
Abstract
Background:
The lower calyx is the most common site for kidney stones. While minimally invasive, flexible ureteroscopic lithotripsy often yields suboptimal stone-free rates (SFR) for lower calyx stones due to anatomical constraints and limited endoscope deflection.
Objectives:
To evaluate the efficacy and safety of a novel technique that combines Sotn ureteroscopy (Sotn-URS) with flexible ureteroscopy (fURS), involving stone displacement before lithotripsy, for managing lower calyx stones ⩽20 mm.
Design:
A retrospective comparative study complemented by in vitro simulation experiments.
Methods:
An in vitro model assessed the impact of a 200 µm laser fiber, a 365 µm fiber, a 1.7 Fr stone retrieval basket, and a flexible ureteral sheath on the deflection of a single-use fURS. In all, 240 patients with lower calyx stones (⩽20 mm) were allocated to either the experimental group (n = 114) or the control group (n = 126). The experimental group underwent combined Sotn-URS and fURS with basket-assisted stone displacement to the kidney pelvis or upper ureter before laser lithotripsy. The control group underwent conventional in situ lithotripsy using fURS alone. Outcomes, including operative time, SFR (immediate and at 4 weeks), surgeon comfort (Borg scale), first-pass sheath placement success, and complications, were compared.
Results:
The maximum deflection angle of the fURS alone was 295.7°. Insertion of a 365 µm fiber significantly reduced this angle to 270.1°, while a 200 µm fiber or basket had minimal impact (293.3° and 293.4°, respectively). Compared with control group, the experimental group demonstrated significantly higher immediate SFR (85.1% vs 73.0%, p < 0.05) and 4-week SFR (91.2% vs 81.7%, p < 0.05), along with shorter total operative time (51.7 vs 70.4 min, p < 0.05) and fURS intrarenal time (22.2 vs 52.2 min, p < 0.05). Surgeon comfort was better (Borg score 0.63 vs 2.9, p < 0.05), and the rate of ureteral mucosal injury was lower (3.5% vs 11.1%, p < 0.05).
Conclusion:
The stone displacement technique utilizing combined Sotn-URS and fURS is an efficient and safe surgical approach for lower calyx stones ⩽20 mm. It uses the stable access and efficient lithotripsy of rigid Sotn-URS and the flexibility of fURS for stone displacement, resulting in improved stone clearance rates, reduced operative time, and lower ureteral injury risk.
Keywords
Introduction
Kidney stones pose a substantial burden on public health and healthcare systems, as they are a significant cause of both chronic kidney disease and end-stage kidney disease. 1 Their incidence is increasing, affecting 10.1%–19.1% of the population. 2 Anatomically, the lower calyx is the most common site for stone formation and retention, accounting for approximately 35% of cases. 3 This predisposition results from gravitational sedimentation and the potential migration of stones from other parts of the collecting system.
The management of lower calyx stones is particularly challenging. While the European Urological Association recommends multiple options, including extracorporeal shockwave lithotripsy (ESWL), flexible ureteroscopic lithotripsy (FURL), and percutaneous nephrolithotomy (PCNL), 4 each has significant limitations for this location. ESWL, despite being non-invasive, is associated with low stone-free rates (SFR) and high retreatment rates, making it a non-first-line therapy per the American Urological Association guidelines. 5 PCNL achieves high stone clearance rates but has greater invasiveness and complication risks. 6 By contrast, flexible ureteroscopy (fURS) has demonstrated favorable SFR and safety and has become the preferred method for treating lower calyx stones of 20 mm or less, according to the European Urological Association guidelines. 4
Before FURL, a ureteral access sheath (UAS) is typically placed to facilitate repeated access and irrigation. Despite this established approach, a significant disparity in outcomes exists based on stone location. Many studies have shown that the SFR for stones in the upper and middle calyxes and the kidney pelvis can reach 94.4%, while the SFR for lower calyx stones is only 60.4%.7,8 This discrepancy is primarily attributed to the unique anatomical challenge posed by the lower calyx, specifically the infundibulopelvic angle (IPA). The IPA, defined as the angle between the axis of the lower calyx and the upper ureter, is often acute. 9 This anatomical constraint directly conflicts with the mechanical limitations of the fURS. The maximum deflection of the fURS is limited, and this available deflection is further compromised during lithotripsy by the physical rigidity of the laser fiber within the working channel. 10 Consequently, when navigating a narrow IPA, the fURS frequently cannot achieve the deflection necessary to reach the dependent portion of the lower calyx. This results in suboptimal visualization and laser targeting, often leaving parts of the stone inaccessible or only partially fragmented. 11 Furthermore, operating at maximum deflection increases energy loss along the laser fiber and elevates the risk of fiber fracture, impairing lithotripsy efficiency and potentially damaging the scope.12,13 Residual fragments in the lower calyx are poorly cleared, increasing the risks of growth, recurrence, and infection. Therefore, strategies to circumvent these anatomical and technical limitations are critically needed.
