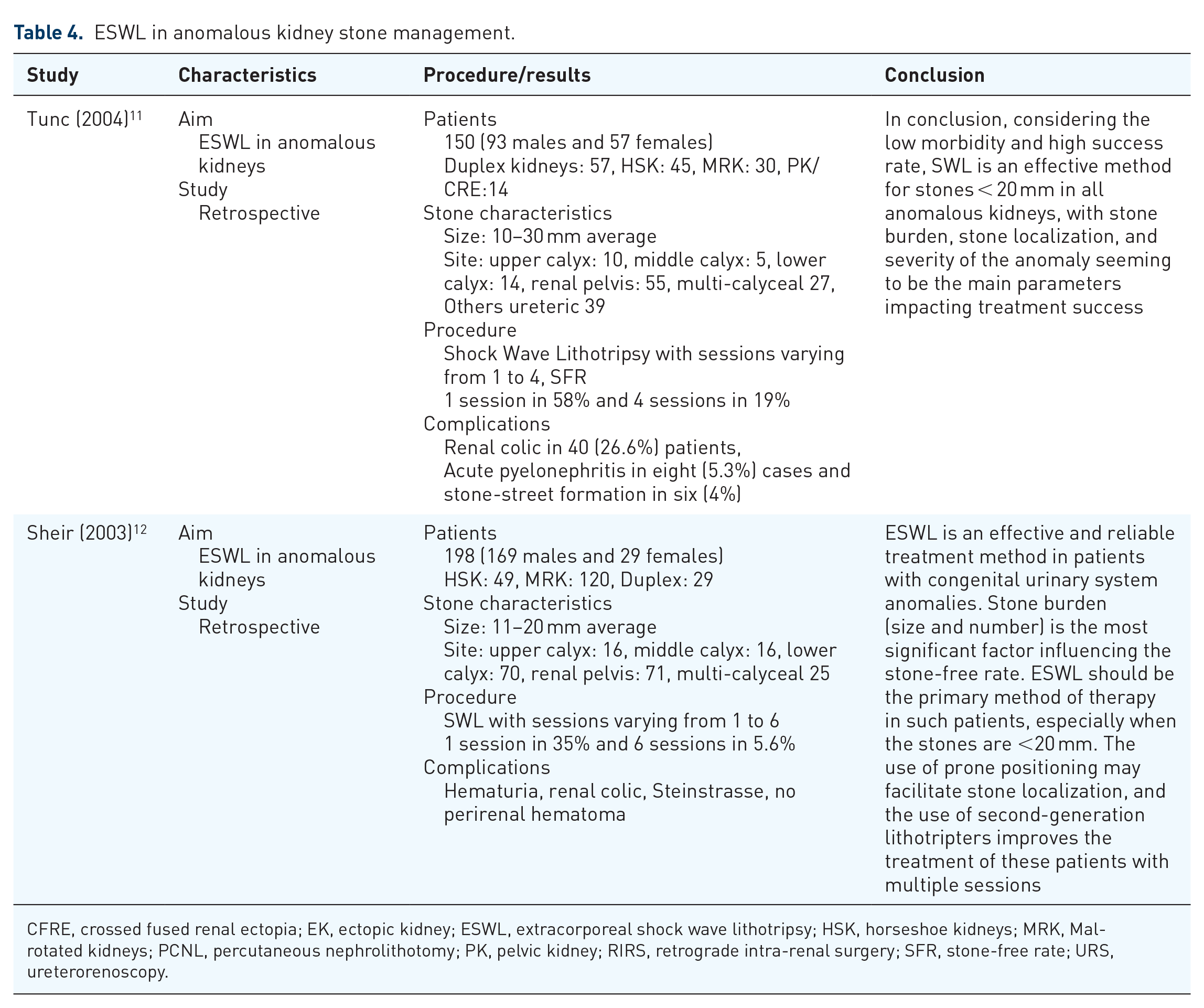
CFRE, crossed fused renal ectopia; EK, ectopic kidney; ESWL, extracorporeal shock wave lithotripsy; HSK, horseshoe kidneys; MRK, Mal-rotated kidneys; PCNL, percutaneous nephrolithotomy; PK, pelvic kidney; RIRS, retrograde intra-renal surgery; SFR, stone-free rate; URS, ureterorenoscopy.
