
Abstract
Objectives:
To evaluate the role of preoperative abdominal straining in predicting de novo overactive bladder (OAB) and voiding dysfunction in female patients undergoing suburethral taping by trans-obturator approach (TVT-O) for uncomplicated stress urinary incontinence (SUI).
Methods:
Data from patients who underwent TVT-O surgery for SUI were retrospectively analyzed. Inclusion criteria included: history of pure SUI. Exclusion criteria included previous surgery for urinary incontinence, pelvic radiation, pelvic surgery within the last 3 months, and anterior or apical pelvic organ prolapse (POP) ⩾ +1 cm. Voiding dysfunction has been defined through symptoms and or urodynamics (UDS) signs. Accordingly, patients were divided into group A and group B according to the presence of abdominal straining during UDS. Patients were observed clinically and with UDS at a 3-year follow-up.
Results:
A total of 192 patients underwent TVT-O surgery for uncomplicated SUI. Preoperative abdominal straining was identified in 60/192 patients (Group A: 31.2% vs Group B: 68.8%). Qmax was not different in the two groups (Group A: 19.5 vs Group B: 20.5 mL/s, p = 0.76). Demographics was similar for the two groups regarding age, parity. At 3-year follow-up, voiding dysfunction was reported in Group A: 9 and Group B: 8 patients (p = 0.056), de novo OAB was significantly reported in Group A: 23 and Group B: 26 patients (p = 0.007).
Conclusion:
Preoperative abdominal straining was found to be related to a significant incidence of de novo OAB. A significant correlation was not assessed for postoperative voiding dysfunction. Further studies may better define the impact of preoperative abdominal straining.
Keywords
Introduction
Sub-urethral sling procedures for stress urinary incontinence (SUI) in female patients have been largely accepted as a valid therapeutic option; however, they have been proved to be affected by detrusor overactivity (DO) in 1.7–42.4% of cases 1 and by overactive bladder (OAB) syndrome in 6–12% of cases. 2
The role of urodynamics (UDS) before surgery for SUI has been widely debated over the last years. In 2009, the non-inferiority ValUE trial by Nager et al. revealed that ‘uncomplicated’ patients (namely, patients affected with pure SUI) may not benefit of preoperative UDS evaluation, since clinical outcome at 1 year after surgery did not show significant differences between patients who underwent preoperative UDS, if compared to patients who underwent only physical examination.3,4 On the other hand, it was noted that ‘uncomplicated’ patients account for a minority of patients complaining with SUI, thus UDS role still remains under debate.5 –7
Accordingly, the potential role of preoperative factors able to predict clinical outcome after surgery has been investigated.8,9 In particular, Lee et al. described a potential implication of pre-existing intrinsic sphincter deficiency (ISD) and DO on postoperative de novo urgency and urge urinary incontinence (UUI). 9 A clinical picture consisting of older age and mixed urinary incontinence with prevalent UUI was identified as at increased risk of postoperative de novo OAB. 2
Therefore, the aim of this study was to evaluate the potential role of abdominal straining at preoperative UDS in predicting de novo OAB and voiding dysfunction in female patients undergoing suburethral taping by trans-obturator approach (tension-free vaginal tape-obturator, TVT-O) for uncomplicated SUI.
Patients and methods
All consecutive women referred to a single urogynecology unit from 2013 to 2015 in order to undergo TVT-O for uncomplicated SUI were retrospectively analyzed. Patients categorization as ‘uncomplicated’ was performed according to ValUE trial.3,4
Inclusion criteria were a history of pure SUI without voiding dysfunction, DO or OAB.
Exclusion criteria were:
DO or OAB previously diagnosed,
Neurological diseases,
Pelvic radiation,
Previous surgery for urinary incontinence,
Any other pelvic surgery within the previous 3 months,
Anterior or apical pelvic organ prolapse (POP) greater than 1 cm.