The Sotn ureteroscopy (Sotn-URS) is a novel lithotripsy system based on ureteroscopic principles. It comprises a detachable, negative-pressure ureteroscope used in combination with a modified rigid UAS, a configuration commonly used for treating ureteral stones. 14 By combining lithotripsy and suction functions, the Sotn-URS enables larger stone fragments to be evacuated during fragmentation via the modified UAS. This reduces both the number of residual fragments and the overall stone retention rate. Notably, a flexible ureteroscope can also be introduced through this modified UAS to manage kidney stones and residual fragments, thereby potentially improving the SFR. 15
In the present study, we used a combination of Sotn-URS and a single-use fURS to treat lower calyx stones measuring ⩽20 mm. Stones were displaced to the ureteropelvic junction or upper ureter using the fURS equipped with a stone retrieval basket. Subsequently, laser lithotripsy was performed using the lithotripsy scope of the Sotn-URS. The clinical efficacy of this combined approach was then compared with that of conventional fURS alone. In addition, by analyzing the deflection performance of fURS in in vitro models, we aimed to optimize the instrument combination and establish a basis for the clinical application of this technique.
Materials and methods
General information
Ethics statement
This study was conducted in accordance with the Declaration of Helsinki and was approved by the Ethics Committee of the Joint Logistics Support Force 910th Hospital (approval number: YL-2023-36). Written informed consent was obtained from all participants or their legal guardians.
Reporting guidelines: This study was reported in accordance with the Strengthening the Reporting of Observational Studies in Epidemiology (STROBE) guidelines for observational studies. 16 The completed STROBE checklist is provided as Supplemental Material.
Study participants
This retrospective comparative study analyzed 240 cases of lower calyx stones treated at the Joint Logistics Support Force 910th Hospital and Fuzhou First General Hospital Affiliated with Fujian Medical University between March 2021 and March 2025. Patients were allocated to either an experimental group or a control group based on different surgical methods. The experimental group underwent a combined procedure using Sotn-URS and fURS, while the control group underwent conventional fURS using a flexible vacuum-assisted ureteric access sheath (FV-UAS). The selection of surgical approach was primarily guided by preoperative CT assessment of key anatomical factors, including the IPA and lower calyx neck length. Cases with anatomical features suggesting potential difficulty for in situ lithotripsy were preferentially assigned to the experimental group. For cases with favorable anatomy, either technique was considered appropriate, with the final decision made by the treating team based on comprehensive clinical evaluation.
The sample size was determined based on the postoperative SFR as the primary outcome. Using historical data indicating an SFR of approximately 60.4% for conventional fURS and anticipating an improvement to 85% with the combined technique, a power analysis was conducted using PASS software (version 15.0.1, Kaysville, UT, USA). Under a two-sided α of 0.05 and 80% power, a minimum of 51 evaluable patients per group was required. Accounting for approximately 20% attrition, we aimed to enroll at least 64 patients per group. The final cohort sizes (experimental, n = 114; control, n = 126) substantially exceeded this minimum, ensuring sufficient statistical power for the analysis.
Inclusion criteria
Patients diagnosed with lower calyx stones (⩽20 mm) through imaging examinations.
Unilateral or bilateral stones, with surgical intervention performed on a single side only.
Patients had a clear clinical indication for ureteroscopic stone management.
Exclusion criteria
Multiple kidney stones.
Congenital anatomical abnormalities of the kidneys.
Ureteral strictures or other pathology precluding safe placement of a ureteroscope or UAS.
Active, uncontrolled urinary tract or systemic infection/inflammation.
Coagulation disorders.
Severe cardiopulmonary insufficiency or other major systemic disease that contraindicates surgery.
Methods
Main surgical instruments and materials
Sotn-URS (Sotn, China; Figure 1(a)–(g)): This system consists of a standard diagnostic ureteroscope (length: 45 cm; diameter: 7.5–11.3 Fr), a dedicated lithotripsy scope (length: 46 cm; diameter: 4–6 Fr), a modified rigid UAS (length: 40 cm; diameter: 11.5–12.5 Fr; non-deflectable), and an integrated irrigation/suction unit.

