
Abstract
Background:
The aim of this study was to report the outcomes of artificial urinary sphincter (AUS) in women with stress urinary incontinence (SUI) resulting from intrinsic sphincter deficiency after a follow up of 10 years.
Methods:
The charts of female patients with moderate-to-severe SUI who underwent open AUS implantation between November 1994 and April 2007 were reviewed retrospectively. All patients were operated on by a single experienced surgeon through an open retropubic approach with systematic bladder incision. Primary endpoint was postoperative continence categorized as complete continence (no pads used), improved incontinence, or unchanged incontinence.
Results:
A total of 63 women (mean age: 58 years, range: 17–82) underwent open AUS implantation. There were seven (11.1%) intraoperative complications. At the last follow up, 26 (41.3%) initial AUSs remained in situ and 21 (33.3%) patients had at least one revision or reimplantation. Of these 47 patients (74.6%), 35 (74.5%) were fully continent, 3 (6.4%) had improved incontinence, and 9 (19.1%) had unchanged incontinence. A total of 20 patients (31.7%) experienced postoperative complications, but only 2 (3.2%) were Clavien ⩾3. After a median follow up of 14 ± 6 years, 20 (31.7%) explantations and 29 (46%) revisions occurred. The average time without explantation or revision was 11.6 and 9 years, respectively.
Conclusions:
In our experience, AUS is a good option for women with moderate to severe SUI, with good long-term outcomes.
Keywords
Introduction
Artificial urinary sphincter (AUS) in female patients is known to give good rates of satisfaction and functional outcome (continence estimated between 42% and 86%), 1 but is not widely used due to operative difficulties. AUS implantation is extremely challenging, especially after multiple anti-incontinence surgeries, and patient selection can also be difficult. We have performed this procedure since 1994, as described initially by Light and colleagues, 2 first by the open approach and then laparoscopically, although robot-assisted AUS implantation has recently emerged in some countries.
Our aim here is to report the outcomes of AUS in women with moderate-to-severe stress urinary incontinence (SUI) resulting from intrinsic sphincter deficiency (ISD) after a minimum follow up of 10 years.
Materials and methods
This retrospective, descriptive, analytical study reviewed the charts of all female patients who underwent open AUS (AMS 800; Boston Scientific, Marborough, MA, USA) implantation for SUI due to ISD between November 1994 and April 2007 in our institution. After 2007, AUS implantation was performed with a laparoscopic approach.
Preoperative management
All patients underwent a clinical interview and physical examination. Maximal urethral closure pressures (MUCP) were calculated during urodynamic studies. ISD was defined as clinical stress incontinence with fixed urethra and low MUCP (<50 cmH2O).
Cognitive function and dexterity were evaluated at consultation. In accordance with the patient, every operative step was explained by local staff.
Operative management
All patients were operated on by a single experienced surgeon (CS) through an open retropubic approach with systematic opening of the bladder dome and full access to the vagina. The AUS pressure regulating balloon reservoir was placed in the Retzius space and the pump was inserted in the major labia after dilation. Deactivation of the system was checked by radioscopy on day 1 (AUS system was filled with saline + contrast agent).
Postoperative management
AUSs were activated after 6 weeks, and postoperative outcomes were assessed during follow up appointments at 3, 6, and 12 months, and every year thereafter.
Outcome measurements
The primary endpoint was the degree of continence categorized as complete continence (no pads used), improved incontinence, or unchanged incontinence. This was assessed both short-term (at 1 year) and long-term (>10 years). The secondary endpoints were any complications, explantations and revision-free time.
Statistical analysis
Continuous variables are represented as mean (min-max) or median [interquartile range (IQR)]. Categorical variables are represented as number and percentage. All statistical tests were performed using SPSS Statistics, version 22.0, statistical software (IBM Corporation, Armonk, NY, USA).
Results
Patient characteristics
From November 1994 (first case in the institution) to April 2007, 63 female patients underwent open AUS implantation in our insti-tution. Mean age was 58 years (range: 17–82). Considering SUI, 45 (71.4%) patients had idiopathic ISD and 18 (28.6%) had neurogenic ISD (3 performed self-catheterization and 2 were wheelchair-bound). A total of 52 patients (82.5%) had a history of previous pelvic surgery (11 patients did not experience pelvic surgery before AUS implantation from 1995 to 2005), and two patients (3%) had a history of pelvic radiotherapy. Mean maximal urethral closure pressure was 27 cmH20 (range: 9–50). The characteristics of the patients are summarized in Table 1.
Characteristics of the study population (n = 63).

