
Abstract
Background and objectives:
Patients with bladder cancer (BC) are at high risk for recurrence rates and readmission costs. However, the evidence about obesity and metabolic abnormalities on the BC prognosis was inconsistent. Our primary aim was to determine the impact of obesity and different metabolic status on the readmission risk in patients with BC.
Design and methods:
We identified 16,649 patients with BC using the 2018 Nationwide Readmissions Database who were hospitalized from January to June 2018 and followed for 180 days. The primary outcome was 180-day readmission. The multivariate Cox regression analysis and ordered logistic regression were performed to analyze data.
Results:
Obesity and metabolic abnormalities were associated with an increased readmission risk in patients with BC [obesity: adjusted hazard ratio (aHR) = 1.08, 95% confidence interval (CI): 1.01–1.16; hyperglycemia: aHR = 1.11, 95% CI: 1.05–1.17; hypertension: aHR = 1.09, 95% CI: 1.03–1.15]. Compared with non-obese and no metabolic abnormalities, the risk of readmission was significantly increased in patients with metabolic abnormalities, irrespective of obesity (non-obese and metabolic abnormalities: aHR = 1.07, 95% CI: 1.02–1.13; obese and metabolic abnormalities: aHR = 1.20, 95% CI: 1.10–1.31), but not in obese and no metabolic abnormalities. These associations were consistent in patients aged 60 years or older and the surgery group. Moreover, hyperglycemia, hypertension, and a graded increment of metabolic risk were associated with an increased readmission risk. We also found increased length of stay for readmission in patients with obesity and metabolic abnormalities (aOR = 1.17, 95% CI: 1.00–1.36).
Conclusion:
Obesity with metabolic abnormalities and metabolic abnormalities alone were associated with higher readmission risks in patients with BC. It is suggested that prevention should focus not only on obesity but also on metabolic abnormalities to decrease the risk of readmission.
Introduction
Bladder cancer (BC) is characterized by high recurrence rates and the need for lifelong surveillance, 1 which inevitably leads to readmission and generates enormous costs. 2 BC’s inpatient care is the major medical expenditure component 3 among them, of which approximately 60% in the US can be attributed to surveillance and the treatment of recurrences. 4 Readmission reflects, to some extent, the prognosis of the disease. The readmission rate is also considered a quality measure by the Institute for Healthcare Improvement. 5 Many studies have pointed out that unplanned hospital readmissions are ordinary, costly, and potentially preventable events.5–7 However, previous studies have investigated the causes of short-term readmission in patients after radical cystectomy for BC, but the risk assessment of readmission in patients with BC is lacking. 6 Consequently, more emphasis is being placed on modifiable life factors, such as obesity and metabolism, to prevent an increase in BC readmission.
Obesity currently affects over 600 million adults, with growing incidence worldwide and involving more than 1 billion people by 2030. 8 Systematic reviews and reporting data have shown that obesity-related conditions were prone to influence outcomes in patients with BC. Obesity and type 2 diabetes mellitus (T2DM) were potentially negatively associated with BC prognosis, but the effect of hyperlipidemia and hypertension on BC prognosis remained uncertain. 9 Another study found that obesity was not considered as the risk of recurrence involving 726 non-muscular invasive BC patients. 10 There might be an ‘obesity paradox’, in which obese patients with BC might experience better survival and fewer readmission than regular weight patients with BC. 11 The above evidence about metabolic abnormalities and obesity on BC prognosis was limited and inconsistent. Inconsistent results could be explained that obesity adversely affected metabolism, but not all obese subjects presented the same metabolic risk. 12 Therefore, given these conflicting views, it seems more appropriate to investigate the association of obesity or metabolic status alone or in combination with readmission risk in patients with BC.
To our knowledge, no previous studies have investigated the association between metabolically defined obesity and BC prognosis. Here, we established a retrospective cohort study using a large-scale administrative database to determine the impact of obesity and different metabolic status on the readmission risk in patients with BC, which may identify higher-risk subphenotypes and be helpful for both physicians to provide a reference for clinical prevention and intervention, resulting in reduced readmission rates, improved quality of life for patients, and reducing the economic burden.