Components of the Sotn-URS system. (a) The modified rigid UAS. (b) The standard diagnostic ureteroscope. (c) The lithotripsy (“gravel”) scope. (d) The integrated negative-pressure control valve. (e) The standard ureteroscope is assembled within the UAS. (f) The lithotripsy scope is assembled with the UAS and negative-pressure valve. (g) The complete Sotn-URS system is connected to the external irrigation and suction apparatus.
Single-use fURS (Fr 8.0 mm, Ruipai, China).
Stone retrieval basket (Fr 1.7 mm, three-wire design, Huamei, China, Figure 2).

Dimensions of the stone retrieval basket. (a) The length of the deployed basket head. (b) The diameter of the opened basket head.
FV-UAS (Fr 12/14 mm, Huamei, China).
Zebra guide wire and double-J ureteral stent (Laike, Germany).
Ureteroscope (Wolf, Germany).
Laser system: Holmium laser lithotripter (100 W, Dazhu, China) with 200 and 365 µm laser fibers (Dazu, China).
In vitro experiment method
The deflectable segment of the fURS was identified as the distal 7 cm. When the deflectable segment of the fURS was not fully extended beyond the ureteral sheath, its maximum achievable deflection was mechanically constrained. In an in vitro simulation, we applied maximum torque to deflect the ureteroscope. The maximum achievable deflection angles were measured and photographed with the fURS extended at varying lengths (0, 1, 3, 5, and 7 cm) from the distal end of the FV-UAS, as well as at 7 cm extension from the modified rigid UAS (Figure 3). The ureteroscope’s working channel was inserted with a stone retrieval basket, a 200 µm laser fiber, and a 365 µm laser fiber. All images were analyzed using ImageJ software (version 2024.6, Bethesda, MD, USA). Using the apex of the deflection curve as a reference point, the maximum deflection angle under each condition was measured (Figure 4).
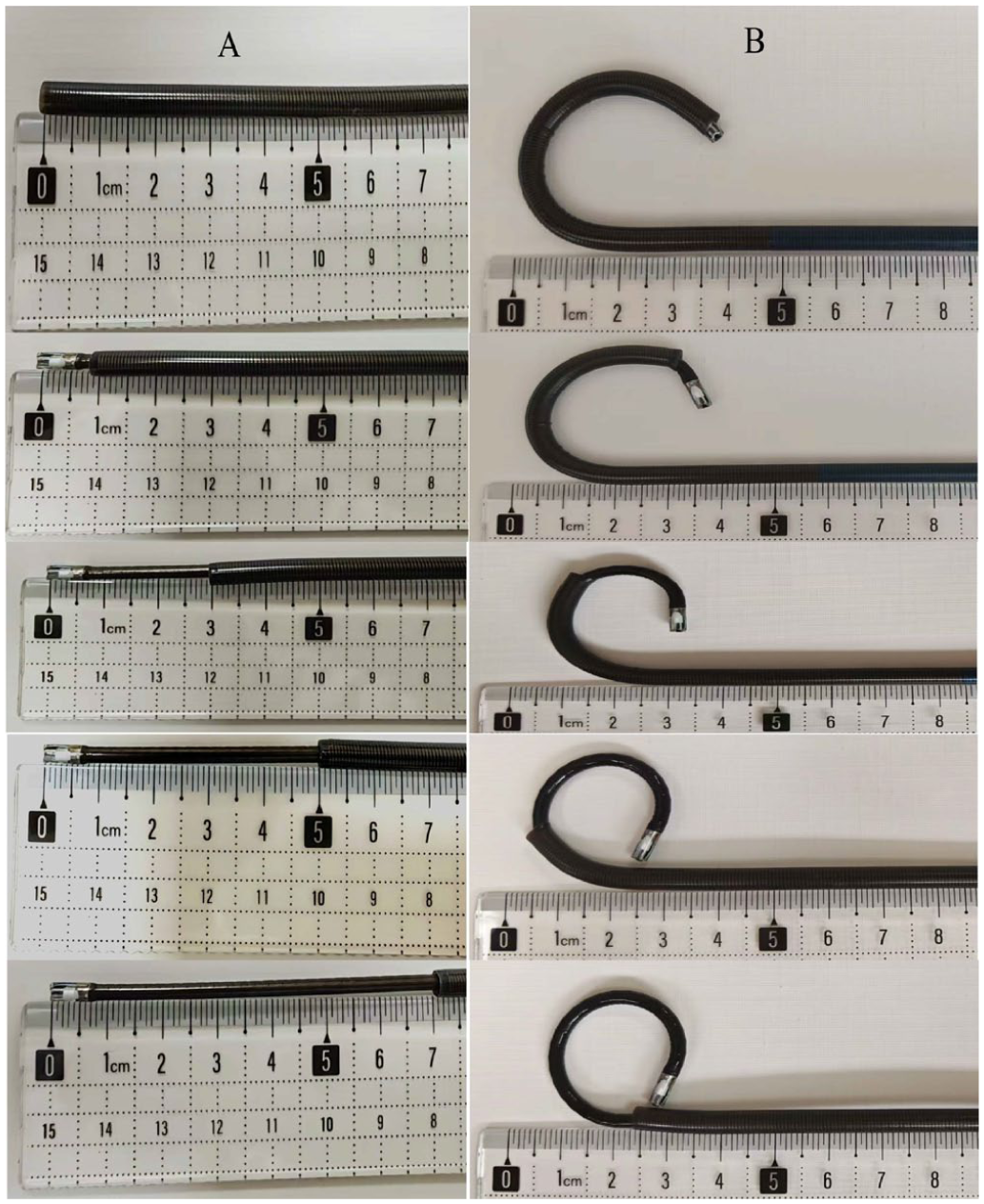
Experimental setup for measuring fURS deflection. (a) The fURS is in a neutral (straight) position, extended from the UAS. (b) The fURS at its maximum manually applied deflection, extended from the sheath.

Measurement of the maximum deflection angle using imageJ software. The image demonstrates the method for angle quantification. The apex of the fURS deflection curve was used as the reference point to measure the maximum achievable bending angle under each experimental condition.
Surgical methods
All procedures were performed under general anesthesia with the patient in the lithotomy position. Following standard sterile preparation, a rigid ureteroscope was inserted transurethrally into the bladder. Under fluoroscopic and direct visual guidance over a safety guidewire, the ureteroscope was advanced to the kidney pelvis. The guide wire was secured, and the rigid scope was withdrawn.
