
Abstract
The use of robot-assisted technology has been widely adopted in urological oncological surgery and its benefits have been well established. In recent years, robotic technology has also been used in several functional reconstructive and neuro-urology (FRNU) procedures. The aim of this review was to evaluate the current evidence in the use of robotic technology in the field of FRNU. We performed a PubMed-based literature search between July and August 2022. The keywords we included were ‘robotic assisted’, ‘ureteric reimplantation’, ‘cystoplasty’, ‘ileal conduit’, ‘neobladder’, ‘sacrocolpopexy’, ‘colposuspension’, ‘artificial urinary sphincter’, ‘genitourinary fistula’ and ‘posterior urethral stenoses’. We identified the latest available evidence in the use of robotic technology in specific FRNU procedures such as the reconstruction of the ureters, bladder and urinary sphincter, urinary diversion, and repair of genitourinary prolapse and fistula. We found that there is a lack of prospective studies to assess the robotic-assisted approach in the field of FRNU. Despite this, the advantages that robotic technology can bring to the field of FRNU are evident, including better ergonomics and visual field, less blood loss and shorter hospital stays. There is therefore a need for further prospective studies with larger patient numbers and longer follow-up periods to establish the reproducibility of these results and the long-term efficacy of the procedures, as well as the impact on patient outcomes. Common index procedures and a standardized approach to these procedures should be identified to enhance training.
Keywords
Introduction
Functional reconstructive and neuro-urology (FRNU) is a subspecialty of urology that covers a broad range of benign conditions. The aetiology of these conditions varies greatly from congenital abnormalities to iatrogenic causes.1–5 Likewise, the management of FRNU conditions ranges from conservative, pharmacological to surgical interventions. Prior to subjecting patients to surgical treatment, a thorough assessment (often including urodynamic studies and radiological imaging) is undertaken.
Open surgery has always been the traditional gold standard for FRNU conditions. Recently, the use of laparoscopic and robotic-assisted surgery has gained popularity amongst different surgical specialties, including urology. Minimally invasive techniques are widely used in uro-oncological procedures such as radical nephrectomy 6 and prostatectomy, 7 which is now becoming the new standard of care. 8 Thanks to enlarged 3D vision, high mobility instruments, improved ergonomics and fluorescence vision; and robotic surgery offers solutions to overcome technical difficulties, particularly some of them frequently faced in FRNU: narrow pelvic operating area, long and difficult suturing steps, and irradiated hypovascularized structures.
However, there has been slower adoption of minimally invasive surgery, particularly robotic surgery, in FRNU due to several reasons. Firstly, the advancement of pharmacological treatment and endoscopic surgery allows more patients to avoid major surgery to achieve symptom control. Secondly, several FRNU procedures such as incontinence surgery, fistula repair and genito-urinary prolapse repair are undertaken through perineal access. In general, minimally invasive surgery has been applied in procedures through the transabdominal approach. Thirdly, training opportunities are limited and there are no common index procedures where surgeons can build or train their skills. Finally, many FRNU patients requiring surgical management would have undergone prior surgeries, resulting in a more complex and challenging operation, which may limit the surgeon’s opportunity to utilize novel surgical approaches in such cases.
Despite the challenges identified in adopting robotic surgery in FRNU patients, surgeons benefit from using novel technologies that have been confirmed in uro-oncology procedures, including enhancement of ergonomics, access and vision. Moreover, comparable benefits could be demonstrated in patients too, including faster recovery, shorter hospital stay and better cosmesis. This review looks at the latest evidence for the use of robotic surgery in a variety of FRNU procedures and discusses potential future implementations that may help promote this technology.
Methodology
We performed a literature search on the PubMed database between July and August 2022 for published evidence on robotic-assisted surgery on various procedures in the field of FRNU. The keywords we included were (‘robotic assisted’ OR ‘robotic’) AND (‘ureteric reimplantation’ OR ‘cystoplasty’ OR ‘ileal conduit’ OR ‘neobladder’ OR ‘sacrocolpopexy’ OR ‘colposuspension’ OR ‘artificial urinary sphincter’ OR ‘genitourinary fistula’ OR ‘posterior urethral stenoses’). There was no time limit applied and we only included studies written in English. The focus is on the most recent evidence and the most relevant articles were included for this review. In addition, from the reference list of the chosen studies, we also identified further eligible studies to be included in the review.