Comparison of different techniques in anomalous kidney stone management
A recent study comparing different techniques has revealed that RIRS, PCNL, and laparoscopy are effective ways of managing stones in anomalous kidneys but RIRS is safe and satisfactory with small- and medium-sized calculi. 4 However, a more recent study comparing different techniques has found that stone size (</>1.5 cm), stone density (</>1000 HU) [and kidney anatomy (regarding drainage) are essential in determining the management of stones in these kidneys]. 2 In the same study, they provided an algorithm for the management of these kidney stones (Figure 2). A multi-centric study in 2022 has concluded that both PCNL and RIRS are safe and feasible options in any anomaly, but PCNL provides better SFR, especially in HSK and ectopic kidneys and those with higher stone volumes. 13 Summarized results are given in Table 5.
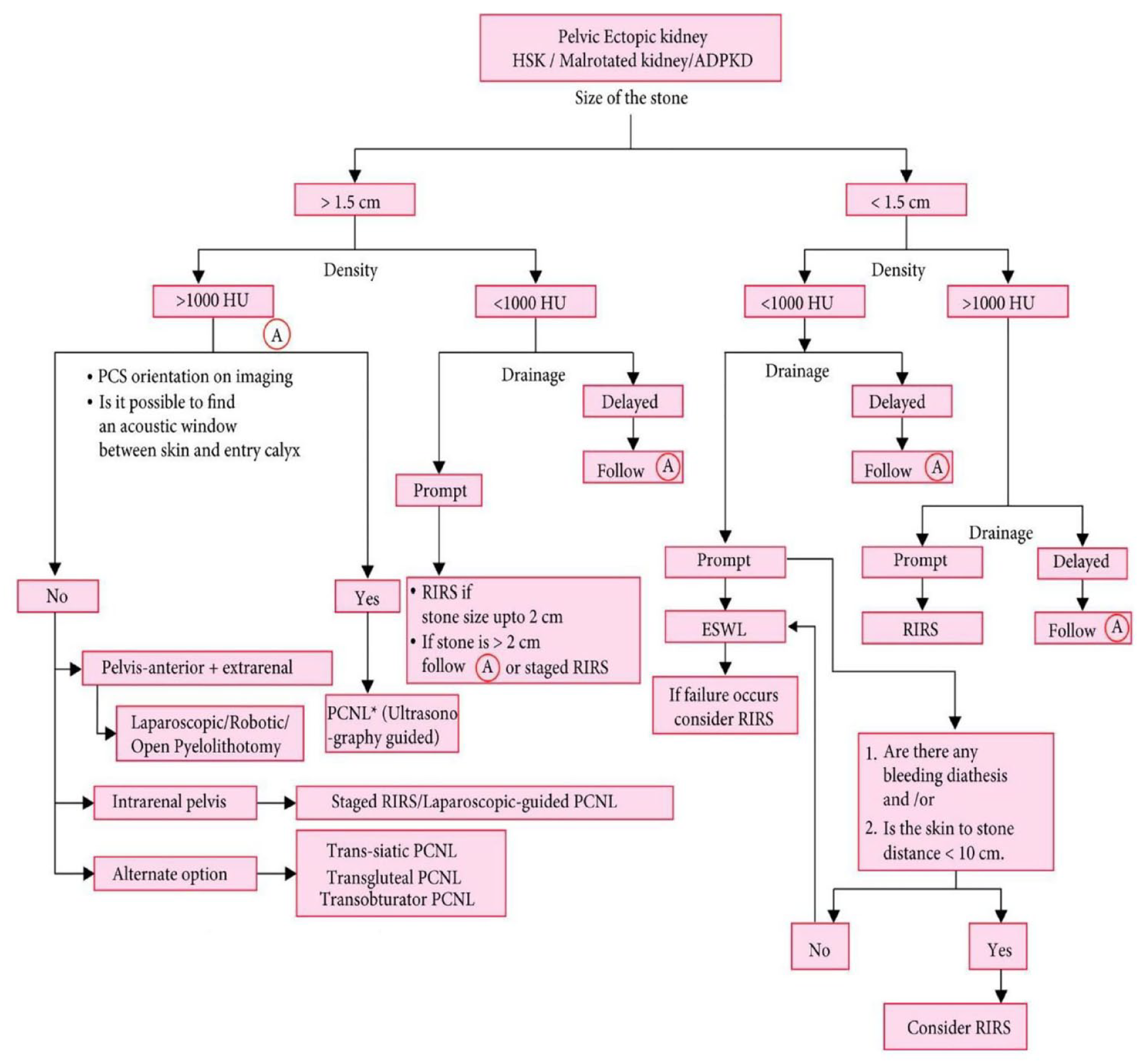
Algorithm for an approach to stones in anomalous kidneys.