Experimental group (combined Sotn-URS/fURS technique)
The standard ureteroscope of the Sotn system, coupled with its modified rigid UAS, was advanced over the guidewire to the kidney pelvis under direct vision. The UAS was positioned at the ureteropelvic junction and secured, after which the standard scope was removed. The operating table was tilted approximately 30° toward the non-operative side. The integrated negative-pressure suction was connected and set to 5–10 kPa, with continuous irrigation maintained at 165–265 mL/min. The fURS was then introduced through the UAS. Upon identifying the target stone in the lower calyx, a retrieval basket was deployed through the fURS working channel. The stone was engaged and displaced to the ureteropelvic junction or proximal ureter. For stones too large to capture intact, initial laser fragmentation (0.8–1.3 J, 20–30 Hz) was performed to create a smaller fragment or a “wedge” for basket engagement (Figure 5). Following successful displacement, the fURS was exchanged for the Sotn lithotripsy scope equipped with a 365 µm laser fiber. Laser lithotripsy (0.8–1.3 J, 20–30 Hz) was performed using a fragmentation mode, with the negative-pressure suction actively removing fragments in real time (Figure 1(d)). Finally, the fURS was reinserted for a systematic inspection of all calyces to check for residual fragments. A safety guidewire was placed, the instruments were removed, and a double-J stent was deployed. A urinary catheter was placed at the conclusion of the procedure.

Schematic of the “wedge” displacement technique using fURS and a retrieval basket. (a) The target stone is in its original position within the lower calyx. (b) Initial laser lithotripsy is performed to fragment the stone and create a wedge-shaped defect. (c) The retrieval basket is advanced and engaged within the created wedge. (d) The stone fragment is successfully displaced from the lower calyx to a more accessible location.
Control group (conventional fURS with FV-UAS)
After securing guidewire access, the FV-UAS was placed over the wire. The operating table was tilted similarly. The suction system was attached to the FV-UAS (5–10 kPa, irrigation 165–265 mL/min). The fURS was introduced. Upon stone visualization, a 200 µm laser fiber was used for lithotripsy, employing a dusting and fragmenting technique (0.8–1.3 J, 20–30 Hz) to reduce stones to fragments ⩽2 mm. Larger residual fragments were retrieved with a basket. Post-lithotripsy, the collecting system was inspected with the fURS. The procedure concluded with guidewire placement, removal of the fURS and FV-UAS, insertion of a double-J stent, and placement of a urinary catheter.