Sacrocolpopexy
Abdominal sacrocolpopexy (SC) is proven to be effective and demonstrates superior outcomes over different vaginal procedures in the management of apical and multi-compartment pelvic organ prolapse.9,10 Robot-assisted sacrocolpopexy (RASC) surgery was first reported in 2004. 11
A meta-analysis of 2916 RASC cases from 49 studies between 2004 and 2020 demonstrated that the procedure was feasible, safe and effective. The conversion to open rate was low at 0.76%. Among the 49 studies, 34 recorded 2029 patients’ treatment outcomes, and 1852 (91.3%) patients have been followed up, with a median follow-up of 12 months (ranging from 1 to 62 months). The objective cure rate, defined as a POP-Q (Pelvic Organ Prolapse Quantification) grade of ⩽1 based on a gynaecological examination, ranged from 82.35% to 100%. The prolapse recurrence rate was 7.2%, and the reoperation rate for these recurrences was 18.7% (25 of 134 recurrence cases). 12
The median operative time of RASC was 226 min. The estimated mean blood loss was 56 ml, while the mean length of hospital stay of 1.55 days. When compared with laparoscopic sacrocolpopexy, RASC was associated with significantly lower blood loss [weighted mean difference (WMD) = −58.48 ml], but longer operative time (WMD = 37.35 min). There was, however, no significant difference in the length of hospital stay (WMD = 0.31).
Colposuspension
Surgical procedures are indicated for women with stress urinary incontinence (SUI) who failed to respond to conservative measures. Following the FDA notifications on transvaginal mesh, the utilization of synthetic slings for SUI has been questioned. As a result, there has been a resurgence of native tissue techniques such as autologous fascial sling and the Burch procedure 13 Robot-assisted Burch colposuspension was first reported in two cases in 2007 by Khan et al. 14 Further case reports were published in 2015, 2017 and 2020.13,15,16
In 2021, Lee et al. published a retrospective study of 76 patients who underwent robotic-assisted Burch colposuspension between 2013 and 2019. This study showed that the procedure was feasible with reasonable short-term outcomes. Amongst the patients, 50 cases underwent concomitant procedures at the time of the operation, while the remaining 26 cases underwent robotic-assisted Burch urethropexy alone. The treatment success rate, defined by more than 50% improvement in post-operative 3-day voiding diary and negative stress cough test, was 85% with a mean follow-up time of 134 (±157.8) days. 17
A prospective study in 2022 done by Tan et al. looked at the post-operative outcomes of 28 women who underwent robotic-assisted laparoscopic colposuspension. The patients had a mean follow-up period of 12 months and this showed a significant 73% improvement in mean 24-h pad usage. The study also demonstrated a significant improvement in the Urinary Incontinence Short Form Questionnaire scores post-operatively (from 18.1 to 9.4). 18

One pitfall that surgeons may encounter when performing robotic colposuspension is the lack of haptic sensation 19 during a procedure in which it is necessary to apply some tension at the level of the bladder neck. Placing the stitches too loose may not improve incontinence.
Apart from these two studies, the evidence on this technique is limited. It is evident that adequate long-term data are lacking. Further clinical trials with larger patient numbers are required to compare robotic colposuspension to other modalities.
Ureteric reimplantation
Ureteric reimplantation is the definitive treatment for distal ureteric strictures. Robotic-assisted ureteric reimplantation (RAUR) was first described in 2003 by Yohanes et al. 20 In 2011, a study led by Kozinn et al. compared the perioperative outcomes of robotic versus open distal ureteral reimplantation. This study showed that the patients who underwent RAUR had a significantly lower estimated blood loss and shorter length of stay in the hospital. Post-operative narcotic use was less in the robotic group, although this was not statistically significant. Both robotic and open groups achieved clinical resolution of ureteric obstruction with subsequent MAG-3 renogram not demonstrating recurrence in either group (median follow-up of 30 and 24 months in the open and RAUR groups, respectively). 21
In 2015, Wason et al. published a case series of 13 patients who underwent RAUR. Their results showed that all procedures were successfully completed robotically without the need for conversion to open. Most patients required a short hospital stay, and no patients had a leak on cystogram after an average of 8 days (range: 4–27 days). This case series also noted a 23% (with six complications in three patients) post-operative complication rate (two Clavien-Dindo grade 1, two Clavien-Dindo grade 2, two Clavien-Dindo grade 3). The authors concluded that RAUR is a safe procedure with good short-term outcomes but recognized that extensive adhesions, typically seen in patients with complex prior surgical history, was the main challenge to undertaking RAUR 22 .
