
Abstract
Whether pancreatic extracorporeal shock wave lithotripsy (ESWL) is safe for patients with autosomal dominant polycystic kidney disease (ADPKD) is unclear. A woman in her early 30s was admitted to our hospital because of intermittent upper abdominal pain and recurrent pancreatitis. The imaging results confirmed the diagnosis of pancreatic stones and ADPKD. We performed pancreatic ESWL using a third-generation lithotripter to pulverize the pancreatic stones. A maximum of 5000 shock waves was delivered per therapeutic session. A second session of ESWL was performed the next day. The patient developed no adverse events or complications related to pancreatic ESWL. Three years after treatment, the patient had developed no relapse of pancreatitis or abdominal pain. Shock waves do not lead to complications such as hematuria, cyst rupture, or deterioration of the inner bleeding of renal cysts. Multiple kidney cysts are not a contraindication for pancreatic ESWL.
Keywords
Introduction
More than 50% of patients with chronic pancreatitis (CP) develop pancreatic stones. 1 Extracorporeal shock wave lithotripsy (ESWL) has been recommended for the management of large pancreatic stones.2 –4 Autosomal dominant polycystic kidney disease (ADPKD) is a chronic, progressive disease characterized by the development and growth of cysts in the kidneys and other organs with resultant systemic manifestations. 5 Although pancreatic ESWL is reportedly safe for patients with concurrent pancreatic stones and pancreatic pseudocysts, 3 whether pancreatic ESWL is safe for patients with ADPKD remains uncertain because these patients have more cysts in their bilateral kidneys. We herein describe a patient with ADPKD who developed concurrent CP and pancreatic stones. Pancreatic ESWL was performed to relieve the obstruction of the pancreatic duct, and no related adverse events or complications occurred.
Case report
The reporting of this study conforms to the CARE guidelines.
6