Comparative of surgical approaches for the management of stones in anomalous kidneys.
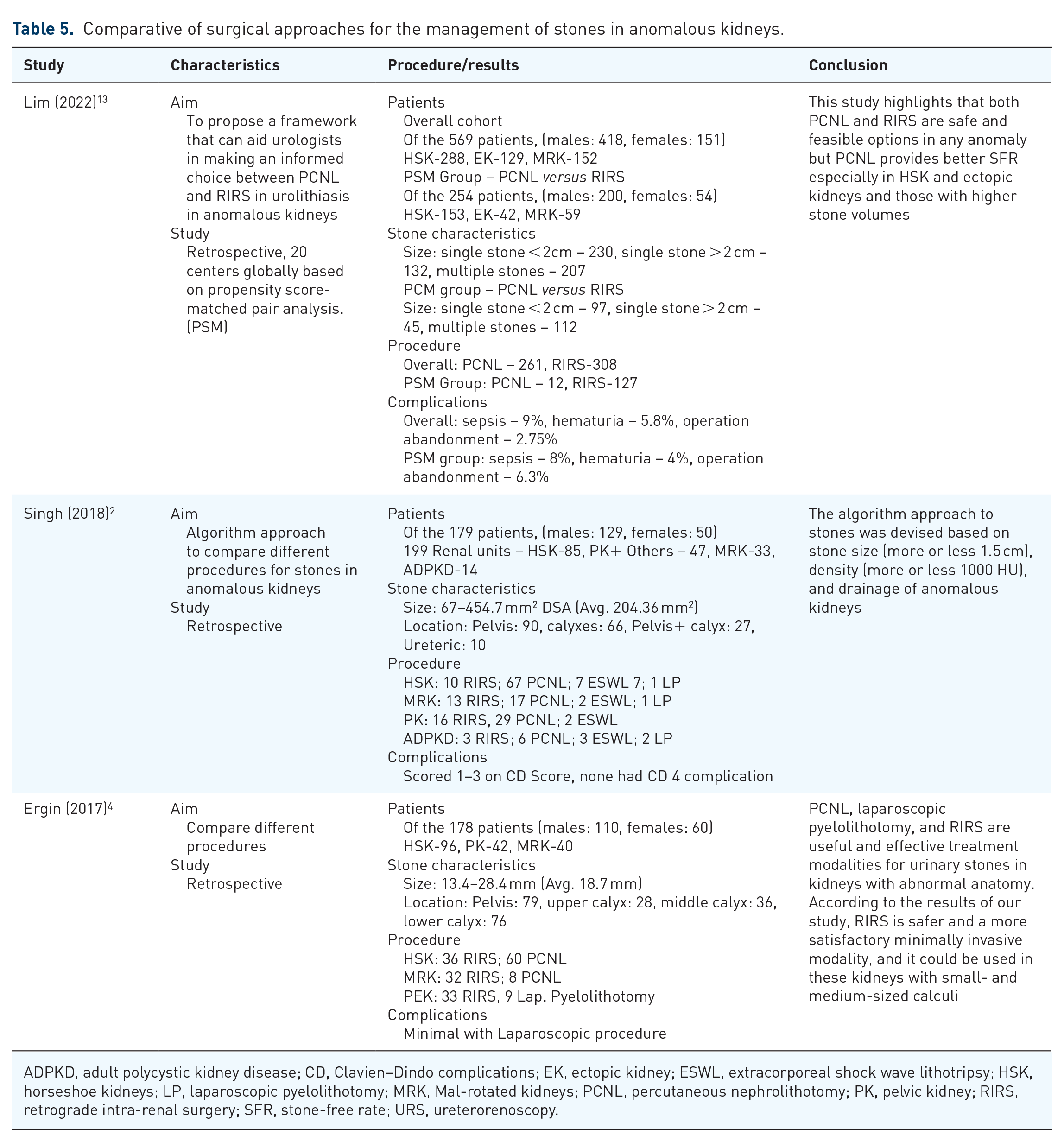
ADPKD, adult polycystic kidney disease; CD, Clavien–Dindo complications; EK, ectopic kidney; ESWL, extracorporeal shock wave lithotripsy; HSK, horseshoe kidneys; LP, laparoscopic pyelolithotomy; MRK, Mal-rotated kidneys; PCNL, percutaneous nephrolithotomy; PK, pelvic kidney; RIRS, retrograde intra-renal surgery; SFR, stone-free rate; URS, ureterorenoscopy.