Methods
Data source and study population
We used data from the Nationwide Readmissions Database (NRD) 2018 sample. The NRD was the publicly available inpatient database, accounting for approximately 35 million discharges each year in 28 US states. It used verified patient linkage numbers to track a person across hospitals within a state while adhering to strict privacy guidelines, containing information on last hospital discharge and readmission hospitalization (https://www.hcup-us.ahrq.gov/nrdoverview.jsp).
We included all adults with BC who were deemed ‘at-risk’ for hospitalization and contributed to follow-up time until 180 days. BC was defined by the International Classification of Diseases, Tenth Revision, Clinical Modification (ICD-10-CM) codes (Supplemental Table 1). We excluded patients with: (1) age < 18 years and pregnant (n = 96), (2) secondary BC (n = 234), (3) missing baseline characteristic data (n = 815), (5) non-first admission (n = 12,282), (4) died during the initial hospitalization (n = 1492), (5) initial hospitalization between July and December 2018 (n = 15,309), (6) low body weight patients [BMI (body mass index) ⩽ 19.9 kg/m2, n = 696] (Figure 1).

Study design, related to methods.
Data collection
We collected baseline characteristics of study participants using NRD variables: age, sex, length of stay, total charges, insurance status (Medicare, Medicaid, private insurance, self-pay, no charge or other), household income (Median household income by ZIP Code), location of residence, Healthcare Cost and Utilization Project (HCUP) Emergency Department service indicator (HCUP E_ D), disposition of the patient, smoking, drinking and comorbidities (e.g. obesity, hyperglycemia, hypertension, dyslipidemia, ischemic heart disease, chronic bronchitis, emphysema, chronic kidney disease, liver cirrhosis and dementia). We also collected data on surgery using the ICD-10-CM PCS (Procedure Coding System). The ICD-10-CM codes were given in Supplemental Table 2.
Definitions
Obesity was defined as BMI ⩾ 25 kg/m2. 13 Metabolic abnormality was described as having any two of the following based on the harmonized International Diabetes Federation criteria 14 : (1) hyperglycemia (including prediabetes and diabetes), (2) dyslipidemia (including hypertriglyceridemia and hypercholesterolemia), and (3) hypertension. Waist circumference was excluded from the definition of metabolic disorders because waist circumference was strongly related to BMI. Participants were classified into four groups according to BMI and metabolic statuses: (1) non-obese and no metabolic abnormalities; (2) non-obese and metabolic abnormalities; (3) obese and no metabolic abnormalities; and (4) obese and metabolic abnormalities.
To determine the number of metabolic abnormalities and specific metabolic abnormalities on the risk of readmission, the selected study population was classified into eight groups. The first grouping included (1) non-obese and with no metabolic abnormality; (2) non-obese and with one metabolic abnormality; (3) non-obese and with two metabolic abnormalities; (4) non-obese and with three metabolic abnormalities; (5) obese and with no metabolic abnormality; (6) obese and with one metabolic abnormality; (7) obese and with two metabolic abnormalities; (8) obese and with three metabolic abnormalities. The secondary grouping included (a) non-obese and with no metabolic abnormality; (b) non-obese and only with hyperglycemia; (c) non-obese and only with hyperlipidemia; (d) non-obese and only with hypertension; (e) obese and with no metabolic abnormality; (f) obese and only with hyperglycemia; (g) obese and only with hyperlipidemia; (h) obese and only with hypertension.
Outcome measures
The primary outcome was 180-day readmission. The 180-day readmission referred to all-cause, unplanned readmissions to the same or different hospital within 180 days. Only the first readmission was counted for patients with multiple readmissions. Elective hospitalizations for maintenance chemotherapy were not defined as readmissions. 15 Secondary outcomes of interest were length of stay during readmission.
Statistical analysis
Descriptive statistics were performed to compare the patient demographics and clinical characteristics for the initial hospitalization. Kruskal–Wallis H test was used to analyze continuous variables with non-normal distribution and uneven variances. The chi-square test was utilized for categorical variables. Continuous variables were expressed as median with an interquartile range (IQR) and categorical variables as percentages. Statistical significance was observed among the groups, and pairwise comparisons were performed. Multivariate Cox regression analysis was used to calculate the hazard ratio (HR) with 95% confidence interval (CI) for readmission. Length of stay for readmission was analyzed using multivariable ordered logistic regression model. Kaplan–Meier survival curves were plotted to estimate the cumulative no probability of readmission. Hypothesis testing was two-sided, with a p value < 0.05 deemed statistically significant. Data were analyzed by SPSS 26.0 software (SPSS Inc., Chicago, IL, USA).
