
Abstract

Keywords
Introduction
The 2024 International Functional and Reconstructive Urology Update (IFRUU) Neurology & Overactive Bladder (OAB) sessions provided integrated insights into neurogenic lower urinary tract dysfunction (NLUTD), transitional urologic care, and contemporary third-line OAB therapies. These presentations advanced the evolving framework of functional urology by promoting risk stratification, diagnostic clarity, and individualized treatment planning.
The American Urological Association (AUA) guidelines have redefined “neurogenic bladder” as NLUTD to encompass both storage and voiding dysfunction with an underlying neurological diagnosis. 1 A risk-stratified model now guides evaluation and management, encouraging focused testing for high-risk patients while minimizing unnecessary interventions for those at lower risk.1,2 In parallel, pediatric to adult transitional care, in urology, has emerged as a critical component for patients with congenital or early-onset NLUTD, requiring coordinated, multidisciplinary engagement.
OAB has traditionally been treated with behavioral modification and oral medications.3,4 However, these first- and second-line therapies have limited durability, in some, and are often poorly tolerated.5,6 Advances in sacral neuromodulation, botulinum toxin injections, and tibial nerve stimulation are important developments in the third-line management for refractory OAB, showing improved efficacy and patient satisfaction. Data presented at the IFRUU emphasized ongoing innovations, including implantable tibial stimulators and noninvasive modalities, reflecting a broader movement toward customizable, evidence-based care.
Methods
These proceedings summarize nine expert-led presentations:
Dr. Stephen Kraus—AUA Guidelines for Neurogenic Lower Urinary Tract Dysfunction
Dr. Daniel Wood—Pediatric to Adult Urology Transition
Dr. Stephen Kraus—Urodynamics 101. The speakers outlined clinical practice updates, guideline-driven risk stratification models, transitional care structures, and interpretive frameworks for urodynamic studies
Dr. Janine Oliver—Noninvasive OAB Therapies
Dr. Matthew Ercolani—Axonics® Sacral Nerve Modulation
Dr. Christopher Wolter—InterStim® Neuromodulation
Dr. Lenaine Westney—Botox for Post-Prostatectomy OAB
Dr. Suzette Sutherland—Revi® Implantable Tibial Nerve Stimulator (OASIS Trial)
Dr. Jason Kim—eCoin® Implantable Tibial Nerve Stimulation
Each speaker provided comprehensive clinical updates, including therapeutic efficacy, safety data, procedural details, patient selection criteria, and future research directions.
Results
Dr. Kraus introduced the updated AUA guidelines, which recommend classifying patients by neurologic diagnosis, bladder function, and imaging findings. Low-risk patients, such as those post-stroke with preserved bladder emptying, may avoid invasive testing. In contrast, high-risk patients (e.g., with spinal cord injury or neurogenic detrusor overactivity) warrant detailed urodynamics, renal imaging, and long-term surveillance. Management should escalate appropriately, avoiding overtreatment (e.g., antibiotics for asymptomatic bacteriuria) and emphasizing patient-centered decision-making.1,2 These updated recommendations are consistent with newer international consensus statements, such as the recently published NEUROGED guidelines.7,8
Dr. Wood addressed pediatric to adult transitional care in patients with congenital or early-onset NLUTD. He emphasized that transition is a longitudinal, multidisciplinary process that includes attention to renal function, continence, sexual function, sexual health, and fertility. One study reported that up to 50% of patients with corrected cloacal anomalies develop renal impairment, and 17% progress to ESRD. 9 Early and coordinated care can prevent complications—fewer than 1% of patients, with spina bifida, in one single-center cohort managed early progressed to advanced renal disease. 10
Returning to diagnostics, Dr. Kraus reviewed the principles of urodynamic testing using the “3 Cs and 2 Ss” framework—capacity, compliance, competence, sensation, and stability—to interpret bladder behavior. He emphasized the selective use of urodynamics based on clinical context.