When comparing outcomes of patients undergoing RAUR and those undergoing conventional laparoscopic ureteral reimplantation, no significant differences in operation time, intra-operative bleeding and length of hospital stay could be identified. Both groups had achieved resolution of symptoms clinically and radiologically. 23
In 2021, Dell’Oglio reported the largest single-centre series of RAUR, with 37 patients included. Operating time ranged greatly from 117 to 323 min, the authors attributed this to the learning curve effect and the variation in complexity of the cases. The complication rate was 27% with two patients requiring further surgical intervention. With a median follow-up of 24 months, five patients had asymptomatic hydronephrosis but all the patients had stable renal function. The authors concluded that RAUR was safe and feasible for patients with ureteric stricture. 24

RAUR has also been utilized in the paediatric group as a treatment for vesicoureteric reflux. In 2016, Bowen et al. observed that between 2000 and 2012 in the United States, there was a decrease in a number of paediatric ureteral reimplantation; however, the proportion of RAUR increased from 0.3% to 6.3%. It was also reported that the length of stay is shorter for the robotic-assisted approach when compared to the open approach, with a mean length of stay of 1.6 and 2.4 days, respectively. 25 RAUR for vesicoureteric reflux can be performed by intravesical or extravesical approach. In 2017, Baek and Koh summarized the reported literature on these two approaches. For the intravesical approach, the reflux resolution rate was between 83% and 100% and the complication rate ranged from 0% to 52%. There were more studies looking at the extravesical approach of RAUR, the reflux resolution rate ranged from 77% to 100% and the complication rate ranged from 2% to 30% with the most common complications being febrile UTI and urinary retention, ranging from 1% to 18% and 3% to 40%, respectively. The lack of standardization in surgical steps along with the learning curve may contribute to this wide variation in complication rate. 26 A further review by Howe et al. had similar findings with the authors concluding that the slow adoption of the robotic technique in paediatric ureteric reimplantation is due to its lower success and higher complication rates as compared to the open approach. 27
In 2020, Kanojia reported their experience with four paediatric vesicoscopic Cohen’s reimplantation using the robotic approach. The results showed the resolution of reflux in all the patients on follow-up voiding cysto-urethrogram at a mean follow-up of 9 months. Kanojia et al. recognized that the procedure is technically challenging with a steep learning curve but the tissue dissection and suturing are easier as compared to laparoscopic surgery. It was suggested that a larger set of data is required to establish the additional benefits of robotic vesicoscopic reimplantation when compared to other methods. 28
In 2022, Carbonara et al. published a systematic review of the comparative outcomes of RAUR versus open ureteric reimplantation (OUR). It showed that there is no difference in operative time (WMD – 6.22 min) and overall complication rate (odds ratio 0.85) in RAUR and OUR. However, the estimated blood loss (EBL) (WMD – 121.71 ml) and length of stay (WMD – 2.39 days) were significantly lower in RAUR. In the 90-day follow-up period, there was no difference in the readmission and stricture recurrence rate. 29
In conclusion, the evidence for RAUR is currently limited, indicating the need for a larger number of patients to assess the efficacy, reproducibility and long-term outcomes of the results. It is also important to consider factors contributing to the varying complication rates.
Augmentation cystoplasty
Augmented cystoplasty is usually reserved as a final treatment option for patients experiencing a low compliance bladder and/or overactive bladder with failed pharmacological and surgical management, including botulinum toxin-A injection and sacral neuromodulation. One of the first robotic-assisted laparoscopic augmentation illeocystoplasty in adults was described in 2010 by Kang et al. 30 In this case report, the patient suffered from urinary frequency with a functional bladder capacity of 100 ml. The operative time was 300 min with 225 ml of blood loss. The patient was discharged on day 14. Post-operatively, the bladder capacity increased to 350 ml and the functional capacity improved to 280 ml.