Evaluation indicators
Preoperative indicators: Demographic and clinical data included age, sex, history of hypertension or diabetes, stone laterality, body mass index, preoperative stent status, stone maximal diameter, stone volume (calculated as π × length × width × height × 0.167), mean stone density (Hounsfield units), degree of hydronephrosis (pelvicalyceal separation), IPA, urine leukocyte status, and preoperative serum levels of white blood cells, hemoglobin, and creatinine.
Intraoperative observation indicators: First-attempt success rate of UAS placement, total surgical time, intrarenal operation time, number of intraoperative respiratory pause events, primary surgeon fatigue (assessed using the Borg 10-point scale, Table 1), 17 and incidence of ureteral mucosal injury. Ureteral mucosal injury was graded intraoperatively using the Traxer-Thomas system 18 (Grade 0: no lesion or only mucosal petechiae; Grade 1: mucosal erosion or flap without smooth muscle injury; Grade 2: damage to mucosa and smooth muscle but intact adventitia; Grade 3: full-thickness perforation; Grade 4: total avulsion). For analysis, grade 0 was considered “no injury,” and grades 1–4 were classified as “injury.”
Borg 10 scoring scale.

Postoperative observation indicators: Duration of urinary catheterization, stent indwelling time, postoperative hospital stay, total hospitalization costs, incidence of postoperative fever (>38.5°C), postoperative serum levels of white blood cells, hemoglobin, and creatinine, immediate postoperative SFR, and SFR at 4-week follow-up. Stone-free status was defined by non-contrast CT as either no residual fragment or fragments ⩽2 mm in maximum diameter. 19
Statistical methods
Statistical analyses were performed using SPSS 27.0, Chicago, IL, USA. Categorical variables are described using numbers (percentages) and were compared using the chi-squared test, continuity-corrected chi-squared test, or Fisher’s exact test, as appropriate. Continuous variables are presented as mean ± standard deviations and were compared using the independent samples t-test or the Mann–Whitney U test, depending on the distribution normality (assessed by the Shapiro–Wilk test) and variance homogeneity (assessed by Levene’s test). A two-sided p-value of less than 0.05 was considered statistically significant.
Results
In vitro model testing of maximum deflection angles of fURS under different interventions
Testing revealed that the deflectable segment of the fURS comprised a bidirectional bending structure. The maximum deflection angle of the unloaded fURS (with no instrument in the working channel) was 295.7° (Table 2).
Maximum deflection angles of the fURS under different experimental conditions.

fURS, flexible ureteroscopy; FV-UAS, flexible vacuum-assisted ureteric access sheath.
When inserted into the FV-UAS, the achievable deflection of the fURS increased progressively as the length of the scope extending beyond the sheath increased (from 0 to 7 cm). The corresponding maximum angles were 221.4°, 245.6°, 267.6°, 290.8°, and 293.4°, respectively. The deflection approached the scope’s inherent maximum when extended 7 cm beyond the FV-UAS, which was comparable to the angle achieved (293.6°) at the same extension length from the modified rigid UAS (Table 2).
We then evaluated the impact of inserting different instruments into the working channel on fURS deflection. The placement of a retrieval basket resulted in a maximum deflection angle of 293.4°, while insertion of a 200 µm laser fiber yielded an angle of 293.3°. By contrast, the 365 µm laser fiber caused a significant reduction in maximum deflection to 270.1° (Table 2). These findings indicate that while both laser fibers and the retrieval basket can reduce the maximum deflection of the fURS, the effect is minimal for the 200 µm fiber and the basket, but substantial for the 365 µm fiber.
Comparison of preoperative general information between the two groups
No statistically significant differences were observed between the experimental and control groups in any of the assessed preoperative demographic, clinical, or stone characteristic parameters (Table 3). The two groups were well-matched at baseline, confirming their comparability for subsequent outcome analyses.
Comparison of preoperative baseline characteristics between the two groups.

Data are presented as mean ± standard deviation or number (percentage).
Comparison of surgical and postoperative outcomes between the two groups
The experimental group demonstrated superior performance across multiple key intraoperative and efficacy endpoints compared to the control group (Table 4).
Comparison of surgical observational indicators between two groups of patients.

Data are presented as mean ± standard deviation or number (percentage).
Statistically significant (p < 0.05).
Efficacy outcomes
Regarding procedural success and efficiency, the experimental group showed significant advantages. The first-attempt success rate for UAS placement was significantly higher in the experimental group (91/114, 79.8%) than in the control group (72/126, 57.1%; p = 0.001). Both total operative time and intrarenal fURS operation time were markedly shorter in the experimental group (51.7 ± 12.2 vs 70.4 ± 13.6 min, p < 0.001; and 22.2 ± 10.1 vs 52.2 ± 12.3 min, p < 0.001, respectively).