The OAB sessions transitioned to third-line therapies and noninvasive options (see Figure 1). Dr. Oliver discussed transcutaneous tibial neurostimulation (TTNS), magnetic stimulation, and high-intensity focused electromagnetic (HIFEM) therapy. 11 TTNS was shown in a 2022 systematic review to improve urgency and frequency, although not urinary incontinence. 12 A 2022 trial, magnetic stimulation plus bladder training improved nocturia, pad use, and quality of life over bladder training alone. 13 HIFEM (e.g., EMSELLA™ chair – BTL Industries, Marlborough, MA, USA) demonstrated benefit in urinary incontinence symptoms in a non-randomized study involving 95 premenopausal women. 14
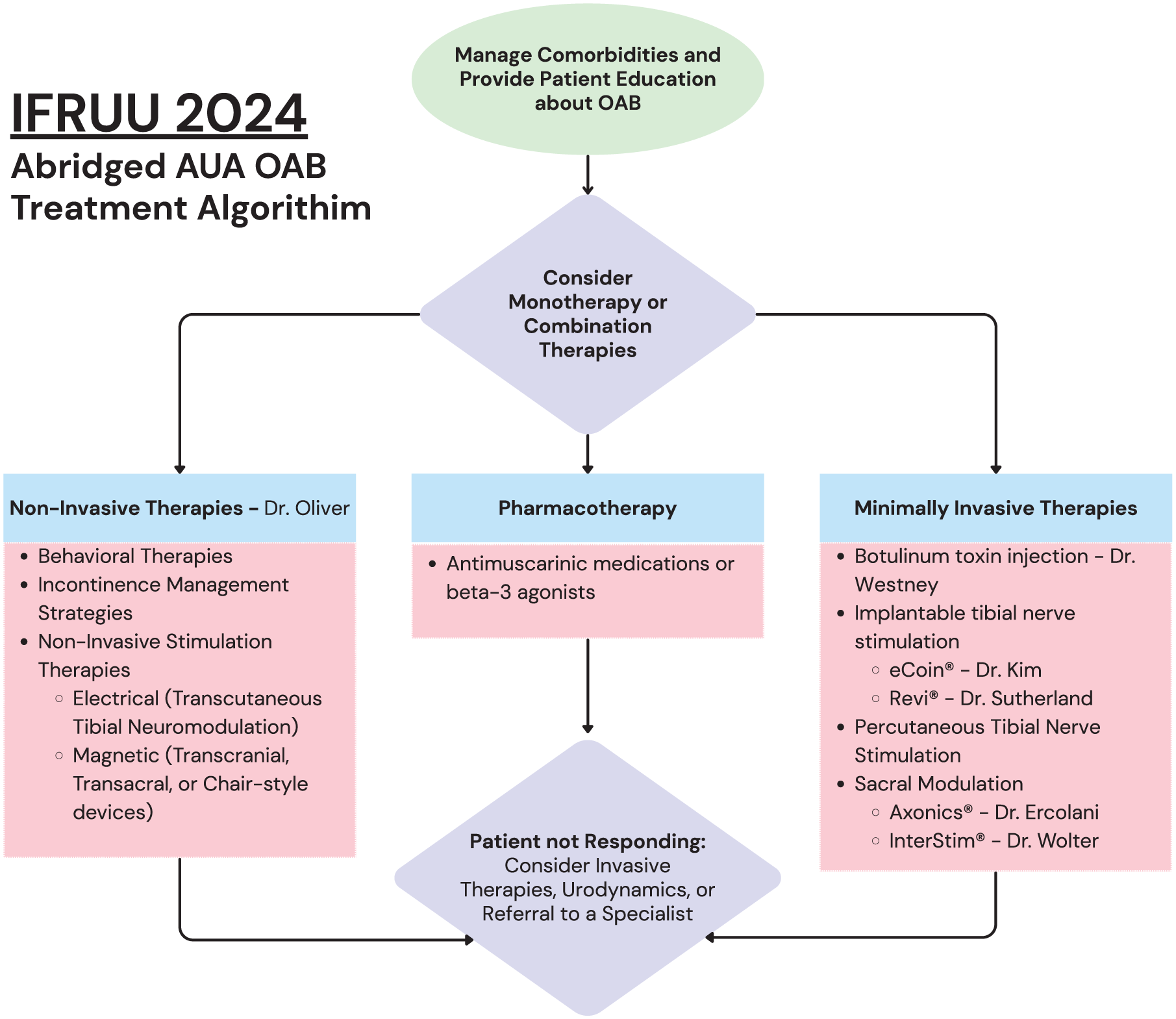
Abridged AUA OAB treatment algorithm focused on therapy considerations and highlighting physicians who presented on therapy options at the IFRUU 2024.
Drs. Ercolani and Wolter presented on Axonics® (Axonics, Inc., Irvine, CA, USA) and InterStim®, (Medtronic, Minneapolis, MN, USA) both targeting S3 nerve roots to restore bladder-brain signaling. Axonics® features a rechargeable system and reported 93% success in reducing urgency incontinence by ⩾50%. InterStim® offers established efficacy, newer MRI-safe models, and streamlined procedures.
Focusing on male patients with post-prostatectomy bladder dysfunction, Dr. Westney highlighted the complex role of botulinum toxin, especially after radiation. A 1998 study showed nearly one-third of prostate cancer patients develop detrusor dysfunction post-treatment. 15 While botulinum toxin shows promise in radiated and BCG-treated bladders, responses remain variable due to compromised compliance and vascularity. She also noted the exclusion of radiated patients from many PTNS trials, underscoring the need for tailored studies.
Dr. Sutherland introduced Revi® (BlueWind Medical Ltd., Salt Lake City, UT, USA), an implantable tibial nerve stimulator paired with an external controller. In the OASIS trial, 82% of participants achieved treatment response, with strong safety and patient satisfaction data over 12 months. 16 Revi’s customizable, maintenance-light design offers promise for long-term OAB management.
Dr. Kim concluded with eCoin® (Valencia Technologies, Valencia, CA, USA), a fully implantable, hands-free tibial nerve stimulator. Implanted subfascially, in a brief office-based procedure, eCoin® achieved ⩾50% UUI symptom reduction in 75% of patients at 48 weeks. Additional data showed 49% achieved ⩾75% improvement, and 23% achieved complete resolution. 17 With over 1000 commercial implants and a 0.4% explant rate, eCoin® offers a low-maintenance alternative to traditional neuromodulation. Patients cited high satisfaction due to insufficient external equipment, recharging, or programming. Comparative patient surveys reinforce its appeal for those prioritizing autonomy. 18
Conclusion
The IFRUU 2024 Neurology & OAB session highlighted a paradigm shift in functional urology: from standardized algorithms to precision medicine. For NLUTD, this means adopting risk-based diagnostics and long-term adult care for childhood conditions. For refractory OAB, the expanding landscape of third-line therapies—both invasive and noninvasive—underscores the value of tailoring interventions to individual patient needs and preferences. As innovations in diagnostics and treatment continue to evolve, the emphasis remains on evidence-based, patient-centered care.