All patients underwent an office-based clinical evaluation before treatment and during the postoperative follow-up every 6 months; a thorough re-evaluation has been performed at 3 years follow-up to define the long-term outcomes. Clinical evaluation included medical history, physical examination, frequency–volume chart, and urine analysis. POP was assessed in the lithotomic position, with the patient exerting a maximal Valsalva maneuver, and was described according to the Pelvic Organ Prolapse Quantification system. 10
All women were studied with UDS before and after treatment, using a standardized protocol in accordance with the Good Urodynamic Practices Guidelines of the International Continence Society (ICS). 11 Each woman was asked to attend for UDS with a comfortably full bladder. Uroflowmetry was performed with the woman voiding in private and recorded on a gravimetric flowmeter. Cystometry was performed with the woman supine: her bladder was filled through a 10 F filling catheter, and two fluid-filled 4.5 F catheter were used to measure the intravesical (vesical catheter) and abdominal (rectal catheter) pressures. The bladder was filled with room temperature saline at 50 mL/minute. The filling catheter was removed when the patient developed a strong desire to void or 500 mL had been infused into the bladder. Provocative maneuvers were employed with the woman standing, asking her to cough once, three, and five times with maximal effort, to listen to running water, and to wash her hands in cold water. Finally, she was seated for a pressure-flow study that was performed in private, and the postvoid residual was measured using ultrasound scan imaging. All women were examined by two trained urogynecologists. All procedures and all definitions conform to those of the ICS.10,12
All the women included in this study were divided into two groups: women who experienced abdominal straining during micturition (group A) and women who did not (group B).
According to the ICS definition, OAB syndrome was defined as a clinical condition of urinary urgency, usually accompanied by frequency and nocturia, with or without urgency urinary incontinence, in the absence of urinary tract infection (UTI) or other obvious pathology. 12 De novo DO has been reported as a secondary outcome.
Symptoms were defined by hesitancy, slow stream, intermittency, straining to void, spraying of urinary stream, feeling of incomplete emptying, need to immediately re-void, postmicturition leakage, position-dependent micturition, dysuria following the International Urogynecological Association (IUGA)/ICS joint report on the terminology. 12 UDS signs included maximum flow rate (Qmax) less than 15 mL/s, maximum detrusor pressure [Pdetmax] greater than 60 cmH20 and postvoid residual volume (PVR) greater than 100 mL (measured by urodynamic bladder catheter).
Post-TVT-O urinary retention (UR) was defined as the complaint of the inability to pass urine despite persistent effort 12 with the need of intermittent bladder catheterization or permanent bladder catheterization for at least 24 hours, with or without sling revision, during the whole follow-up.
