
Abstract
Background:
The artificial fluorinated group of compounds polyfluoroalkyl chemicals (PFCs) has been applied extensively in daily life for decades, and is present in food, drinking water, and indoor dust. The nephrotoxicity of PFCs has been widely studied for its characteristics of being mainly excreted through passing urine and affecting urodynamics. This work aimed to investigate the relationship between PFCs and the occurrence of urge urinary incontinence (UUI) in the United States (US) population.
Methods:
There were 3157 eligible female participants retrieved from the National Health and Nutrition Examination Survey (NHANES) between 2007 and 2014. A logistic regression model was used to examine the relationship between UUI and eight kinds of PFCs. The dose–response relationship was investigated through restricted cubic spline analysis in this retrospective study.
Results:
Of the 3157 eligible female participants, 913 self-reported a history of UUI. Total PFCs, perfluorohexane sulfonic acid (PFHS), 2-(N-methyl-perfluorooctane sulfonamido) acetate (MPAH), and perfluorononanoic acid (PFNA) correlated positively with the occurrence of UUI after adjusting for age, race, education, vigorous recreational activities, hypertension, diabetes, body mass index (BMI), creatinine, and estimated glomerular filtration rate (eGFR). Based on the results of sub-group analysis, the increasing tertiles contained odds ratios [OR; 95% confidence intervals (CI)] of 1.25 (95% CI, 1.03–1.51, p = 0.026) and 1.56 (95% CI, 1.29–1.89, p < 0.001) for total PFCs compared with the lowest tertile. The OR for PFHS, MPAH, and PFNA were 1.75, 1.71, and 1.41 respectively, in the highest tertile.
Conclusion:
This study investigated the relationship between PFCs and UUI in female and found total PFCs, PFHS, MPAH, and PFNA were positively correlated with the risk of UUI. The results will contribute to developing individualized treatment for female patients suffering UUI.
Keywords
Introduction
Urge urinary incontinence (UUI) is particularly characterized by involuntary loss (leakage) of urine associated with a sudden, compelling desire to pass urine that is difficult to delay. 1 Compare with stress urinary incontinence (SUI), UUI can have more detrimental impacts on an individual’s physical, mental, and social well-being. The incidence of UUI in women is much more frequent than in men. 2 Moreover, with increasing age, the prevalence of this disruptive disease ranges from 17% in women aged over 45 years to 27% in those older than 75 years in the United States (US). 3 UUI is also associated with an enormous economic burden from a societal perspective. During last 5 years, the estimated total cost of UUI in the US increased from $76.2 billion to $82.6 billion. 4 Risk factors for UUI include age, obesity, delivery mode, and, for women, postmenopausal status. 5 The incidence of UUI is also related to long-term smoking and chronic coughing. 6
Polyfluoroalkyl chemicals (PFCs) are a group of artificial fluorinated compounds that have been used widely in human life over the past decades, including in food packaging, clothing, and cosmetics. 7 According to previous reports, PFCs have been detected in food, drinking water, and indoor dust. Humans can be exposed to PFCs through those routes. 8 In the 2019 US National Biomonitoring Program, at least one type of PFC can be detected in every sample of blood. Moreover, because these chemicals are resistant to degradation, PFCs can bioaccumulate in food chains. 9 Along with growing evidence indicating that long-term exposure to PFCs cause adverse health concerns including kidney stones, 10 developmental toxicity, 11 and premature ovarian insufficiency, 12 more and more attention has been attracted to human exposure to PFCs. Thus, PFCs are considered as emerging anthropogenic pollutants worldwide.
Like other organic pollutants, PFCs are excreted mainly through passing urine. Many studies have suggested that PFCs are associated with nephrotoxicity, which may affect urodynamics. 13 The potential urodynamic impairment caused by exposure to PFCs has been a source of concern. However, the relationship between PFCs and the occurrence of UUI remains unclear. In this study, we aim to investigate whether the level of PFCs is associated with the occurrence of UUI in adults using data from the 2007–2014 National Health and Nutrition Examination Survey (NHANES).