In 2016, Cohen et al. published a retrospective comparative study of robotic total intracorporeal versus open cystoplasty in paediatric patients. There were 17 and 15 patients, in the open and robotic groups, respectively. They identified a significantly longer operative time in the robotic group with a median operative time in the robotic cohort of 623 versus 265 min in the open group. Other perioperative parameters such as estimated blood loss, intravenous morphine usage and length of stay were comparable. In terms of clinical outcomes, all patients had stable or improved renal appearances on ultrasound (US). Post-operative bladder capacity was not measured routinely but from the collected data, both groups demonstrated an increase in bladder capacity, with a mean increase of 150% and 94.5% in the robotic group and open group, respectively. In terms of post-operative complications, the open group had a greater major reoperation rate of 11.8% for bowel complications while the robotic group had none. 31
In 2021, Grilo et al. presented their results on 10 patients who had undergone intracorporeal robot-assisted supratrigonal cystectomy and augmentation cystoplasty (RAAC). The mean operative time was 250 min and the mean length of stay was 13 days. Four of the patients had a complication at the 30-day follow-up, two had UTI, one had bleeding at the trocar site requiring arterial embolization and two had post-operative ileus. Two of the patients developed urinary fistula (one at 6 weeks, one at 9 months). All patients were reported to be continent at the last follow-up and subsequent urodynamic studies in all confirmed a significant improvement in bladder capacity (maximum mean capacity increased from 260 to 515 ml). The authors concluded that with a standardized technique and careful selection of patients, RAAC is a safe and feasible procedure. 32
From the limited studies thus far, it can be summarized that robotic-assisted cystoplasty is feasible and can lead to symptomatic improvement and increased bladder capacity; however, further studies are required to understand the long-term efficacy and complications rate.
Ileal conduit
Ileal conduit (IC) is the most common form of urinary diversion as the technique is straightforward and reliable. In addition to its use after radical cystectomy, it is also used as a last resort in refractory overactive bladder and/or low compliance bladder. A total intracorporeal urinary diversion has the advantage of smaller incision, less post-operative pain, lower associated paralytic ileus and a decreased third space fluid loss. 33
In 2000, Gill et al. showed that constructing an intracorporeal ileal conduit (ICIC) is feasible by laparoscopy. 34 Subsequently, a case report on ICIC using robotic assistance was published in 2003. 35 In 2004, a robotic-assisted laparoscopic total ICIC was reported by Balagi et al., 36 three patients were included (two with radiation cystitis and one with bladder cancer who underwent total ICIC along with radical cystectomy). The mean operative time was 691 min. The estimated mean blood loss was 250 ml and one patient who underwent radical cystectomy received a blood transfusion post-operatively. There were no major complications detected during the follow-up period of a median of 4.5 months.
The initially reported operative times were a limiting factor; however, it has been shown that operative time decreased with increased experience and increased volume of cases performed. In a cumulative analysis of 83 studies by Tanneru et al. in 2021, 37 the mean operative time (including cystectomy, pelvic lymph node dissection and urinary diversion) for ICIC was 313 ± 54 min compared to extracorporeal (ECIC) 428 ± 18 min.
In the metanalysis by Tanneru et al., 37 a higher proportion of patients with American Society of Anaesthesiologist (ASA) score > 3 were detected in the extracorporeal urinary diversion group, which may be due to the longer time needed for intracorporeal diversion (especially during the early period of the learning curve) and with potential for increased early post-operative complications which frailer patients may not withstand. They also showed that the 1-month overall mean complication rate was 59% in the ICIC versus 44% in the ECIC group. While the 3-month overall complications in ICIC was 39% compared to 77% in ECIC. There was no significant difference between both groups regarding the incidence of early or late overall mean complications.