The patient global impression of improvement (PGI-I) questionnaire was used to rate the response to the TVT-O treatment in the two groups as a subjective parameter of efficacy. 13
Anonymized data were extracted from medical reports. Ethical committee approval was not required as this was a retrospective study based on anonymized data only. The authors were granted access to anonymized data only; anonymization was performed at the center where patients had been evaluated and treated (Varese) by one of the physicians who treated them and none of the authors were involved in the anonymisation process. All patients gave written consent for the use of their anonymized data for scientific research.
Results
One hundred and ninety-two female patients underwent TVT-O surgery for uncomplicated SUI. Preoperative abdominal straining was identified in 60/192 patients namely called group A: 31.2% while it was not shown in the other 132 patients, Group B: 68.8%. A sample preoperative UDS trace showing abdominal strain is reported in Figure 1. Demographic characteristics of the included patients are summarized in Table 1. Age, parity, and body mass index (BMI) were similar in the two groups.
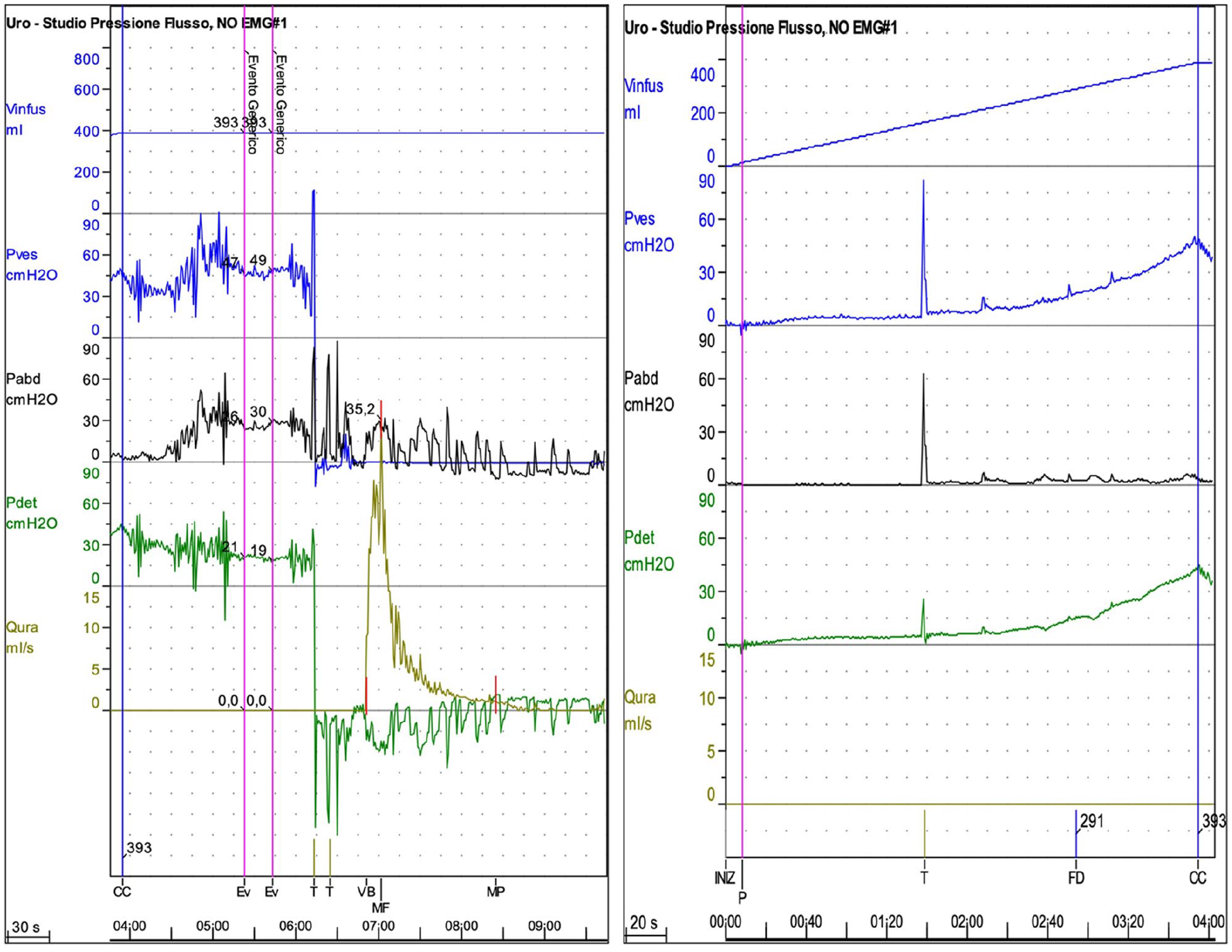
Preoperative urodynamics (UDS) traces from patients complaining with abdominal straining.
Baseline characteristics.

Data are expressed as mean and percentage (%) or mean and range (range).
BMI, body mass index.
Preoperative Qmax was not different in the two groups (group A: 19.5 mL/s vs group B: 20.5 mL/s, p = 0.76).
At a 3-year follow-up, we evaluated the presence of voiding dysfunction that was reported in nine patients from group A and in eight patients from group B (15% versus 6%, p = 0.056). There was no significant difference in developing post TVT-O voiding dysfunctions in women presenting with or without abdominal straining before surgery. The UR cases were not statistically significant (group A: 4 vs group B: 2; p = 0.7).
On the other hand, de novo OAB was reported in 23 patients from group A and 26 patients from group B (38% versus 19.6%, p = 0.007). At 3 years follow-up, patients with de novo OAB reported a worse PGI-I. Specifically, 40/49 (81%) patients with de novo OAB reported a PGI-I > 3 (‘no change’ to ‘very much worse’); interestingly, 26/40 patients with de novo OAB and PGI-I > 3 were in group A and 14/40 in group B. On the other hand, patients not suffering de novo OAB had a PGI-I > 3 in only 21/143 patients (14.6%) reporting a higher grade of satisfaction. There was significant difference in the PGI-I between the groups.
Among patients presenting with de novo OAB, 18/23 from group A (78.2%) and 23/26 from group B (88.5%) showed also de novo DO. Comprehensive UDS data are reported in Table 2. Operative data are reported in Table 3.
Urodynamics (UDS) data.

Data are expressed as median (range).
CC, cystometric capacity; FDTV, first desire to void; I-OpenP, intravescical opening pressure; PDetMax, Maximum Detrusor pressure; PDetQMax, Detrusor Pressure at Maximum Flow; Qmax, Maximum Flow.
Operative data.

Data are expressed as absolute number (%) or median (interquartile range).