Material and methods
Study population
The demographic data included in the study originates from NHANES. As a nationally representative survey, NHNES is conducted by the Centers for Disease Control and Prevention (CDC) every other year among the non-institutionalized US population. Study protocols of NHANES were approved by the Institutional Review Board of National Center for Health Statistics (NCHS) and participants’ consent was obtained during the survey process. Participants receive confidential questionnaires on socioeconomics, diet, and health, at home or at mobile examination centers.
In this study, we analyzed data from four consecutive NHANES 2-year survey cycles (2007–2008, 2009–2010, 2011–2012, 2013–2014), which including the questionnaires involving urinary incontinence type and frequency. We conducted the survey of UUI for the reason that UUI is more common in woman and the other kinds of UI (including SUI and mixed urinary incontinence) were not involved in this work. All the female participants aged 20 or older who responded to the survey questionnaire of “Kidney Conditions – Urology” were included in this cohort. There were 20,437 female participants from NHANES between 2007 and 2014. The exclusion criteria followed in this study were as follows: (1) with no incomplete UUI survey or unknown UUI; (2) with no PFCs data; (3) unknown BMI; (4) unknown creatinine (Figure 1).

Schematic flow diagram of exclusion criteria in this study.
PFC exposure and study variables
The levels of PFCs were the main predictors in this study, consisting of perfluorodecanoic acid (PFDE), perfluorohexane sulfonic acid (PFHS), 2-(N-methyl-perfluorooctane sulfonamido) acetate (MPAH), perfluorobutane sulfonate (PFBS), perfluoroheptanoic acid (PFHP), perfluorononanoic acid (PFNA), perfluoroundecanoic acid (PFUA), and perfluorododecanoic acid (PFDO). The quantitative investigation of PFCs in serum were determined by online solid phase extraction coupled to high performance liquid chromatography-turbo ionspray ionization-tandem mass spectrometry (online SPE-HPLC-TIS-MS/MS). For detection of PFCs, a volume of 50 μl serum was examined in a commercial column switching system after dilution with formic acid. This method could rapidly determine the concentration of PFCs with a limit of detection (LOD) of around 0.1 ng/ml. Detailed protocols for the detection of serum PFCs have been reported in a previous study. 14
The other variables analyzed in this study included age (<50 years and ⩾50 years), race (Non-Hispanic (white or black), Mexican American, Other Hispanic and Other), marital status (married and unmarried), education (less than high school, high school or equivalent, college or above and other), etc. In addition, recreational activities with two kinds of intensity (vigorous and moderate), hypertension, diabetes and body mass index (BMI, kg/m2; <25.0 and ⩾25.0) were included in this work as covariates. Simultaneously, the creatinine and estimated glomerular filtration rate (eGFR) were also evaluated for the determination of risk factors.
UUI assessment
The primary end point of the study was whether UUI had been experienced in the past 12 months, which was assessed by self-report. Participants were asked the following questions to decide SUI or UUI.1,2 “(1) Have you leaked or lost control of even a small amount of urine with an activity like coughing, lifting or exercise? (2) Have you leaked or lost control of even a small amount of urine with an urge or pressure to urinate and you could not get to the toilet fast enough?” The assessment of UUI by the self-reported questionnaire was proved as effective and reliable. 15 The participants excluded from UUI were considered non-cases.
Statistical analysis
All the continuous variables were represented by mean ± standard deviation (SD) and the classified variables were counted by proportion in this study. Chi-square analysis was conducted to investigate the characteristics of all qualified participants. Eight kinds of PFCs and total PFCs were classified into tertiles. Logistic regression was conducted to determine the corrected odds ratios (ORs) with 95% confidence interval (CI) for PFC-related UUI occurrence in this study. Univariate and multivariate models were established for the evaluation of relationship between PFCs and UUI. In the basic multivariate model, the age, race, marital status and education of the participants were included for the determination. The additional factors including vigorous/moderate recreational activities, hypertension, diabetes and BMI were adjusted in the core model. Subsequently, the eGFR was adjusted in the extended model. Finally, restricted cubic spline was conducted to characterize the dose-response relationship between continuous PFCs exposure and the occurrence of UUI. All the analyses were conducted by using R (version 3.5.3) and SPSS software (version 24.0) with two-tailed p < 0.05 considering as statistically significant.