Results
Baseline clinical and demographic characteristics of initial hospitalizations in patients with BC
A total of 16,649 patients were enrolled in the cohort study, and 6923 (41.6%) BC patients were considered unplanned readmission within 180 days (Figure 1). A total of 13.2% of patients who readmitted within 180-days were obese, 34.3% had hyperglycemia, 74.3% had hypertension, 46.4% had dyslipidemia (Figure 2). The average age was 75 years (IQR, 67–83 years) and males accounted for 76.9% (Table 1). Among the 16,649 patients, most patients [n = 12,915 (77.6%)] had Medicare insurance status and home was the most frequent discharge location for patients after their initial hospitalizations. Patients with 180-day readmission were more likely to have obesity, metabolic abnormalities and chronic kidney disease than those without 180-day readmission (all p value < 0.001, Table 1).
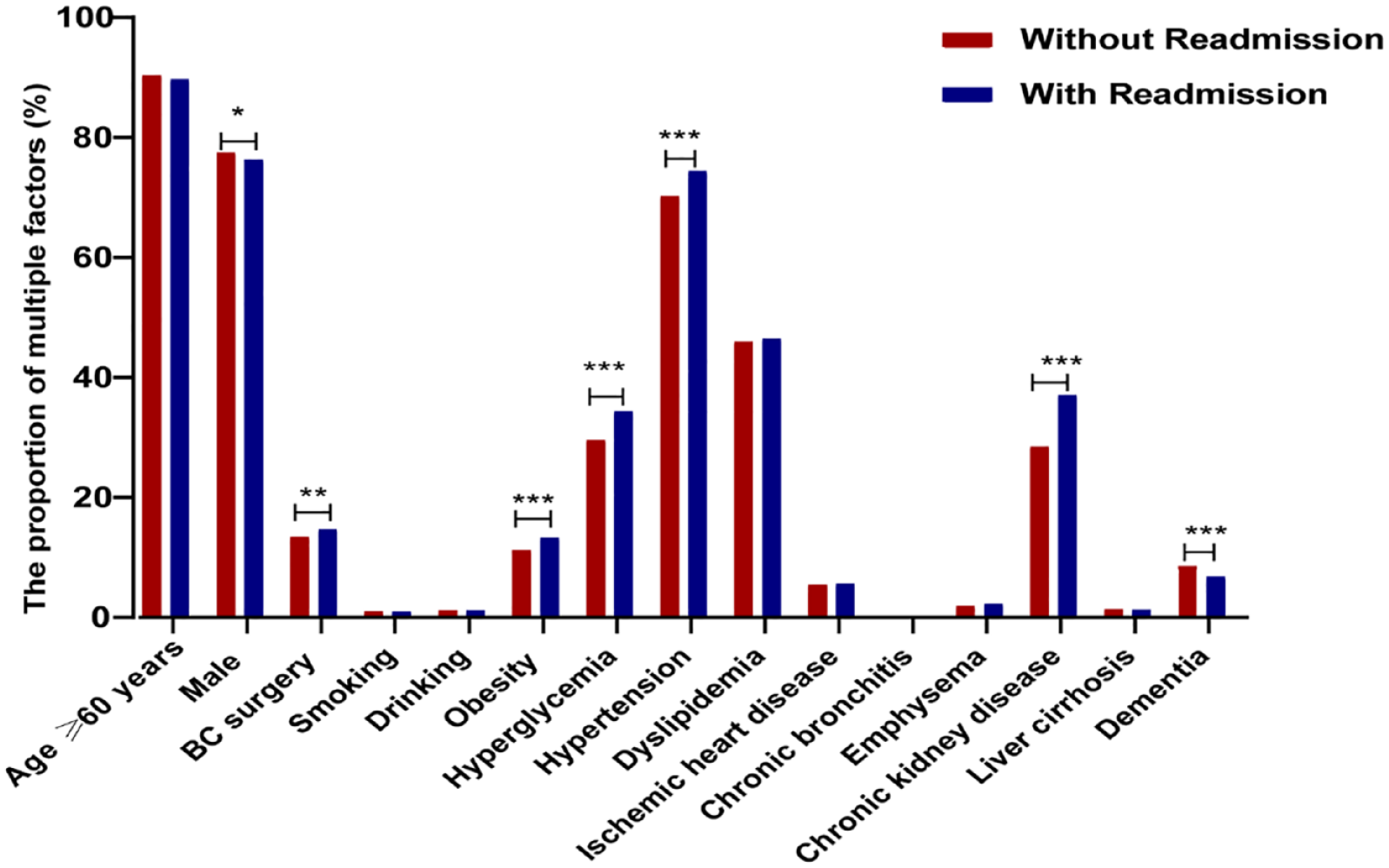
The proportion of multiple factors related to 180-day readmission after initial hospitalization in patients with BC.