A study of 65 patients who underwent cystectomy and IC urinary diversion for neurogenic lower urinary tract dysfunction was published by Deboudt et al. in 2016. The authors compared the outcomes between different approaches, including open, laparoscopy and robotic assisted. No significant difference in IC formation time, EBL and length of stay was found across the groups. Post-operatively, the restoration of bowel function was significantly faster in the robotic group (4 days), when compared to the open (5.9 days) and laparoscopic (4.5 days) groups. Regarding early morbidity (<30 days), there was a significantly higher rate of haemorrhagic complications in the laparoscopic group (28.6%) when compared to the open and robotic-assisted groups (9.1% and 5%, respectively). The late (>30 days) major complication rate was lower in the robotic-assisted group, although not significant. 38
In summary, robotic ICIC is feasible and associated with evident positive post-operative outcomes. However, more studies on this technique are required. The significant complication rates seen above indicate that mastering of the surgical technique of this complex procedure is vital.
Neobladder
The first robotic-assisted intracorporeal neobladder (ICNB) was reported in 2003, using a ‘W’ configuration pouch based on the Hautmann neobladder. 39 Since then, many other ICNB reconstructive techniques have been adopted in an attempt to reduce operative time, such as the Studer ‘U’ modified neobladder, 40 the ‘Y’ neobladder,41,42 the Padua neobladder, 43 and the Shell neobladder. 44
In the systematic review by Karthik et al., a total of 2593 patients underwent robotic assisted radical cystectomy with diversion in six studies. The intracorporeal cystectomy group involved 1334 patients, of which only 22% had neobladder as compared to IC (78%). This is likely attributable to the technically demanding nature of ICNB creation, the long learning curve and patient preference for IC. 37
In the cumulative analysis of 83 studies, it was found that the ICNB group has a mean operative time of 428 ± 42 min, which is similar to the extracorporeal neobladder (ECNB) (426 ± 72 min). 37 It is worth noting that, from the largest multi-centre series consisting of 2125 patients performed by Hussein et al. in 2017, the operative time was shorter in the intracorporeal diversion (358 min) when compared with the extracorporeal diversion (406 min). 45 On the other hand, there are three studies consisting of 64, 108 and 126 patients, respectively,46–48 which showed a longer operative time for intracorporeal urinary diversion (ICUD) as compared to extracorporeal urinary diversion (ECUD), with mean operative times being (581 versus 468), (306 versus 288) and (420 versus 360) min, respectively. These data suggest that higher procedure volume and increased experience were associated with reduced operative time for intracorporeal diversion; therefore, intracorporeal diversion may become the preferred method for diversion.
The ICNB group had a lower mean blood loss (198 ± 109 ml) and a lower rate of blood transfusion when compared to the ECNB group (365.3 ± 187.5 ml). There was a significant difference in blood loss and consequently blood transfusion rates between both groups. ICNB and ECNB had comparable short-term and mid-term complication rates. The 3-month overall complication rate in the ICNB group was 33% and 77% in the ECNB group. In addition, the urethra–neobladder stricture rate in the ECNB group was noted to be significantly higher (23% versus 0%), which may be explained by increased manipulation of urethra and neobladder in comparison to the ICNB group. 49
In conclusion, there is a lack of randomized prospective studies comparing the results of different techniques of robotic ICNB.
Artificial urinary sphincter
The indications for artificial urinary sphincter (AUS) insertion implantation are congenital neurogenic (spina bifida), acquired neurogenic (injury to the spinal cord), congenital non-neurogenic (e.g. bladder exstrophy complex) and acquired non-neurogenic (e.g. post-prostatectomy incontinence and refractory female SUI due to sphincter deficiency]. 50 Considering the first three indications, the cuff of the prosthesis is placed around the bladder neck, to prevent the risk of urethral erosion in wheelchair-bound patients and/or those needing intermittent self-catheterization. Despite the variety of indications, the largest body of evidence for AUS is based on male SUI after radical prostatectomy and is still considered the ‘gold standard’ for this indication for several decades. 38 Currently, it regains also interest for the treatment of persistent female SUI after failed surgical treatment.