Stone clearance rates were significantly better in the experimental group at both assessment time points. The immediate postoperative SFR was 97/114 (85.1%) in the experimental group versus 92/126 (73.0%) in the control group (p = 0.022). This advantage was maintained at the 4-week follow-up, with SFRs of 104/114 (91.2%) and 103/126 (81.7%), respectively (p = 0.033).
Safety and procedural parameters
The experimental technique was associated with improved safety and ergonomic outcomes. The incidence of intraoperative ureteral mucosal injury was significantly lower in the experimental group (4/114, 3.5%) than in the control group (14/126, 11.1%; p = 0.026). Surgeon-reported procedural comfort, as measured by the Borg scale, was significantly better in the experimental group (0.63 ± 0.65 vs 2.9 ± 1.1; p < 0.001). The number of intraoperative respiratory pause events was also lower in the experimental group (16/114, 14.0% vs 32/126, 25.4%; p = 0.029).
Other postoperative outcomes
No statistically significant differences were observed between the two groups in secondary postoperative parameters, including duration of urinary catheterization, ureteral stent indwelling time, postoperative hospital stay, total hospitalization costs, incidence of postoperative fever (>38.5°C), or postoperative laboratory values (white blood cell count, hemoglobin, and serum creatinine levels) (all p > 0.05).
Discussion
The efficacy of FURL in treating lower calyx stones is intrinsically constrained by the interplay between kidney anatomy and the mechanical limitations of the endoscope. The fURS incorporates a deflectable distal segment, which in the tested model encompasses the terminal 7 cm and provides bidirectional, manually controlled deflection. Our in vitro experiments demonstrated that this deflection capability was significantly impeded when the scope’s deflectable portion was not fully extended beyond the UAS due to mechanical constraint from the sheath wall. 20 Deflection progressively improved as the extension length increased, reaching the maximum only when the scope was extended 7 cm beyond the sheath. This underscores the surgical principle that precise UAS positioning, typically at the ureteropelvic junction or proximal ureter, is critical to ensure complete deployment of the fURS deflectable segment within the kidney collecting system.
The development of flexible, deflectable ureteral sheaths aims to mitigate this limitation by allowing coordinated bending with the fURS, potentially improving stone localization and, when combined with suction, clearance efficiency. 21 However, our experimental data revealed a persisting constraint: when the tips of the fURS and a flexible sheath were aligned (0 cm extension), their combined deflection was markedly reduced to 221.4°. This indicates that for patients with an acute IPA or stones situated deep in the dependent lower calyx, the available deflection, even with a deflectable sheath, may remain insufficient for effective in situ lithotripsy. Consequently, in such anatomically challenging scenarios, alternative strategies such as stone displacement merit consideration.
The selection of instruments for managing lower calyx stones under fURS guidance necessitates a critical balance, dictated by the interplay between their biomechanical properties and the challenging anatomy. The holmium laser fiber, with its silica core, introduces inherent rigidity. Consequently, while a larger-diameter fiber (e.g., 365 µm) facilitates greater energy delivery, it proportionally and significantly compromises the fURS deflection—a finding quantified in our in vitro study, which showed a reduction to 270.1°, versus 293.3° with a 200 µm fiber.12,22 This biomechanical limitation translated directly into a decisive clinical constraint: the restricted deflection with a 365 µm fiber frequently rendered target stones in the lower calyx inaccessible or even invisible, thereby precluding effective lithotripsy. By contrast, the stone retrieval basket—typically constructed from nitinol for its elasticity and excellent compliance with scope deflection 23 —had a markedly lesser impact on maneuverability, reducing the maximum deflection only slightly to 293.4°. These comparative data formed the foundational rationale for our procedural strategy. To achieve the primary goal of reliable stone access and displacement—a prerequisite for any treatment—preserving near-maximal fURS deflection was paramount. Therefore, we prioritized the use of the nitinol basket as the primary tool for stone manipulation. Its ability to extend laterally 0.5–1 cm beyond the scope tip at full deflection further enhanced stone engagement. When laser application was deemed necessary during the displacement phase, the 200 µm fiber was the deliberate choice. For stones ⩽20 mm, it provides sufficient lithotripsy efficiency 12 while minimizing the impairment of deflection, irrigation flow, and visual field. This represents an optimized compromise, grounded in experimental evidence, that balances scope deflection capability, lithotripsy efficiency, and procedural visibility. By using this instrument hierarchy, we could successfully relocate stones from the unfavorable lower calyx to a more accessible position in the renal pelvis or proximal ureter, setting the stage for efficient subsequent fragmentation.