Stone management in horseshoe kidneys
Two recent studies have compared different techniques for the management of stones in HSK patients. One study compared RIRS with ESWL for stones in HSK management. This study established that RIRS is a feasible and sufficient option for stone management in HSK patients with sizes less than 2 cm. 14 In another study, RIRS was compared to PCNL in HSK patients with stones, they concluded that RIRS had almost similar stone clearance as that of PCNL with minimal complications. 15 Summarized results are given in Table 6.
Stone management in HSK.
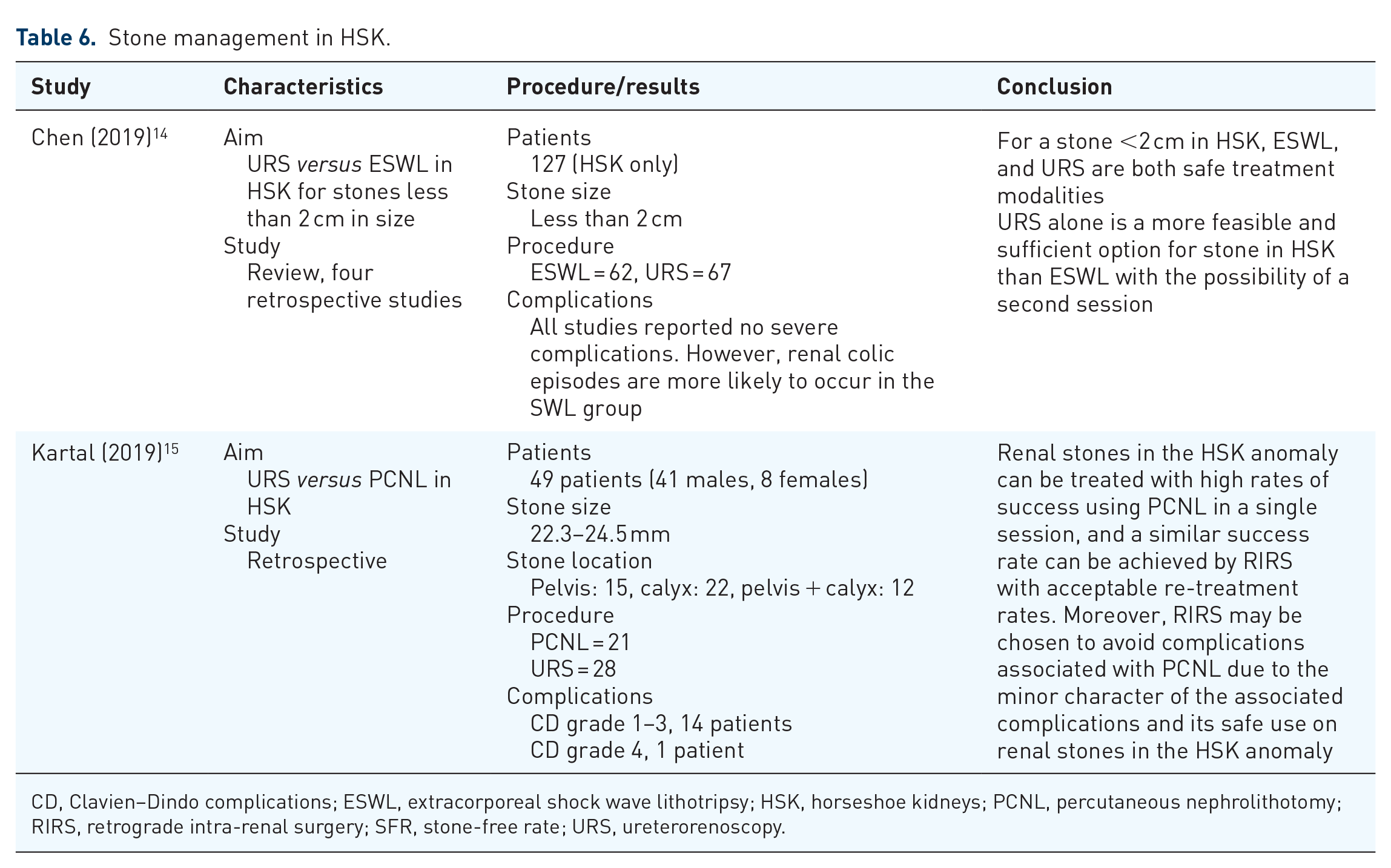
CD, Clavien–Dindo complications; ESWL, extracorporeal shock wave lithotripsy; HSK, horseshoe kidneys; PCNL, percutaneous nephrolithotomy; RIRS, retrograde intra-renal surgery; SFR, stone-free rate; URS, ureterorenoscopy.