Baseline clinical and demographic characteristics of initial hospitalizations in patients with BC.

The small letters (e.g. a, b) in this table refer to comparisons between groups. There is no statistical difference between groups with the same small letters.
BC, bladder cancer; HCUP, Healthcare Cost and Utilization Project; HCUP E_ D, HCUP Emergency Department service indicator; ED, Emergency Department; IQR, interquartile range.
Multivariable Cox regression analysis of 180-day readmission after initial hospitalization in patients with BC
The multivariate Cox regression model used with each estimate adjusted for all other variables in the model (Table 2). We found that length of stay in initial hospitalizations, Medicaid insurance status, ED revenue on record, BC surgery, obesity, hyperglycemia, hypertension, and chronic kidney disease increased the risk of 180-day readmission [length of stay: adjusted hazard ratio (aHR) = 1.01, 95% CI: 1.01–1.02; Medicaid insurance status: aHR = 1.30, 95% CI: 1.16–1.46; ED revenue on record: aHR = 1.35, 95% CI: 1.27–1.45; BC surgery: aHR = 1.38, 95% CI: 1.27–1.51; obesity: aHR = 1.08, 95% CI: 1.01–1.16; hyperglycemia: aHR = 1.11, 95% CI: 1.05–1.17; hypertension: aHR = 1.09, 95% CI: 1.03–1.15; chronic kidney disease: aHR = 1.28, 95% CI: 1.21–1.34] in patients with BC. Therefore, obesity and metabolic abnormalities were associated with an increased readmission risk in patients with BC.
Multivariable Cox regression analysis of 180-day readmission after initial hospitalization in patients with BC.

The multivariate Cox regression model used with each estimate adjusted for all other variables in the model.
aHR, adjusted hazard ratio; BC, bladder cancer; CI, confidence interval; HCUP E_ D, HCUP Emergency Department service indicator; HCUP, Healthcare Cost and Utilization Project.
The relationship between metabolically defined obesity and the 180-day readmission in patients with BC
Patients with obesity had more hospitalization costs and longer hospitalization duration than those without obesity, regardless of metabolic status (p value < 0.001). In addition, patients with metabolic abnormalities were more likely to have Medicare insurance, ischemic heart disease and chronic kidney disease than those with no obesity and no metabolic abnormalities, irrespective of obesity (all p value < 0.001, Supplemental Table 3).
Over the median follow-up time of 6 months, patients with metabolic abnormalities had significantly higher rate of readmission than those with no obesity and no metabolic abnormalities, irrespective of obesity [non-obese and metabolic abnormalities: n = 3100 (42.6%) versus obese and metabolic abnormalities: n = 609 (47.7%), p < 0.05, Figure 3]. We adjusted for the potential confounders of age, sex, length of stay, total charges, insurance status, household income, location of residence, HCUP E_ D, disposition of the patient, BC surgery, smoking, drinking and ischemic heart disease, chronic bronchitis, emphysema, chronic kidney disease, liver cirrhosis and dementia. Compared with non-obese and no metabolic abnormalities, the risk of readmission was significantly increased in patients with metabolic abnormalities, irrespective of obesity (non-obese and metabolic abnormalities: aHR = 1.07, 95% CI: 1.02–1.13; obese and metabolic abnormalities: aHR = 1.20, 95% CI: 1.10–1.31), but not in obese and no metabolic abnormalities (Table 3). Kaplan–Meier survival plots found that the cumulative probability of readmission was highest in the obese and metabolic abnormalities group [Figure 4(a)].