Details regarding the identity of the patient were de-identified. A woman in her early 30s was admitted to our hospital because of intermittent upper abdominal pain and recurrent pancreatitis. She had a history of ADPKD. Her renal function was normal, but she had experienced an episode of hematuria and received a blood transfusion before admission to our hospital. Magnetic resonance cholangiopancreatography showed old hemorrhage within the renal cysts and dilation of the main pancreatic duct with multiple filling defects (

Magnetic resonance cholangiopancreatography showed old hemorrhage within the cysts and a dilated main pancreatic duct with multiple filling defects.
According to the mechanism of ESWL, shock waves are transmitted through liquid and human tissues with the same acoustic impedance. Therefore, a cyst filled with fluid would consume little energy from shock waves. Theoretically, therefore, ESWL should be safe in a patient such as ours.
After a discussion among our multidisciplinary team, we decided to perform pancreatic ESWL on this patient. The patient was fully informed about the procedure, and she provided written informed consent for treatment. We performed pancreatic ESWL starting from the pancreatic head and progressing to the tail with a third-generation lithotripter (Compact Delta II; Dornier Med Tech, Wessling, Germany) to pulverize the stones. A maximum of 5000 shock waves was delivered per therapeutic session. Another session of ESWL was performed the next day. Endoscopic retrograde pancreatography was performed to extract the stone fragments, and a pancreatic stent was placed to improve the drainage of the pancreatic duct. The patient developed no adverse events or complications related to pancreatic ESWL. At the 6-month follow-up, a computed tomography scan showed that the pancreatic stent was still in situ and that complete clearance of stones from the main pancreatic duct had been achieved (
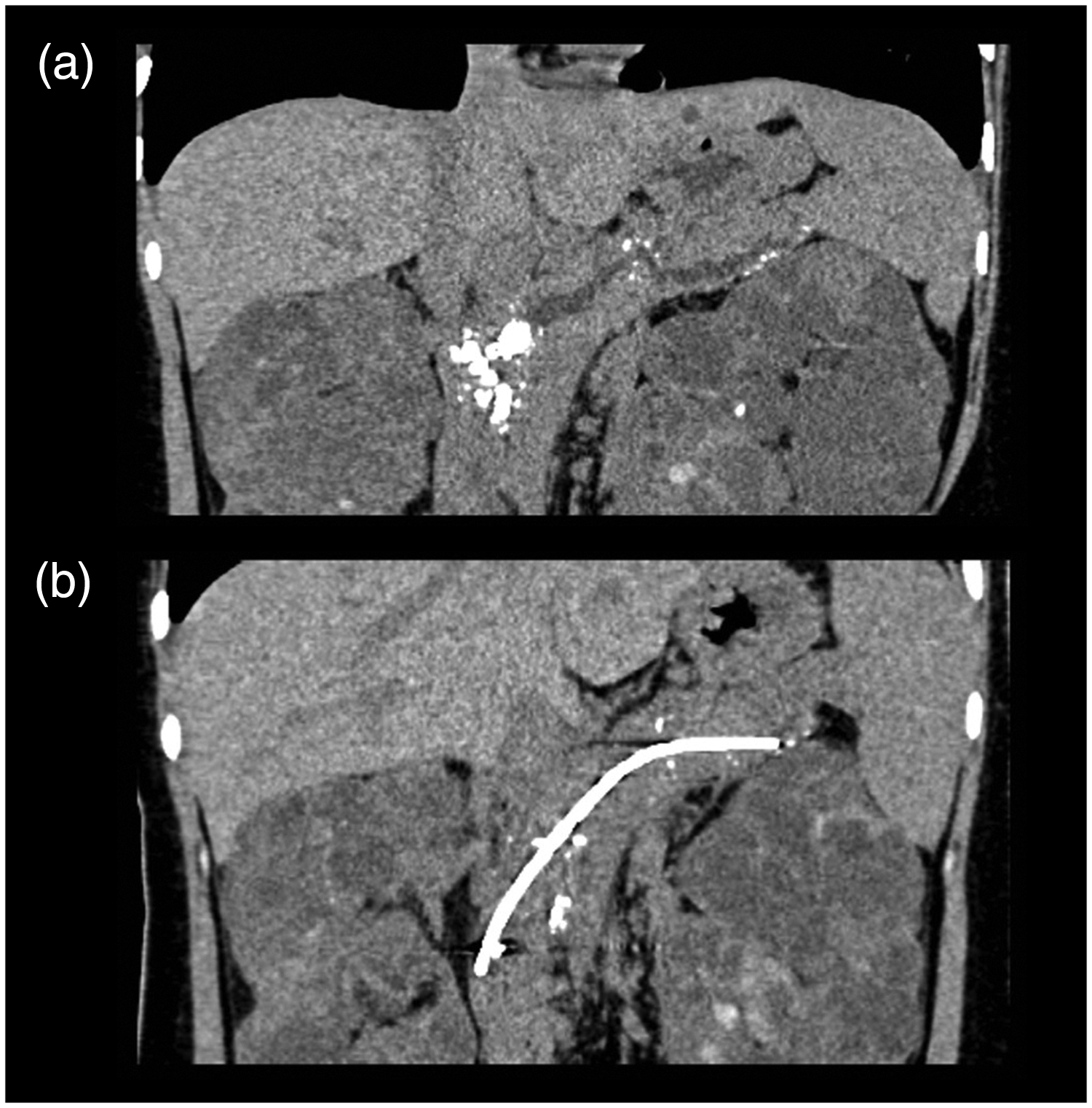
Curved planar reconstruction from a computed tomography scan of the pancreas before and after ESWL (extracorporeal shock wave lithotripsy). (a) Before ESWL, multiple stones were present in the significantly dilated main pancreatic duct. (b) Six months after ESWL, complete clearance of the stones from the main pancreatic duct had been achieved and the inserted stent was in situ.