Stone management in crossed-fused renal ectopia
A single study, reviewing 35 CFRE cases with stones reported in the literature, has found that all methods have been used for management including open surgery as well. 16 Summarized results are given in Table 7.
Stone management in CFRE.
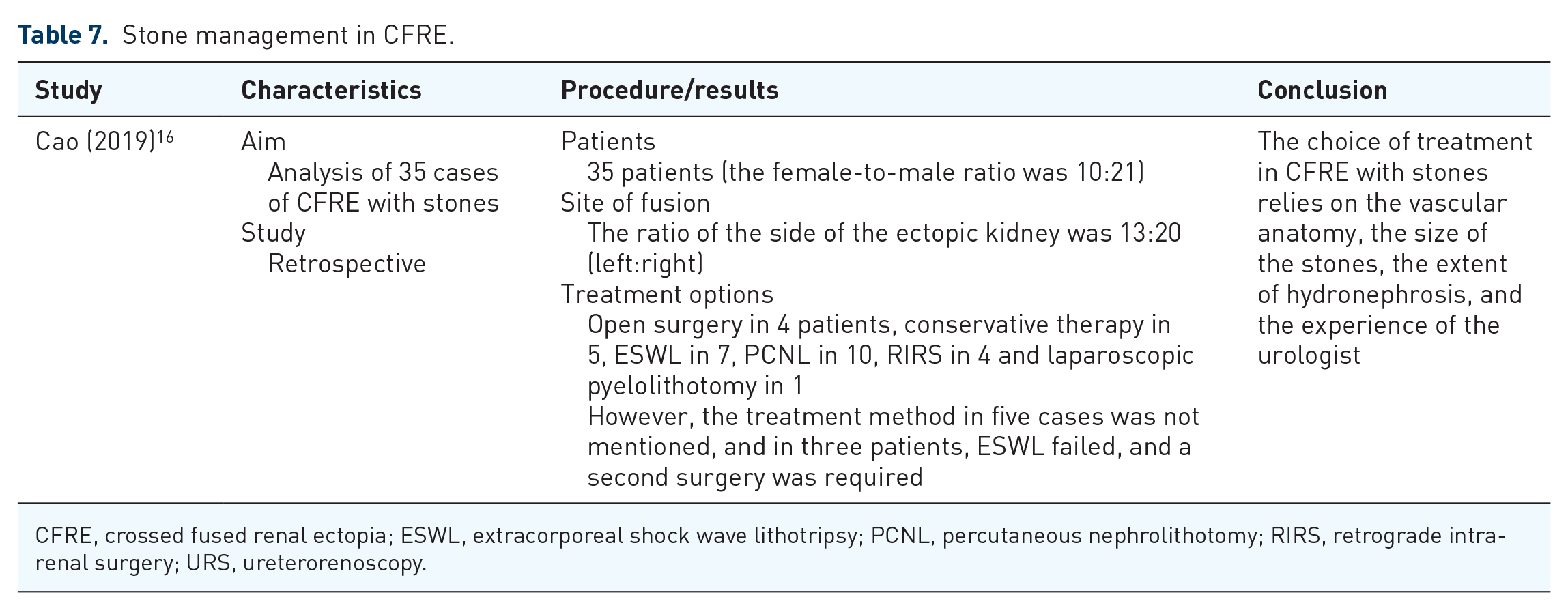
CFRE, crossed fused renal ectopia; ESWL, extracorporeal shock wave lithotripsy; PCNL, percutaneous nephrolithotomy; RIRS, retrograde intra-renal surgery; URS, ureterorenoscopy.