The relationship between metabolically defined obesity and the readmission rate with BC.
Results of multivariate Cox regression analysis between obesity and metabolically defined obesity and the risk of 180-day readmission in patients with BC.

After adjusting for age, sex, length of stay, total charges, insurance status, household income, location of residence, HCUP E_ D, disposition of the patient, BC surgery, smoking, drinking and ischemic heart disease, chronic bronchitis, emphysema, chronic kidney disease, liver cirrhosis and dementia.
aHR, adjusted hazard ratio; BC, bladder cancer; CI, confidence interval; HCUP E_ D, HCUP Emergency Department service indicator; HCUP, Healthcare Cost and Utilization Project; Ob (−) MA (−), non-obese and no metabolic abnormalities; Ob (−) MA (+), non-obese and metabolic abnormalities; Ob (+) MA (−), obese and no metabolic abnormalities; Ob (+) MA (+), obese and metabolic abnormalities.

Kaplan–Meier plot for the cumulative no probability of readmission based on metabolically defined obesity (a) in total participants, (b) in patients aged 60 years and older, and (c) in BC surgery.
In patients aged 60 years and older, patients with metabolic abnormalities were more likely to be readmitted than those who were non-obese and with no metabolic abnormalities, irrespective of obesity (non-obese and metabolic abnormalities: aHR = 1.08, 95% CI: 1.02–1.14; obese and metabolic abnormalities: aHR = 1.21, 95% CI: 1.11–1.33, respectively), whereas those who were obese and with no metabolic abnormalities were less likely (Table 3). Patients with metabolic abnormalities showed a pretty apparent increased risk of readmission in the surgery group, irrespective of obesity (non-obese and metabolic abnormalities: aHR = 1.27, 95% CI: 1.10–1.46; obese and metabolic abnormalities: aHR = 1.76, 95% CI: 1.44–2.15, respectively). However, patients with metabolic abnormalities were not related to the risk of 180-day readmission in the patients under 60 years of age and non-surgical group (Table 3). Kaplan–Meier survival plots found that the cumulative probability of readmission was also highest in the obese and metabolic abnormalities group in age-specific and the surgical history [Figure 4(b) and (c)].
The relationship between the number of metabolic abnormalities and specific metabolic abnormalities and the 180-day readmission in patients with BC
After adjusting for age, sex, length of stay, total charges, insurance status, household income, location of residence, HCUP E_ D, disposition of the patient, BC surgery, smoking, drinking and ischemic heart disease, chronic bronchitis, emphysema, chronic kidney disease, liver cirrhosis and dementia, we revealed that the risk of readmission increased as the number of metabolic abnormalities increased, regardless of obesity. We also observed that obesity might exacerbate the adverse effects of metabolic abnormalities on readmission compared with non-obesity when the number of coalescent metabolic abnormalities was consistent (Table 4). In the secondary grouping, the hazards of readmission were 1.22-fold (p Value = 0.015) and 1.09-fold (p Value = 0.039) higher in non-obese and only with hyperglycemia and non-obese and only with hypertension and non-obese and with no metabolic abnormality after adjusting for same confounder. We also found that the presence of hyperlipidemia was not associated with an increased readmission risk, regardless of obesity (Table 4).
Results of multivariate Cox regression analysis between obesity and metabolic abnormalities and the risk of 180-day readmission in patients with BC.

After adjusting for age, sex, length of stay, total charges, insurance status, household income, location of residence, HCUP E_ D, disposition of the patient, BC surgery, smoking, drinking and ischemic heart disease, chronic bronchitis, emphysema, chronic kidney disease, liver cirrhosis and dementia.
aHR, adjusted hazard ratio; BC, bladder cancer; CI, confidence interval; HCUP E_ D, HCUP Emergency Department service indicator; HCUP, Healthcare Cost and Utilization Project; MA: metabolic abnormality; Ob: obese.