Discussion
ADPKD is the most common inherited kidney disease, affecting 1/400 to 1/1000 people in the general population. 8 One retrospective study showed that 36% of patients with ADPKD had pancreatic lesions, which were primarily cysts. 9 Most pancreatic cysts in these patients are asymptomatic. 10 To date, only a few sporadic cases of concomitant pancreatitis and ADPKD have been described in the literature. When the pancreatic cyst is very large and compresses the main pancreatic duct, chronic obstructive pancreatitis may occur. 11 In the present case, pancreatic cysts were not diagnosed. Therefore, CP was not a gastrointestinal manifestation of ADPKD in our patient but instead a concurrent disease. One report described a pediatric patient with genetically determined CP and ADPKD. 12
ESWL has been the mainstay in the management of pancreatic stones with a success rate of up to 90%. 13 However, for patients with multiple cysts in the bilateral kidneys, the risk of complications and the stone clearance rate of pancreatic ESWL are uncertain. Concerns include the risk of traumatic hemorrhage into the cysts, shock wave-induced damage to nephrons, and decreased stone clearance. To our knowledge, no report has described the application of ESWL for pulverization of pancreatic stones in patients with ADPKD. While there are few studies of ESWL for treatment of renal stones in patients with ADPKD, the intensity of shock waves used in pancreatic ESWL is usually much higher than that used for nephrolithiasis. 13 Kim et al. 14 described a patient with ADPKD who presented with acute cyst rupture, hemorrhage, and septic shock after ESWL. Only one case series has described the use of ESWL for nephrolithiasis in patients with ADPKD. In the 13 patients of that series, a stone-free rate of 85% was achieved at 3 months, with 2 patients requiring repeated treatments during this time, and no complications were reported. 15 In our previous research, major complications of pancreatic ESWL included post-ESWL pancreatitis, bleeding, infection, steinstrasse, and perforation. In addition to these complications, transient adverse events (TAEs), specifically referring to mild adverse events, were proposed. TAEs were defined as transient injuries caused by shock waves that required no medical intervention and did not prolong hospitalization. TAEs included skin erythema, mild tenderness of the region in contact with the shock wave head, asymptomatic hyperamylasemia, hematuria, and acute gastrointestinal mucosal injury (manifesting as hematemesis and melena). 16 Hematuria is caused by delivery of the refracted shock wave energy to the kidney during pancreatic ESWL, resulting in mild renal injury. The occurrence rate of hematuria was 4.2%. Because kidneys with ADPKD are more fragile than healthy kidneys, it is clinically meaningful to determine whether pancreatic ESWL is safe in patients with ADPKD.
Theoretically, pancreatic ESWL should be safe in patients with ADPKD because shock waves are transmitted through liquid and human tissues with the same acoustic impedance, and cysts consume a low amount of energy. We performed pancreatic ESWL on 59 patients with pancreatic pseudocysts among 849 patients with pancreatic stones, and no significant increase in adverse events was observed. 3
This is the first report to show that pancreatic EWSL is a safe and effective therapeutic strategy in patients with concurrent pancreatic stones and ADPKD. Multiple kidney cysts are not a contraindication for pancreatic ESWL.
Ethics
The study protocol was approved by the Ethics Committee of Changhai Hospital.
Declaration of competing interests
The authors declare that they have no competing interests.
Availability of data and materials
Data sharing is not applicable to this article because no datasets were generated or analyzed during the current study.
Footnotes
Funding
The authors disclosed receipt of the following financial support for the research, authorship, and/or publication of this article: This study was supported by Shanghai Science and Technology Innovation Action Plan [Grant No. 19DZ2201900 (LHH)], Shanghai Shuguang Program [Grant No. 20SG36], Shanghai Chenguang Program [Grant No. 20CG42], and Shanghai Sailing Program [Grant No. 19YF1446800 (DW)].
Authors’ contributions
DW, JX, and YWB collected and analyzed the patient’s data and wrote the manuscript. CLM, ZSL, and LHH contributed to the conception of the article. All authors read and approved the final manuscript.