The negative pressure combination rigid ureteroscope (Sotn-URS) is a detachable lithotripsy system that combines a rigid ureteroscope with a standard scope through a modified rigid UAS. This system is primarily indicated for ureteral stones, where the standard ureteroscope is first inserted through the UAS to locate the stones; following this, the lithotripter is engaged to perform Holmium laser fragmentation while negative pressure suction concurrently evacuates the debris. This modality is also applicable to stones in the kidney pelvis and upper to middle calyces and can be adapted for lower calyx stones by using the fURS. 15 In the experimental group of this study, we implemented a sequential strategy of “rigid-scope-soft-scope-basket combined displacement.” After establishing a stable conduit using the standard ureteroscope and UAS, the stones were displaced using the fURS combined with a stone retrieval basket. The lithotripter was then employed to accomplish fragmentation and clearance. This strategy combines the complementary advantages of each instrument: the stable access channel and efficient suction-assisted lithotripsy of the rigid ureteroscope system, together with the flexibility of the fURS for stone displacement. Conventional fURS procedures require continuous pressure on the deflection lever to maintain the angulation of the scope. This not only leads to operator fatigue but also complicates precise targeting, as respiratory motion can displace the stone. 22 By contrast, the technique used in this study used the fURS exclusively for stone displacement rather than for fragmentation. This is evidenced by the significantly shorter intrarenal operation time for the fURS (22.2 ± 10.1 min) compared to the control group (52.2 ± 12.3 min) and the substantially lower Borg score for hand fatigue (0.63 ± 0.65 vs 2.9 ± 1.1). These outcomes verify that the presented strategy not only facilitates efficient fragmentation by using the complementary characteristics of the instruments but also enhances procedural ergonomics for the primary surgeon.
Notably, a systematic review and meta-analysis indicates that for lower pole kidney stones ⩽2 cm in diameter, the SFR achieved with stone displacement (86%) is significantly higher than that with in situ lithotripsy (71%), without increasing complication rates or operative time. 23 However, a recognized limitation of conventional displacement techniques is that stones are relocated to the ureteropelvic junction for fragmentation, where laser energy poses a risk of thermal injury to the ureteral wall and subsequent stenosis. Moreover, displaced stones may migrate with irrigation flow and potentially fall back into the lower pole. By contrast, the combined Ston-URS offers distinct advantages: under stable negative-pressure suction, stones are anchored at the sheath opening, which minimizes stone movement and prevents retropulsion. Laser lithotripsy is performed inside the ureteral sheath, which provides a protective barrier that reduces direct energy exposure to the ureteral mucosa. Instead of pursuing a dusting strategy, the technique allows for efficient fragmenting into larger pieces, which are then promptly evacuated through the sheath via continuous negative pressure. This approach not only improves stone clearance and procedural efficiency but also reduces operative time.
The rigid UAS is constructed from metallic material, which prevents luminal collapse under pressure and maintains stable negative pressure suction. When combined with the negative pressure system, this characteristic offers three core advantages. First, continuous outflow and circulating suction prevent stone migration and maintain relatively fixed stone positioning. This allows smaller fragments to be immediately evacuated through negative pressure during lithotripsy, while larger stones can be removed through retropulsion. Second, the real-time anchoring of stones enables the surgeon to manually adjust the negative pressure valve during the procedure. This facilitates concurrent fragmentation and clearance, reduces the likelihood of stone migration to other calyces, and lowers postoperative residual rates. Third, it simplifies the process of using a retrieval basket after fragmentation to extract residual stones, thereby shortening total clearance times.14,15 In this study, residual stones were defined as fragments <2 mm. The experimental group demonstrated a significantly higher immediate stone clearance rate (85.1%) compared to the control group (73.0%). This advantage was sustained at the 4-week follow-up, with clearance rates of 91.2% and 81.7% in the experimental and control groups, respectively.