In 2013, a robotic AUS (R-AUS) placement in six male patients with neurogenic stress urinary incontinence (SUI) was first reported with a mean operative time of 195 min (175–250 min). 51 Although Yates et al. showed that robotic insertion of AUS appears safe, technically feasible and associated with complete continence in all patients, another R-AUS series of four male patients had less promising results with persistent incontinence in 50%. 52 However, a monocentric retrospective study included all consecutive adult male neuro-urological patients who underwent laparoscopic robot-assisted AUS was published in 2022. Overall, 19 men were included. No conversion to laparotomy was needed. Three minor early post-operative complications occurring in 15.8% of patients were reported. At the end of the follow-up, the continence rate was 89.5%. The AUS revision and explantation rates were 5.3% and 0%, respectively. 53
Robotic AUS in women has been described by several groups. Peyronnet et al. reported a multi-centre study of 49 patients who had undergone robot-assisted AUS surgery performed by 10 surgeons. The mean operative time in this study was 180 min (120–300 min). There were eight intraoperative complications (16.3%): five bladder neck (BN) injuries and three vaginal injuries. Nine patients experienced post-operative complications (18.3%), but only two were Clavien 3 (4.1%). After a median follow-up of 18.5 months, one explantation (2.1%) and three revisions (6.1%) were required. In all, 40 patients were fully continent (81.6%), six had improved continence (12.2%) while three patients’ symptoms had remained unchanged (6.1%). This study showed that R-AUS in women was feasible, safe and reproducible with functional outcomes in the early learning curve comparable with those described in a large series of open AUS implantation. 54 Conversely, a smaller series with a mean operative time of 142 min (127.5–174 min) showed a significant incidence of adjacent organ injury (bladder, vagina) (in 4/11 women). 55 After a mean follow-up of 17.6 months, seven patients (87.5%) achieved complete continence and one patient (5.8%) has improved continence. Four patients (36%) experienced post-operative complications, but only two were categorized as Clavien 3 (18%).
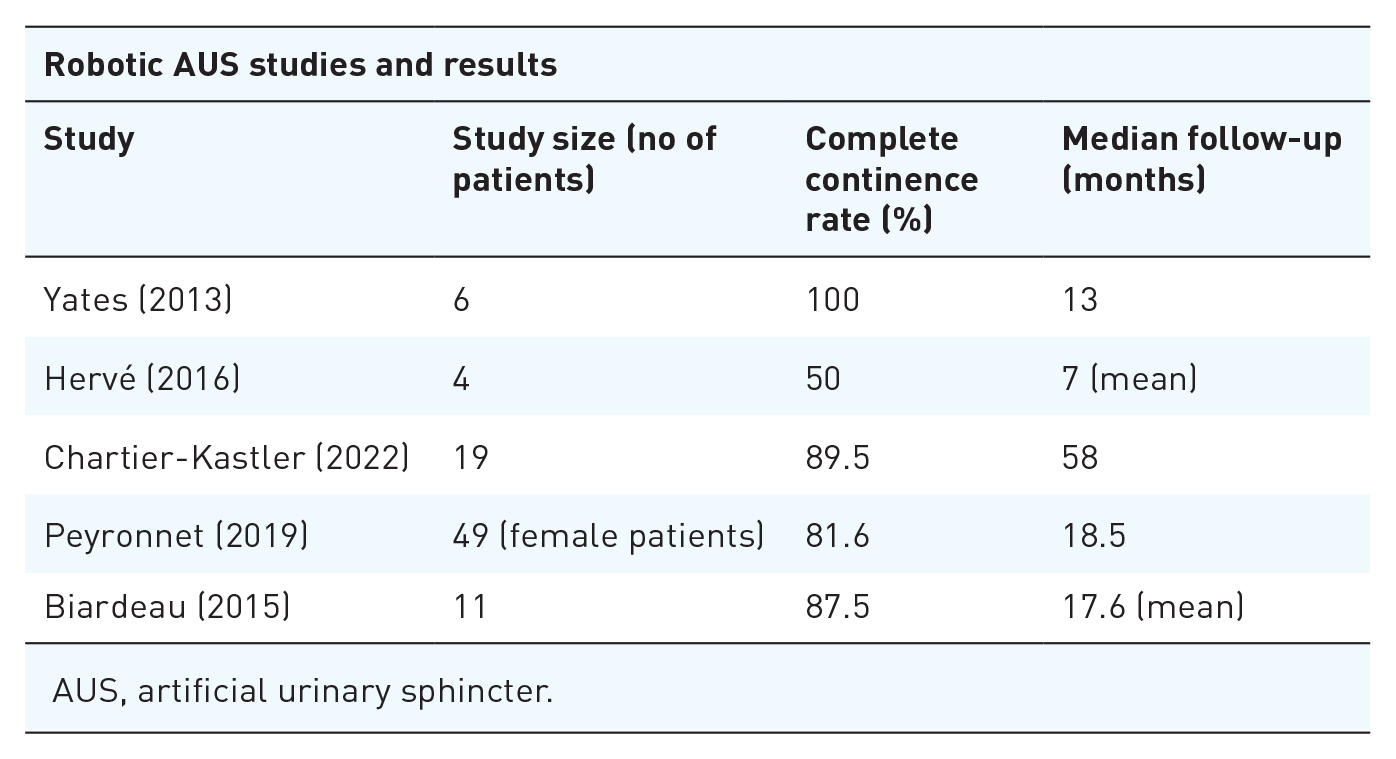
AUS, artificial urinary sphincter.