Discussion
The ideal outcome of SUI surgery is to restore perfect continence with minimal morbidity and significant improvement in quality of life. TVT-O has been largely demonstrated as a highly effective and safe option for the treatment of female pure SUI. 14 However, the placement of mid-urethral slings has been associated with a number of perioperative and postoperative complications, including voiding dysfunctions, urinary retention, and de novo OAB symptoms. 15
Regarding the postoperative voiding dysfunction, Stanford et al. reported an incidence of 16.3%. 1 Ripperda et al. reported that postoperative voiding dysfunction could be due to a preoperative ‘abnormal voiding pattern’ (odds ratio (OR) = 1.79 (1.06–3)) defined as a combination of abdominal/Valsalva void and mixed and mixed voiding pattern. 15 Furthermore, Khayyami et al. highlighted that postvoid residual urine (PVR) alone cannot exclude preoperative voiding dysfunctions underlining the role of flow measurements before surgery. 16 Although in an uncomplicated population of women with SUI, it is not demonstrated that preoperative UDS can improve the outcome of continence surgery, UDS may provide additional information when the simple office-based evaluation is not enough to identify some relevant diagnosis such as voiding dysfunction in absence of a significant post voiding residual urine, or an ‘asymptomatic’ DO, or a urethral sphincter deficiency. 7
As of de novo OAB, it is a known complication of mid-urethral sling surgery for the treatment of SUI. A meta-analysis performed by Pergialiotis et al. reported that differences in the incidence of de novo OAB following the use of different types of mid-urethral sling remain relatively unknown without any significant differences (p = 0.58). 17 The incidence of de novo OAB for TVT-O was 11.2%, aligned with the one reported by Marcelissen et al. ranging from 4.1% (6- to 12-month follow-up) to 15% at 10-year follow-up. 2 DO has been also described as a de novo sling-related complication with an incidence of 15.4%. 1
Although the endpoint of our study was to evaluate de novo OAB, as further information, we recorded a high incidence of de novo DO among patients presenting with de novo OAB (78.2% in group A and 88.5% in group B, respectively). This result should be taken into account considering Giarenis et al. who reported that women with DO experience more significant impairment to their quality of life and have a greater degree of bladder dysfunction in terms of higher urgency episode frequency and larger maximum and mean urge ratings. 18
Our study evaluated the potential role of abdominal straining at preoperative UDS in predicting de novo OAB and voiding dysfunction in female patients undergoing TVT-O with a hypothesis-generating and exploratory purpose. Our data showed a significant relationship between abdominal straining and de novo OAB leading to consider them as able to overlap mild forms of voiding dysfunctions without high PVR, although a significant correlation was not assessed (p = 0.056), probably due to our small sample size. Furthermore, patients with de novo OAB (significantly associated with the preoperative abdominal straining) reported a significant worsening of the PGI-I questionnaire at 3-years follow-up underling the important role of urodynamic preoperative investigation. Thus, the role of preoperative abdominal straining is a new urodynamic feature that should be considered once investigating a patient undergoing SUI surgery. It may ameliorate the patient counseling leading to alternative therapeutic options such as rehabilitation prior to surgery in uncomplicated SUI patients. Hence, several papers highlighted the role of UDS in changing and improving the clinical and surgical management of women with SUI and OAB and the recent urodynamic recommendations of the Italian Society of Urodynamics in the female population suggest that UDS may be performed in complicated patients with both symptoms and physical findings of SUI before invasive treatments or in uncomplicated patients, when UDS may help for counseling.19 –21
We still need to consider that OAB and urinary incontinence have a lifelong dynamic progression of symptoms (e.g. among women with OAB without UUI 28% reported OAB with UUI 16 years later) and that although symptom severity progresses dynamically, for many patients’ symptoms also persist over long periods. 22
To date, there are no randomized trials specifically including de novo OAB as one of the primary outcome measures after mid-urethral slings nor trials investigating the role between abdominal straining as its possible underlying cause. Several possible limitations should be considered in the assessment of this study. Although a prospective, well-powered and randomized clinical trial would have been more helpful in the comprehension of the role of abdominal straining, we tried to carry out a hypothesis-generating retrospective analysis in order to explore its possible relationship with the incidence of de novo OAB and voiding dysfunctions. This implies that our results cannot lead to a confirmatory cause-effect relationship that needs a hypothesis-testing trial. However, the 3-year follow-up provides information about long-term de novo OAB and voiding dysfunctions in uncomplicated SUI patients.
Conclusion
Preoperative abdominal straining was found to be related with an increased incidence risk of de novo OAB.
Although the role of invasive UDS seems relevant in providing surgeons and patients with more information on the potential postoperative development of de novo OAB and de novo DO, further best-powered studies are needed to better define the impact of preoperative abdominal straining on OAB and voiding dysfunctions in women undergoing TVT-O.
Footnotes
Author contributions
Valerio Iacovelli: data analysis, paper writing and editing
Maurizio Serati: conceived and designed the analysis, paper editing
Daniele Bianchi: data collection and analysis, paper writing and editing
Andrea Braga: data collection and analysis
Andrea Turbanti: data collection and analysis
Enrico Finazzi Agrò: conceived and designed the analysis, paper editing
Conflict of interest statement
The authors have no potential conflicts of interest with respect to the research, authorship, and/or publication of this article.
Funding
The authors received no financial support for the research, authorship, and/or publication of this article.