Short-term functional outcomes
After 1 year, 51 patients (81%) were fully continent, 6 (9.5%) had improved incontinence and 5 (7.9%) had unchanged incontinence; 5 patients (7.9%) needed AUS explantation (2 urethral erosion, 1 vaginal erosion, and 2 labial erosion) 3 three (4.7%) needed AUS revision (2 experienced pump migration, and 1 atrophy of the bladder neck requiring cuff replacement).
Long-term functional outcomes
After a median follow up of 14 years (IQR: 0.2–22.9), 20 explantations (31.7%) and 29 revisions (46%) occurred. The average time without explantation (Figure 1) or revision (Figure 2) was 11.6 and 9 years, respectively. The fully continent rate was 55.6%.

Kaplan–Meier analyses for explantation-free survival.

Kaplan–Meier analyses for revision-free survival.
At the last follow up, 26 patients (41.3%) still had their initial AUS in situ and 21 patients (33.3%) had an AUS after at least one revision or reimplantation. Of these 47 (74.6%) patients, 35 (74.5%) were fully continent, 3 (6.4%) had improved incontinence and 9 (19.1%) had unchanged incontinence (6 patients were not able to use the AUS due to cognitive impairment, 1 required a tension-free vaginal tape (TVT) sling, 1 required botulinum toxin injections because of associated detrusor overactivity, and one patient died prematurely at day 22 with an inactivated AUS). These results are summarized in Table 2.
Long-term functional outcomes.
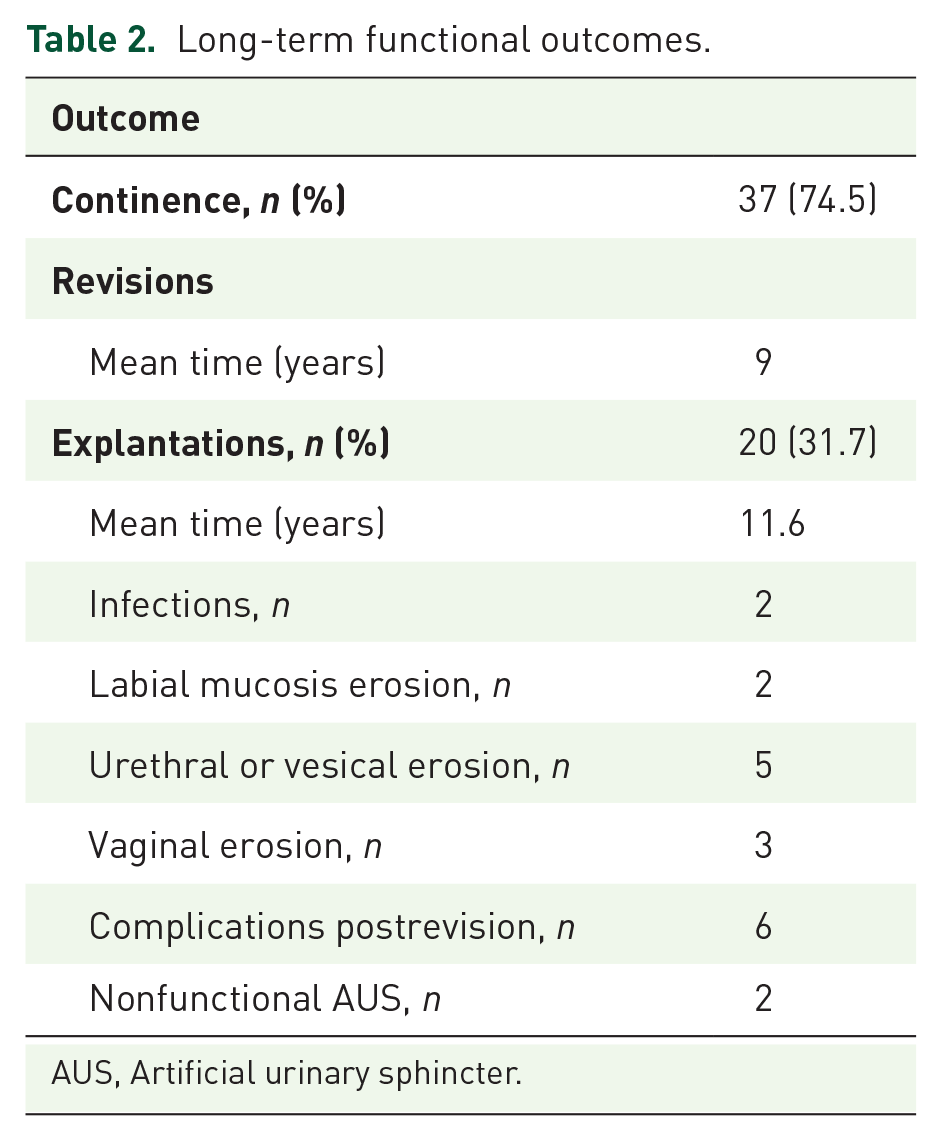
AUS, Artificial urinary sphincter.