From a technical point of view, surgeons may find robotic bladder neck dissection challenging during R-AUS. Peyronnet et al. 54 described a technique where the operating surgeon relies on an experienced assistant’s digital control in the vagina to facilitate the dissection of the vesicoviganal plane, to minimize the risk of the bladder neck and vaginal injury. Chartier-Kastler et al. described a posterior approach in bladder neck dissection during R-AUS. The authors commented that patients who had previous urethral sling operations can make the procedure more challenging as this may hinder the bladder neck dissection and cuff placement. 56
Although the surgical approach may have eminent advantages, particularly in women, a larger body of evidence is required in both men and women with SUI to evaluate the risk–benefit ratio under critical consideration of the cost of robotic surgery for this procedure.
Genitourinary fistula
The vesicovaginal fistula (VVF) is the commonest acquired fistula of the urinary tract. While gynaecological surgery, in particular abdominal hysterectomy, is the most common cause of VVF in developed countries, persistent obstructed labour is the most common cause in developing countries. 57 Transvaginal approach is advocated for low-lying VVF, while the transabdominal approach is recommended for supratrigonal or complex VVF, when vaginal access is difficult, or when concomitant intra-abdominal surgery is being considered.
The use of minimally invasive approaches is growing in an attempt to reduce the morbidity associated with open abdominal VVF repair. 58 In this regard, laparoscopic repair has been used for supratrigonal VVF. However, it has been noted that this was associated with a steep learning curve for laparoscopic suturing and difficulties with access and ergonomics. These issues have been mitigated with the introduction of robotic surgery. 59
Robotic repair of VVF was first reported in 2005. 60 This has been followed by publications of various case series which revealed the feasibility and safety of this technique with a reported success rate ranging from 71.4% to 100%.61–66 However, the series is generally small in number. There are only three studies that included more than 15 patients, with a respective mean operative time of 127.5 min (100–270), 133 ± 48 min and 187 min (151–219 min), and a reported success rate of 100%, 93.3% and 91%.57,58,67
Most surgeons have used the conventional transvesical approach with some form of tissue interposition. A robotic extravesical approach for VVF repair was first reported in 2007 by Schimpf et al. 63

In summary, due to the small number of VVF cases repaired robotically in addition to the heterogeneity of studies, there is a need for more prospective and comparative studies with greater patient numbers and longer follow-ups.