Discussion
Congenital malformations of the urogenital system at birth account for about 10%. 17 Approximately 50% of these involve upper urinary tract abnormalities. 18 Of the various upper urinary tract anomalies, abnormalities of the kidney are predominant accounting for 20–30% of all detectable anomalies. 19 The prevalence of stones in anomalous kidneys is significantly higher compared to the general population. 5 However, the mechanism or mechanisms leading to the increased prevalence of stones in anomalous kidneys are not fully elucidated. However, urinary stasis appears to be the most common factor leading to increased stone formation in these anomalies. 20 Surgical intervention remains the most effective therapeutic intervention in managing symptomatic kidney stones. In the past, options were limited to open nephrolithotomy; however, it has since been superseded by minimally invasive methods such as PCNL, ESWL, and ureteroscopy/ureterorenoscopy (URS) However, at present still there is no clear superiority of one method over the other in treating stones in individuals with CAKUT. Often the treatment has to be innovative and individualized for the given patient. Although CAKUT includes a spectrum of abnormalities including the kidney’s number, ascent, form and fusion, ascent, rotational anomalies, renal vasculature, and the renal collecting system. 21 However, this review focused on those anomalies which are commonly encountered clinically.
HSK is present in 1 in 400–1600 births and is the most common renal fusion abnormality. 22 The incidence of stones in adult patients with HSK is as high as 36%.23,24 CFRE malformation of the kidney is estimated in autopsies in the range of 1 in 1000–2000 and about ~0.01% of live births. 25 From studies, only 35 patients with crossed renal ectopia having stones have been reported. 16 MK occurs in about 1 in 939 autopsies. It is further classified into non-rotation, incomplete rotation, reverse rotation, transverse rotation, or excessive rotation. 26 PK incidence is in the range of 1 in 5000 patients. Most of these patients remain asymptomatic, and clinical recognition is seen in the range of 1–10,000. 26
Although a multitude of studies are available dealing with the same topic, due to the heterogeneity of clinical presentation and non-availability of randomized controlled trials in anomalous kidneys, there is a lack of a consensus on an approach to stone management in such kidneys. 13
We found more and more cases can be managed with RIRS with minimal morbidity particularly if the size of stones is <20 mm. The advances in endourological instrumentation include smaller diameter disposable flexible ureteroscopes and advances in lasers, RIRS is considered an attractive option in challenging stone cases associated with anomalous kidneys. 13 PCNL still has a vital role in stones with sizes more than 20 mm. A recent multi-centric study concluded that both PCNL and RIRS are safe and feasible options in any anomaly, but PCNL provides better SFR, especially in HSK and ectopic kidneys and those with higher stone volumes. 13
It was also obvious that ESWL is not being employed for such stones with much enthusiasm. The reason was not clear, but it appears it is because of the overall decreased usage of ESWL in the management of kidney stones rather than his subset of patients. We found the algorithmic approach recommended in one of the comparative studies very useful for approaching these stones (Figure 2).
This literary review reveals that the approach to stones in anomalous kidneys is not straightforward and depends on multiple factors – anatomy of the kidney, stone location, stone size, stone density, and expertise available (both urological as well as radiological). As such, each case needs to be approached individually and planned carefully.
This review has many limitations. The studies/reviews involved are based mostly on retrospective data. The clinical entities as well as the procedures employed and differences in approaches are also variable and difficult to standardize. Also, some of the data used for some rare conditions is very old due to the rarity of anomalies.
Conclusion
We conclude that stones in anomalous kidneys can be challenging but can be managed safely. There is no straightforward answer to the right technique but rather the right planning based on the anatomy of the kidney in terms of vascularity and drainage, stone size and density, and expertise available. We found RIRS is a feasible approach in the majority of stones with sizes <20 mm and PCNL holds the upper hand in stones >20 mm. However, ESWL, laparoscopy, and robotics do have their places in the management of some of these cases.
Supplemental Material
sj-docx-1-tau-10.1177_17562872231217797 – Supplemental material for Challenges and options for management of stones in anomalous kidneys: a review of current literature
Supplemental material, sj-docx-1-tau-10.1177_17562872231217797 for Challenges and options for management of stones in anomalous kidneys: a review of current literature by Mudassir Wani, Ahmed Haider Abdalla Mohamed, Gareth Brown, Seshadri Sriprasad and Sanjeev Madaan in Therapeutic Advances in Urology
Footnotes
References
Supplementary Material
Please find the following supplemental material available below.
For Open Access articles published under a Creative Commons License, all supplemental material carries the same license as the article it is associated with.
For non-Open Access articles published, all supplemental material carries a non-exclusive license, and permission requests for re-use of supplemental material or any part of supplemental material shall be sent directly to the copyright owner as specified in the copyright notice associated with the article.