Results
Sample characteristics
A total of 3157 participants retrieved from NHANES 2007–2014 were included in this study. The baseline characteristics of all participants are detailed in Table 1. There were 2244 (71.1%) participants without UUI and 913 (28.9%) with UUI. The results of chi-square analysis demonstrated that there were significant differences among several variables, i.e., age (p < 0.001), race (p < 0.001), marital status (p = 0.002), education (p < 0.001), vigorous recreational activities (p < 0.001), moderate recreational activities (p = 0.001), hypertension (p < 0.001), diabetes (p < 0.001), BMI (p < 0.001), creatinine (p < 0.001), eGFR (p < 0.001), and total PFCs (p < 0.001). Participants with UUI were tended to be older and unmarried. As for other variables, participants with UUI were concentrated in non-Hispanic white (48.3%), less moderate recreational activities (64.4%), hypertension-positive (52.0%), and BMI (⩾ 25.0 kg/m2, 75.8%). Additionally, participants with UUI had higher creatinine, total PFCs, PFHs, MPAH, PFNA, and lower eGFR compared with participants without UUI. The relationship between PFCs with significant differences and UUI was visualized by violin diagram in Figure 2.
Demographic characteristics of eligible female NHANES population a .

For categorical variables, p values were analyzed by chi-square tests. For continuous variables, the t-test for slope was used in generalized linear models.
BMI, body mass index; eGFR, estimated glomerular filtration rate; MPAH, 2-(N-methyl-perfluorooctane sulfonamido) acetate; NHANES, National Health and Nutrition Examination Survey; PFBS, perfluorobutane sulfonate; PFCs, polyfluoroalkyl chemicals; PFDE, perfluorodecanoic acid; PFDO, perfluorododecanoic acid; PFHP, perfluoroheptanoic acid; PFHS, perfluorohexane sulfonic acid; PFNA, perfluorononanoic acid; PFUA, perfluoroundecanoic acid; SD, standard deviation; UUI, urge urinary incontinence.

Violin diagram of the relationship between total PFCs, PFHS, MPAH, and PFNA with the occurrence of UUI.