Perioperative outcomes
Mean length of hospital stay was 9 days (range: 6–22) postsurgery. There were seven intraoperative complications (11.1%): one urethral injury, three bladder neck injuries, and three vaginal injuries. A total of 20 patients (31.7%) experienced postoperative complications, but 18 (28.5%) were Clavien <3 and only two (3.2%) were Clavien ⩾3: one superficial abscess requiring a scar revision and drainage and one acute pulmonary distress leading to death at day 22.
Discussion
This cohort study reports a series of women who received an AUS implantation via the open approach, with a median follow up time of 15 years. In light of the postoperative continence rate of 56%, our real-life study confirms that AUS gives excellent functional results in female patients with SUI.
SUI is a worldwide public health issue with a severe social and psychological impact, which affects a patient’s quality of life. 3 Unlike in men, given the lack of evidence-based data, AUS is not yet recognized as a gold standard in women but as an optional or second-line treatment. In the case of female SUI, the first-line surgical techniques recommended by learned societies are midurethral slings and TVT or transobturator tape. 4
Functional long-term results after AUS implantation have previously been reported to be acceptable. In the systematic review published by Reus and colleagues in 2018, evaluating the safety and effectiveness of AUS in non-neurogenic women, 1 the complete continence rates, defined as ‘no pad’, were reported to range from 42% to 86% across studies using the open technique. In female neurological patients with SUI, AUS has a complete continence rate of 71.4%. 5 The heterogeneity of the complete continence rate may be explained by follow up variability between the studies, ranging from 17 to 204 months in the review of Reus and colleagues. 1 Phé and colleagues demonstrated that a short follow up was not sufficient to assess the occurrence of serious side-effects. 5 Our study includes the longest follow up with a median of 15 years. It is noteworthy that both neurogenic and non-neurogenic incontinence were considered indiscriminately in our study, which leads to a certain heterogeneity of the population, but allows an evaluation of the overall effectiveness of AUS in female SUI.
In accordance with the literature,6,7 the explantation rate in our study was around 30%. The major risk factors for explantation are pelvic irradiation, age >70 years, neurological pathology, and a history of pelvic surgery, including the Burch procedure and sacral colpopexy,6,8,9 In our study, patients had a mean age of 58 years, and 28.6% had neurogenic ISD. Over 80% of the women included had undergone previous pelvic surgery, which may play a role in the occurrence of complications, and shows that implantation of an AUS was, in most cases, not the first treatment of choice.
In the present study, the average time without explantation or revision was 11.6 and 9 years, respectively. The revision rate reported in the review of 11 studies by Reus and colleagues is reported to range from 6% to 45%. 1 When studies with identical follow up and the open approach are considered,10–12 the revision rate varied from 32% to 45%, and is, therefore, in line with our results.
One of the main limitations of our study is the absence of a validated incontinence questionnaire, since our surgeries started 15 years ago. Owing to their age, some of the data in our study cannot also be correctly interpreted, in particular hospital stay, which was clearly longer 15 years ago for this type of surgery. Another limitation to be considered in our study is the realization of AUS implantation by retropubic laparotomy. Surgical techniques have now improved and a laparoscopic, or even robotic, approach has to be considered nowadays.13–15 In the case of a laparoscopic or robotic approach, the ‘no pad’ rates reported in the literature ranged from 63% to 83%, but the follow up was shorter and fewer patients were included.13,15,16 Given the limited information available in the literature, it is still premature to try to compare the performance and safety of the different surgical techniques and further prospective studies are required. We think, however, that a good experience with open AUS implantation is a prerequisite for laparoscopic/robotic AUS implantation due to the risk of difficulties encountered, notably in women with a history of previous pelvic surgery.
To our knowledge, this is the largest series with the longest follow-up of female incontinent patients treated by open AUS implantation. In our experience, AUS can provide excellent long-term functional outcomes in female patients with SUI, but at the cost of high revision and explantation rates.
Footnotes
Acknowledgements
All authors have read and approved the paper.
Author contributions
Drafting of the manuscript: T. Tricard, F. Jochum; critical revision of the manuscript: S. Bergerat, P. Munier, C. Saussine, A. Schroeder.
Funding
The author(s) received no financial support for the research, authorship, and publication of this article.
Conflict of interest statement
The authors have no conflicts of interest to declare.
Ethical statement
Our study did not require an ethical board approval because it was a retrospective study with oral patient consent.
Presentation
A part of this work was presented at European Association of Urology congress in Barcelona on the 19th of March, 2019.