The relationship between metabolically defined obesity and the length of stay for 180-day readmission after initial hospitalization in patients with BC
After adjusting for age, sex, length of stay, total charges, insurance status, household income, location of residence, HCUP E_ D, disposition of the patient, BC surgery, smoking, drinking and ischemic heart disease, chronic bronchitis, emphysema, chronic kidney disease, liver cirrhosis and dementia, patients who were obese and with metabolic abnormalities were associated with higher risk of length of stay (aOR = 1.17, 95% CI: 1.00–1.36) compared with the non-obese and no metabolic abnormalities group, but patients who were non-obese and with metabolic abnormalities and obese with no metabolic abnormalities showed no significant differences (Supplemental Table 4).
Discussion
In this retrospective cohort study, metabolic abnormalities were associated with an increased readmission risk in patients with BC, irrespective of obesity. However, obesity alone was not associated with an increased risk of readmission risk. The link between obesity and BC readmission appeared to depend on metabolic status, and obesity aggravated the adverse effects of metabolic abnormalities on readmission. These associations were consistent in patients aged 60 years or older and the surgery group. Another interesting result was that readmission risk gradually increased as the number of metabolic disorders increased, regardless of obesity. Moreover, hyperglycemia and hypertension were associated with an increased readmission risk, but hyperlipidemia was not. We also found increased length of stay for readmission in patients with obesity and metabolic abnormalities.
Although the widely accepted WHO BMI classifications defined obesity as BMI ⩾ 30 kg/m2 in most scenarios, obesity was defined as BMI ⩾ 25 kg/m2 in our study. A previous study found that Asian Americans with a BMI of 25–30 kg/m2 had a similar prevalence of diabetes to White Americans with a BMI of greater than 30 kg/m2, so one size did not fit all. 16 We were devoted to determining whether the risk of BC readmission will increase once body weight is above normal, so as to highlight new at-risk individuals and populations and inform future public health prevention programs. It is well known that obesity is associated with adverse prognosis in patients with BC. The underlying mechanism might be that obesity caused metabolic and hormonal changes.10,17 Especially, chemokine ligand 1, plasminogen activator inhibitor 1, and interleukin-6 secreted by adipose tissue increased risk of BC recurrence. 18 For example, a retrospective cohort study implied that obesity, a threshold of BMI ⩾ 25, was significantly related to an increased risk of recurrence and progression in patients with BC. 19 A meta-analysis also showed that the recurrence rate was visibly greater in obese patients. 9 However, some studies have found that a BMI of ⩾25 kg/m2 was associated with improved outcomes in patients with BC.20,21 There was a complex relationship between obesity and its effect on metabolism and BC outcomes. 22 In addition, a recent multicenter experience has found that poor immuno-nutritional status is associated with a poorer postoperative course after radical cystectomy, 23 hence we excluded patients with low body weight to avoid the influence of poor nutritional status on the prognosis of BC. Our study found that obesity alone was not associated with an increased risk of readmission risk, and the underlying mechanisms for this phenomenon were that fat deposition, such as subcutaneous adipose tissue, may prevent the production of immunological substances such as Natural killer T cells and protect tissues from cancer cells metastasis. 24
In addition, similar trends were observed in the patients aged 60 years and older and surgery group. Cantiello et al. showed that metabolic syndrome was associated with high-grade complications in patients undergoing radical cystectomy based on the Clavien classification system. 25 Most patients who undergo radical cystectomy have advanced age and age-related comorbidities. 26 The age and degree of comorbid illness are strong predictors of outcome in patients with BC.26,27 In the present study, we adjusted for important confounders to exclude the impact of age-related comorbidities. The possible explanation was that BC was most likely to occur in elderly people. 20 The population >60 years accounted for 90% in our study, so the patient number might drive this difference with age. Yet another possible explanation was that older people may be more susceptible to weight loss or metabolic abnormalities due to the disease itself or the drugs, which may lead to reverse causation (weight change as a consequence rather than a cause of BC). The patients were followed for only 1 year due to the limitation of NRD database. Therefore, further research is needed to determine the mechanism, especially in older patients.