The duration of ureteroscopic lithotripsy surgery should be limited to under 90 min, with staged surgeries considered when necessary to minimize intraoperative and postoperative complications. 24 In the experimental group, stone retrieval was primarily achieved using a retrieval basket. For larger stones not amenable to complete basket capture, the strategy involved initial laser fragmentation to create manageable fragments or a surface “wedge,” followed by basket engagement for displacement. This approach ensured high stone displacement efficiency. The fURS accommodates a 365 µm laser fiber for fragmentation, providing significantly greater lithotripsy power compared to the 200 µm fiber in the control group, thereby reducing fragmentation time. Furthermore, the rigid ureteroscope offers superior directional stability, enabling quicker insertion and withdrawal through the ureteral sheath. However, the flexible ureteral sheath is approximately 10 cm longer than the rigid sheath combination, increasing the procedural working length and potentially extending operative time. The experimental protocol of performing simultaneous fragmentation and suction shortened the clearance time and simplified the surgical workflow. This is reflected in the significantly shorter total operative time for the experimental group (51.7 ± 12.2 min) compared to the control group (70.4 ± 13.6 min).
Postoperative fever and ureteral stricture are common complications of fURS surgery.25,26 Ureteral strictures may develop postoperatively due to direct mechanical injury or perforation of the ureteral wall (e.g., from guide wires, laser fibers, or ureteroscopes), the presence of foreign bodies (e.g., guide wires or ureteral sheaths), thermal injury (e.g., from lasers), or ischemia (e.g., from impacted stones), all of which can initiate inflammatory processes in the ureteral wall.27,28 The combined rigid ureteroscope technique facilitates sheath placement under direct visualization. This approach effectively mitigates injury to the ureteropelvic mucosa during sheath insertion and reduces the need for sheath depth readjustment, thereby enhancing placement safety. In addition, since the procedure involves anchoring stones to the distal end of the negative pressure sheath and delivering laser energy within the sheath lumen for fragmentation, the risk of iatrogenic ureteral strictures secondary to laser thermal injury is significantly reduced. The experimental results demonstrate a higher first-pass sheath placement success rate in the experimental group (79.8%) compared to the control group (57.1%). Furthermore, the incidence of ureteropelvic mucosal injury was significantly lower in the experimental group (3.5%) than in the control group (11.1%). The stable lumen of the rigid ureteroscope, coupled with continuous outflow and suction, provides enhanced visualization during the procedure. This allows for real-time assessment of the ureteropelvic mucosa and intrarenal pressure. Indicators of low intrarenal pressure include a semi-filled kidney pelvis with clearly visible mucosal folds and small gaps between the mucosa and stones. By contrast, high intrarenal pressure is suggested by the gradual disappearance of mucosal folds, enlargement of spaces, and the appearance of pinpoint mucosal hemorrhages. Excessively strong negative pressure may lead to the complete collapse of the gap between the mucosa and the stones. Utilizing these indicators enables real-time monitoring of intrarenal pressure, which may contribute to reducing the incidence of postoperative septicemia.
This study has several limitations. First, its retrospective design may introduce selection bias. Second, the follow-up period was relatively short (4 weeks), which may not fully reflect long-term outcomes. Third, the Sotn-URS system currently lacks real-time intrarenal pressure monitoring. Future prospective, multi-center studies with longer follow-up are warranted to validate these findings.
Conclusion
The stone displacement technique utilizing a combined Sotn-URS and fURS approach significantly enhances the stone-free rate for lower calyx stones ⩽20 mm, reduces total operative and intrarenal fURS time, and lowers the risk of ureteral mucosal injury. Furthermore, it improves surgeon ergonomics without increasing the incidence of other complications or overall healthcare costs. This technique offers a safe, efficient, and easily adaptable novel surgical strategy for managing this challenging subset of kidney stones.
Supplemental Material
sj-docx-1-tau-10.1177_17562872261423750 – Supplemental material for Stone displacement with combined Sotn ureteroscopy and flexible ureteroscopy for lower calyx stones ⩽20 mm: a retrospective comparative study
Supplemental material, sj-docx-1-tau-10.1177_17562872261423750 for Stone displacement with combined Sotn ureteroscopy and flexible ureteroscopy for lower calyx stones ⩽20 mm: a retrospective comparative study by Jianping Zhang, Mengqing Li, Shaomei Lin, Xiaoxia Wu, Qinhua Guo, Haiying Chen, Ming Lin, Zihuang Hong, Rongkai Lin and Lingfeng Zhu in Therapeutic Advances in Urology
Footnotes
References
Supplementary Material
Please find the following supplemental material available below.
For Open Access articles published under a Creative Commons License, all supplemental material carries the same license as the article it is associated with.
For non-Open Access articles published, all supplemental material carries a non-exclusive license, and permission requests for re-use of supplemental material or any part of supplemental material shall be sent directly to the copyright owner as specified in the copyright notice associated with the article.