Posterior urethral stenoses
Posterior urethral stenoses (PUS) often result from pelvic trauma or surgical treatment of either benign or malignant prostate disease. Reconstructive surgery of the posterior urethra is known to be challenging due to the nature of the anatomy. The posterior is located deep in the pelvis and is close to the pelvic bone. Its proximity to the urinary sphincter also risks patients being incontinent following posterior urethroplasty. 68 Endoscopic dilatation and incision are usually used as the initial approach to manage PUS. However, this approach carries a high recurrent stricture rate (up to 90%) and is particularly ineffective in patients who have had previous radiation.69,70
The first case series of robotic approach in managing bladder neck contracture (BNC) was in 2017. A total of 12 patients who underwent robotic-assisted laparoscopic Y-V plasty were included in this series and the median follow-up period was 23.2 months. A success rate of 80% was reported and there were two patients who experienced recurrent BNC post-surgery. A total of 6 patients (50%) experienced minor post-operative complications such as urinary tract infection, anaemia requiring blood transfusion, epididymitis and transient stress incontinence were observed in this group of patients. 71
Kirshenbaum (2018) reported his experience with robotic bladder neck reconstruction on 12 patients. It is worth noting that none of the patients in this cohort received any prior pelvic radiation or operation that involved perineal dissection. These patients had an average follow-up of 13.5 months and the success rate was reported as 75% (success defined by the ability to pass a 17 Fr cystoscope) with the continence rate reported to be 82%. 72 In the same year, Granieri (2018) reported a similar success rate in seven patients who had undergone robotic Y-V plasty for bladder neck contracture. These patients had a success rate of 100% and continence was preserved in 71% of patients at a median follow-up for 8 months. 73 Unterberg (2018) also reported similar results in 10 patients who had robotic-assisted proximal perineal urethroplasty. A 100% success rate was observed at 12 months post-operative cystoscopy check. 74
Bearrick (2022) reported her experience in robotic urethral reconstruction in 20 patients with posterior urethral stenosis. Amongst the patients, 10 had benign prostate hyperplasia (BPH) treatment, 5 had radical prostatectomy alone and 5 had radiotherapy prior to radical prostatectomy. When comparing the three groups of patients, patients who had received prior radiotherapy required a significantly longer operative time (p ⩽ 0.01) compared to the other two groups. The median operative time for patients who had prior radiotherapy was 8.58 h, while the BPH group and prostatectomy alone group had a median operative time of 4.03 h and 5.44 h, respectively. In the follow-up period, the BPH group and the prostatectomy-alone group achieved anatomical (defined as able to pass a 17 Fr cystoscope) and functional success (post-void residual urine of <50 cc) rate of 90%–100% whilst the radiotherapy group had a significantly lower success rate of 60%. The pad per day usage was also significantly greater in the radiotherapy group (10.5 pads per day) compared to the other two groups of patients (0 pads per day) and therefore consequentially more likely to require an AUS insertion. A total of 30-day complications were observed in both the prostatectomy-alone group and radiotherapy group were 20% and 40%, respectively, these complications include anastomotic dehiscence, fluid collection and uro-symphyseal fistula formation. 75

Historically, posterior urethral strictures were mainly managed endoscopically, and open reconstructive surgery is often used as a final option. There are multiple studies on open repair of posterior urethral stricture achieving a high success rate ranging from 60% to 92%. In these cases, success is usually defined by the ability to pass a 17 Fr cystoscopy at follow-up. These studies often follow up patients for a long period of time with the median follow-up time between 45 and 75 months. The main downside of the open approach is the low continence rate (0–35%) that it was associated with.76–80 Overall, it has been demonstrated that robotic reconstruction of posterior urethral stenosis has a comparable outcome compared to the open technique. The robotic case series were achieving a patency rate similar to the open cases. It was found that the robotic approach was able to preserve a higher continence rate, ranging from 75% to 82%; while the open cases have a notably lower continence rate post-operatively. 69 However, the currently available evidence of a robotic approach to posterior urethral reconstruction only consists of a small patient sample size and a much shorter follow-up period compared to the studies on the open approach. It is therefore difficult to deduce the long-term outcome of the robotic approach.
Conclusion
The utilization of robotic surgery is growing in the field of FRNU. The largest body of evidence for robotic surgery exists for SC, which confirmed the efficacy and safety of the procedure with reduced blood loss compared to the laparoscopic approach. However, despite the evidence in SC procedure, from our review of the different surgical procedures seen in FRNU, it is obvious that there is a lack of robust prospective studies and randomized controlled trials. Moreover, studies with a larger patient number, particularly with functional and neurological conditions, and longer follow-up time are warranted to assess the reproducibility of these results and particularly the long-term efficacy of the procedures.
It is also noted that there is a great degree of variability in the complication rate encountered across the different studies. This may be explained by the lack of surgical consistency as the technique is still in the experimental phase or due to the complex patient population which has often undergone various prior surgeries. It is therefore vital that a standardized approach is established for each procedure. This will facilitate training which should be incorporated in the subspecialty training in FRNU for surgeons to feel comfortable and confident in using the technology. Common index procedures should be identified to facilitate such training.