Moreover, we understood that assessing BC readmission with metabolic disorders was complicated because of the different clinical combinations of the various metabolic abnormalities. Therefore, our study evaluated the actual role of these metabolic disorders. Previous reports have documented the close connections between T2DM and disease recurrence and progression to muscle-invasive BC, 28 but have not ruled out the influence of other metabolic disorders. Our research addressed this important knowledge gap that patients with hyperglycemia alone have a higher readmission risk. The proposed mechanisms were that insulin, through activation of insulin-like growth factor-1 receptor, triggered downstream pathways with mitosis and transformational activity. 29 Diabetes also contributed to mitochondrial dysfunction, which could promote oxidative stress and result in impaired DNA repair 30 and a permanent proinflammatory state. 20 Cantiello et al. 31 showed that hypertension could increase the risk of higher pathological stage as well as lymph vascular invasion and lymph node metastasis. In Tai’s study, investigators reported an insignificant correlation between hypertension and BC recurrence, 32 but the underlying mechanisms of this effect were not well elucidated. Previous studies have not found that dyslipidemia was adverse in BC prognosis, which was consistent with our results. Although we found that the relationship between metabolic disorders and BC readmission was complex, we extended the previous knowledge. In addition, further research is needed to identify mechanisms by which hypertension leads to BC recurrence. Longer cohort studies are required to determine the effect of hyperlipidemia on BC recurrence.
To our knowledge, no study has investigated the association between metabolically defined obesity and the risk of BC readmission. Our study had several unique strengths. First, the research on obesity and BC prognosis was mostly on individual institutions in the past. The readmission data obtained from individual institution studies would grossly underestimate the actual readmission rates. Current studies based on national populations were free from the limitations mentioned above. Second, obesity phenotype classification could compensate for the limitations of using BMI alone to assess obesity, metabolically defined obesity can serve as a model for mechanistic studies regarding obesity and obesity-associated diseases through the identification of characteristic populations. Finally, we adjusted for important confounders to exclude the impact of comorbidities and carried out subgroup analysis to evaluate the impact of age and surgery.
Nevertheless, our study had several limitations. First, the NRD datasets are year-based and cannot be linked, excluding out-of-hospital mortality, 15 so the study population was followed for half of the year. Second, we utilized diagnosis codes to determine disease; sometimes imprecise coding could lead to potential misclassification. Third, the database does not include clinical information, such as disease stage, tumor grade and urothelial variants, 33 but we considered the effect of surgery on readmission. Finally, there is a lack of medication information. Several drugs used to treat T2DM may be associated with anticancer effects. 34 A multicenter study has shown that statin use was independently associated with a lower risk of BC recurrence. 35 Further research is needed to consider the beneficial or adverse effects of drugs. However, our study represented a cohort from 28 USA states, and our results could be considered reliable due to the large-sized nationwide study population.
Conclusion
In conclusion, obesity with metabolic abnormalities and metabolic abnormalities alone were associated with higher readmission risks in patients with BC. Age and surgical history modified the relationship between metabolically defined obesity and the risk of readmission. Further analysis also showed that the risk of readmission was directly proportional to the increased metabolic volumes and the specific metabolic disorders. We also found increased length of stay for readmission in patients with obesity and metabolic abnormalities. Future studies will focus on the early identification of higher-risk subgroups for BC readmission, and then a range of interventions will be tailored and improved, especially in older patients.
Supplemental Material
sj-docx-1-tau-10.1177_17562872231213720 – Supplemental material for Association of obesity and different metabolic status with prognosis in patients with bladder cancer: a retrospective cohort study
Supplemental material, sj-docx-1-tau-10.1177_17562872231213720 for Association of obesity and different metabolic status with prognosis in patients with bladder cancer: a retrospective cohort study by Yingchun Dong, Yiping Cheng, Honglin Guo, Jiaxing Sun, Junming Han, Fang Zhong, Qihang Li, Dawei Wang, Wenbin Chen, Xiude Fan and Jiajun Zhao in Therapeutic Advances in Urology
Footnotes
References
Supplementary Material
Please find the following supplemental material available below.
For Open Access articles published under a Creative Commons License, all supplemental material carries the same license as the article it is associated with.
For non-Open Access articles published, all supplemental material carries a non-exclusive license, and permission requests for re-use of supplemental material or any part of supplemental material shall be sent directly to the copyright owner as specified in the copyright notice associated with the article.