
Abstract
Aims:
To analyze the outcomes of urethral re-bulking in the treatment of female stress urinary incontinence.
Materials and Methods:
We performed a multicenter observational retrospective study, which included all consecutive patients treated with urethral re-bulking for the treatment of persistent stress or mixed urinary incontinence after a previous urethral bulking. Objective outcomes were evaluated with the 24 h pad-test, while PGI-I questionnaires were administered to evaluate subjective outcomes. Clinical outcomes were assessed before re-bulking procedure and at last follow-up. Mann–Whitney’s U test was used for subgroup analysis. Shapiro-Wilk’s tests were used as normality tests.
Results:
In total, 62 patients who underwent urethral re-bulking between 2013 and 2020 in a multicenter setting were included. Most patients did not reach complete continence after the first procedure (n = 56) while the remainder reported recurrence of urinary incontinence after initial benefit. Median age at surgery was 66 (IQR: 55-73). Median overall follow-up was 30 months (IQR: 24-41). Median time occurred between the first procedure and reintervention was 12 months (IQR: 7-27). Bulking agents for the re-bulking procedures were bulkamid(n = 56), macroplastique(n = 4), and Prolastic(n = 2). A statistically significant reduction of median 24 h pad test from 100 g(IQR: 40-200) to 35 g(IQR: 0-120) was observed (p = 0.003). Dry rate after rebulking was 36.6%, while 85.4% patients declared themselves ‘very much improved’ or ‘much improved’ (PGI-I 1-2). Very few low-grade complications were observed (n = 4). A single case of major complication occurred.
Conclusions:
Urethral re-bulking can be an effective technique for the treatment of stress urinary incontinence refractory to a previous urethral bulking and can determine a cumulative benefit after the first procedure.
Introduction
Urethral bulking (UB) is a minimally invasive technique for the treatment of female stress and mixed urinary incontinence with dry rates ranging from 16% up to 50% 1 and subjective satisfaction rates up to 80%.1–3 The most appealing features both for patients and clinicians are the extreme simplicity of the surgical procedure and the very low incidence of peri-operative and long-term complications, which include self-limiting hematuria, temporary urinary retention and uncomplicated urinary tract infections. 2
Nevertheless, when compared to different anti-incontinence techniques such as mid-urethral slings (MUS), UB has shown inferior continence results and was therefore considered a second choice in the past years. 3 Recent concern regarding mesh surgery has raised new interest in UB as a possible first-line technique. 4 However, the relatively inferior functional results of UB compared to MUS still limit the applicability of the technique, which is usually proposed to older comorbid patients or to patients who privilege a minimally invasive approach. 5
The aim of this work is to assess the functional outcomes and the safety profile of urethral re-bulking after the failure of a prior urethral bulking.
Materials and methods
We performed a retrospective, observational, multicentric study. After approval by the Institutional Ethical Committee (Intercompany Ethics Committee AOU Città della Salute e della Scienza di Torino, ID 00371/2020), all consecutive patients treated with urethral re-bulking after failure of a previous urethral bulking in a multicenter setting were enrolled. Treatment failure was defined both as lack of efficacy of the primary UB treatment and as progressive loss of efficacy after an initial good result. We included female patients affected either by genuine stress urinary incontinence or mixed incontinence. All enrolled patients had undergone a primary bulking treatment, without achieving a satisfactory continence result or with postoperative recurrence of SUI. In our clinical practice, all these patients are offered a secondary treatment for SUI; patients are counseled about indications, results and possible complications of both a re-bulking treatment and a MUS implant. We included in this study all patients choosing a re-bulking procedure after an extensive counseling.
As this is a retrospective study, any effort to avoid possible bias could be done. Nevertheless, we chose strict exclusion criteria in order to minimize the confounding factors. Exclusion criteria were neurogenic bladder, male gender, previous major bladder surgery and abnormal intra-operative cystoscopy (such as bladder diverticula, undirect signs of bladder outlet obstruction, vesical stones, or tumor).
Data from patient’s clinical records were collected in a dedicated database. Every patient underwent accurate anamnesis, physical examination and urodynamic evaluation before surgery. Physical examination included stress test, POP-Q test, perineal US scan or Q-tip test to evaluate urethral mobility. Urodynamic exams were performed according to Good Urodynamic Practice 6 as recommended by International Continence Society (ICS). The operative procedure was performed under local anesthesia after antibiotic prophylaxis according to local institutional guidelines. A dedicated cystoscope with 0-degree optic was employed and bulking agents were injected in the proximal urethra under bladder neck until a visually satisfying bulking effect was reached. Patients were dismissed the same day of the procedure. Outcomes were evaluated before re-bulking surgery and at last follow-up. Primary outcome was the result of the procedure on urinary incontinence. As secondary outcome the complications of the procedure were assessed. Continence outcomes were evaluated with a 24 hour pad test and Patient’s Global Impression of Improvement questionnaire (PGI-I). 7 Methods, definitions, and units used in the present study are compliant to the standards recommended by the International Continence Society, except where specifically noted. 6
Data were indicated as mean (SD) or median (IQR) depending on the variable’s distribution, which was assessed via Shaphiro-Wilk’s tests. In the statistical analysis, the outcomes of UB and urethral re-bulking were treated as independent groups and Mann–Whitney’s U tests were used for the comparison between groups. P < = 0.05 defined statistical significance. Statistical analysis was performed with IBM® SPSS® Statistics software.
Results
A total of, 73 patients who underwent primary UB between 2009 and 2019 and subsequent urethral re-bulking between 2013 and 2020 were identified. In all, 62 patients met the inclusion criteria and therefore were included in the study. Patient’s characteristics at baseline are enlisted in Table 1. Several patients had undergone previous pelvic surgery (40.3%) or anti-incontinence surgery (37.1%). The detailed list of previous interventions is reported in Table 2. Most patients did not reach complete continence after the first procedure (n = 56), while 6 reported recurrence of urinary incontinence after 6 months (n = 2), 12 months (n = 2) or more than 12 months (n = 2). Median age at surgery was 66 (IQR: 55-73). Median overall follow-up was 30 months (IQR: 24-41) while median time occurred between the first procedure and reintervention was 12 months (IQR: 7-27). Median follow-up after re-bulking was 9 months (IQR: 6-12). The bulking agents employed for re-bulking procedures were Bulkamid® (n = 56); Macroplastique® (n = 4), and Urolastic® (n = 2). After the re-bulking procedure, 24 h pad test decreased from 100 g (IQR: 40-200) to 35 g (IQR: 0-120), p = 0.003. Dry rate after re-bulking was 36.6%, while 85.4% patients declared themselves ‘very much improved’ or ‘much improved’ (PGI-I: 1-2) and only 14.6% declared themselves ‘little improved’ or ‘not improved’ (PGI-I: 3-4). Complications included transient post-operative urinary retention (n = 4) which spontaneously resolved with a brief period of self clean intermittent catheterization and which was classified as Clavien-Dindo I. One case of urethra-vaginal fistula occurred after urethral re-bulking with Urolastic, which required surgical intervention of fistulectomy and urethral repair (Clavien-Dindo IIIa).
Baseline characteristics of the study population.
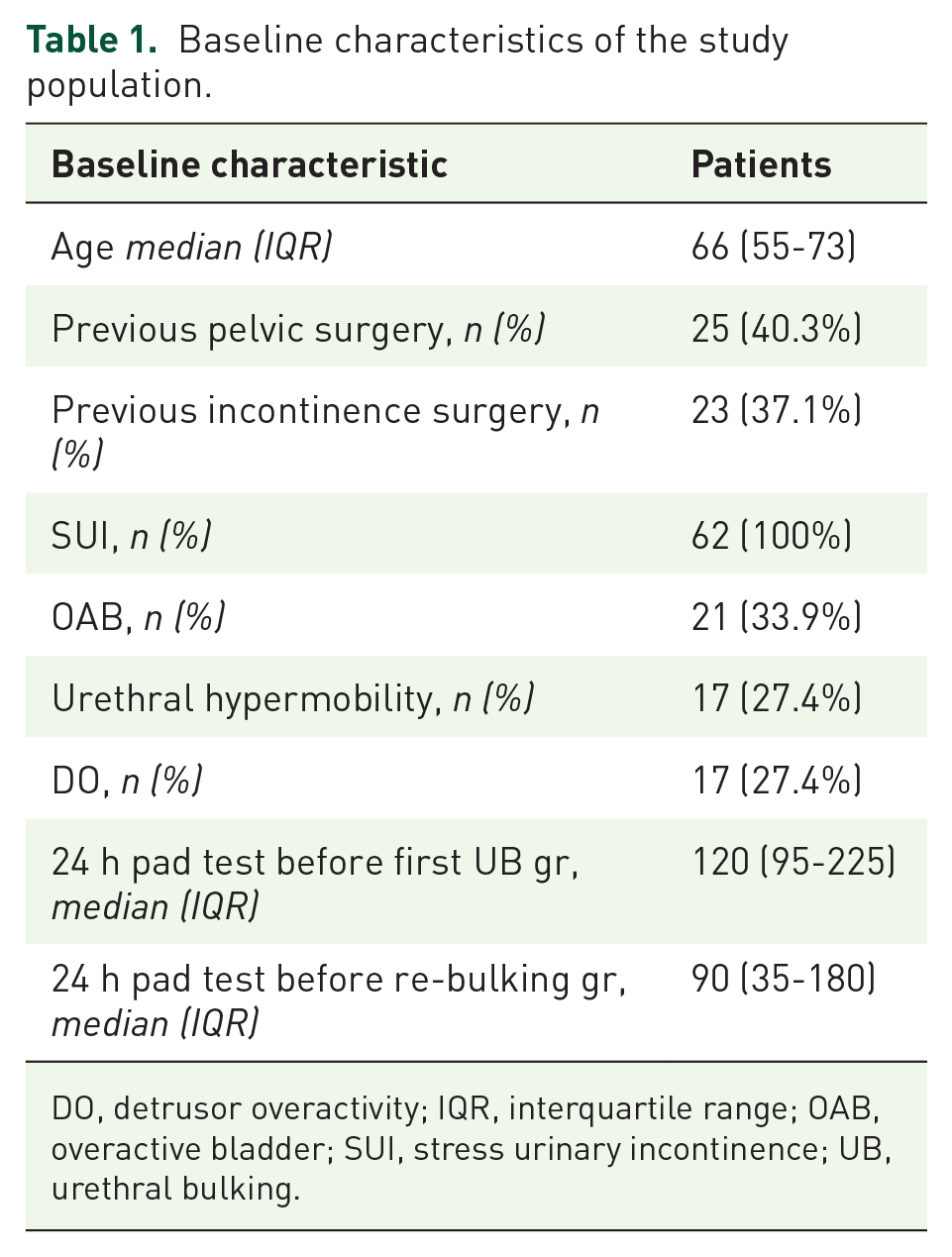
DO, detrusor overactivity; IQR, interquartile range; OAB, overactive bladder; SUI, stress urinary incontinence; UB, urethral bulking.
Previous anti-incontinence surgery and previous pelvic surgery.

ACT, adjustable continence therapy; SNM, sacral neuro modulation; TOT, Trans obturator tape; TVT, tension-free vaginal tape.
Discussion
The treatment of recurrent urinary incontinence in female patients after anti-incontinence surgery is still controversial and scarce evidence is available. Urethral bulking is often regarded as salvage therapy after the failure of MUS with a cure rate that can reach 80%, associated with low complications. 8 Surgical options such as Burch’s vaginal suspension, autologous slings or artificial urinary sphincter implantation can also be considered, although remains unclear whether surgical or mini-invasive approach should be preferred. 9 On the contrary, a surgical treatment for recurrent urinary incontinence after UB would be hardly accepted by patients who had already chosen a mini-invasive approach. Urethral re-bulking can be an effective solution in the treatment of these patients and can give good results maintaining the mini-invasiveness of the procedure.
Some low-evidence works that compare the outcomes of urethral bulking in naïve patients and in patients with recurrent urinary incontinence, confirm analogous outcomes in both groups. A recent study performed on a small cohort of patients reports a percentage of success of UB of 75% in the salvage group and 67% in naïve group with no statistically significant difference between groups. 10 The present study confirms comparable outcomes of urethral re-bulking and of UB performed on naïve patients, with a dry rate exceeding 36% and satisfaction rate over 85%.
Furthermore, our work underlined a favorable safety profile of urethral re-bulking, with low peri-operative complications (6% of complications classified as Clavien-Dindo I; 1.5% of complications classified as Clavien-Dindo IIIa). In the present series of cases only one major complication was observed, which was represented by a urethral fistula which required surgical repair. The bulking agent related to this complication was Urolastic®. According to the authors, the safety of UB should be considered individually, depending on the bulking agent which is used for the procedure. In fact, some recent reports regarding major complications after urethral bulking with Macroplastique® are available. 11 Also UB with Urolastic® was associated with a non-negligible rate of complications, such as migration of the bulking agent into bladder. 12 In the present study, the good safety outcomes could be influenced by the fact that most of re-bulking procedures were performed with Bulkamid® and only for a low number of procedures were performed with Macroplastique® or Urolastic®. In addition, in the naïve group most procedures were performed with Bulkamid® and no procedure was performed with Urolastic®. Therefore, the onset of one major complication in the re-treatment group should be referred probably to the bulking agent more than to the reiteration of UB itself. Prospective randomized studies conducted with a single bulking agent could help to validate the safety of re-bulking and to underline possible differences between bulking agents.
To the best of our knowledge, the present study is the first one assessing the outcomes of urethral re-bulking. Our work describes a mini-invasive, effective method to treat urinary incontinence refractory to UB. Urethral re-bulking could improve the outcomes of UB with overall results comparable to more invasive procedures. Strengths of the present study are the relatively high number of patients enrolled and the use of validated questionnaires and of pad weight test for the evaluation of outcomes. The major limitation of the study is the inhomogeneity of bulking agents used for urethral re-bulking, along with the heterogeneity of the surgical techniques (given the multicentric design which involved several surgeons with different levels of expertise). Furthermore, a major weakness is the retrospective observational design of the study. Moreover, the present study is characterized by a relatively elderly population, with high prevalence of patients who were subjected to previous anti-incontinence surgery. These aspects could limit the generalizability of the data reported in the work. To overcome these major limitations, further prospective studies are advocated.
Conclusion
Urethral re-bulking can be a suitable option for the treatment of stress urinary incontinence refractory to a previous urethral bulking and can determine a cumulative benefit. Objective and subjective outcomes are comparable to the outcomes of urethral bulking on naïve patients. Any increase in complications was observed with the reiteration of the procedure, except for a single case of major complication.
Footnotes
Author contributions
Conflict of interest statement
All authors declare not to have any conflict of interest with regard to the topic of this paper.
Funding
The authors received no financial support for the research, authorship, and/or publication of this article.
Ethical approval
This study received the approval of the local Ethical Committee (Intercompany Ethics Committee AOU Città della Salute e della Scienza di Torino, ID 00371/2020). All patients signed an informed consent.