We further investigated the characteristics of qualified participants based on the fraction of total PFCs in Table 2. The results indicated that participants with higher serum total PFCs were associated with characteristics including elder, non-Hispanic White, unmarried, no-hypertension, higher creatinine, and lower eGFR.
Characteristics of the weighted population by categories of total PFC levels a .
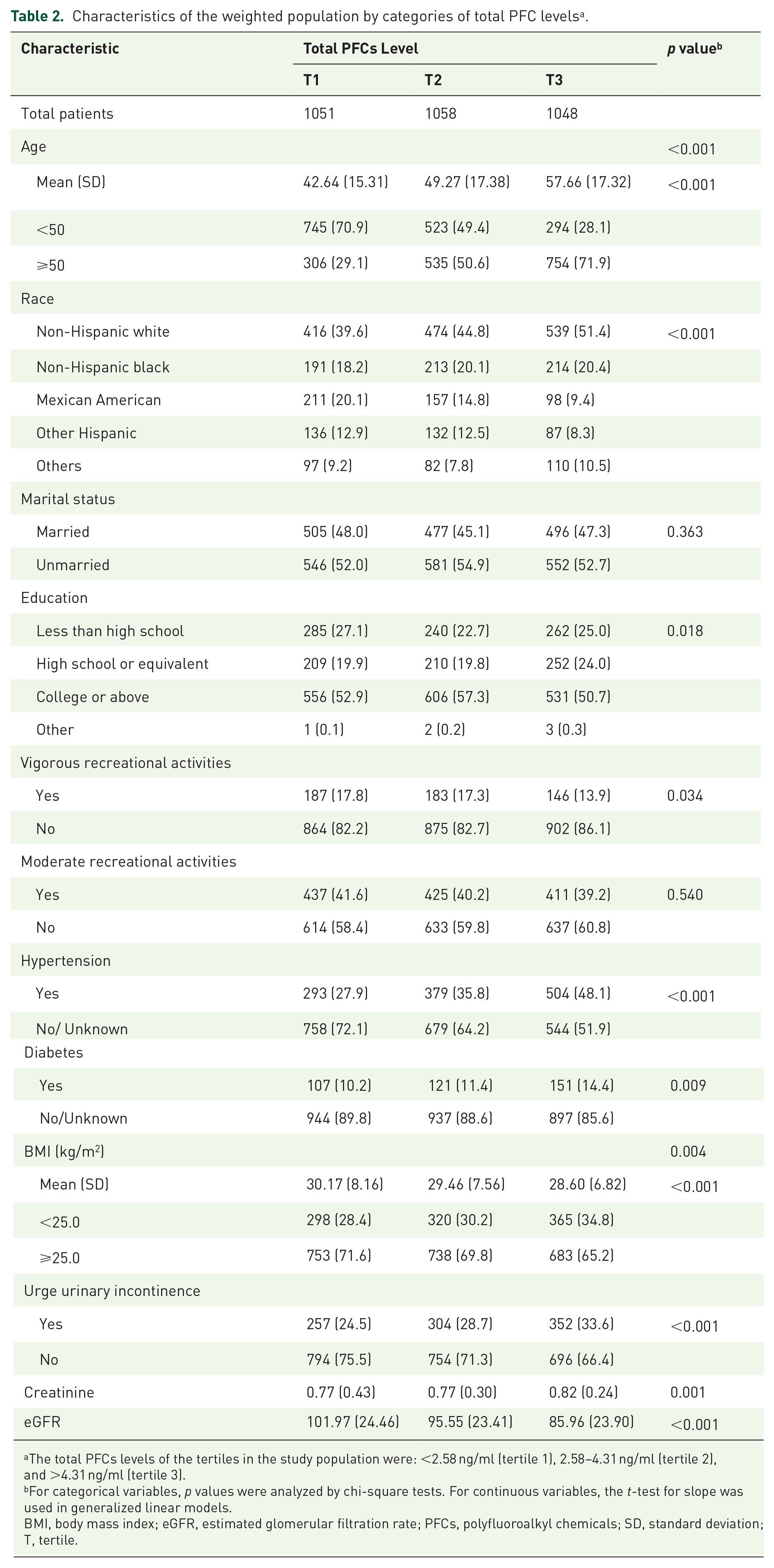
The total PFCs levels of the tertiles in the study population were: <2.58 ng/ml (tertile 1), 2.58–4.31 ng/ml (tertile 2), and >4.31 ng/ml (tertile 3).
For categorical variables, p values were analyzed by chi-square tests. For continuous variables, the t-test for slope was used in generalized linear models.
BMI, body mass index; eGFR, estimated glomerular filtration rate; PFCs, polyfluoroalkyl chemicals; SD, standard deviation; T, tertile.
Serum PFCs and UUI
Logistic regression analysis was conducted to further examine the risk factors related with the occurrence of UUI (Table 3). The results of univariate model showed that total PFCs (p < 0.001), PFHS (p < 0.001), MPAH (p < 0.001), and PFNA (p = 0.002) were the risk factors for UUI. The adjusted OR (aOR; 95% CI) in higher tertiles of total PFCs were 1.25 (1.03–1.51) and 1.56 (1.29–1.89), respectively, compared with the lowest tertile. The positive associations were also found in PFHS, MPAH, and PFNA with significant statistical difference. Simultaneously, the positive associations of serum levels of total PFCs, PFHS, MPAH, and PFNA with the occurrence of UUI were confirmed in multivariate logistic regression analyses of three models.
Adjusted ORs of associations between the PFCs and UUI in different models. a

Adjusted covariates: Basic model: age, race, education levels, and marital status; core model: basic model plus vigorous recreational activities, moderate recreational activities, diabetes, hypertension, and BMI; Extended model: core model plus creatinine and eGFR.
aOR, adjusted odds ratio; BMI, body mass index; CI, confidence interval; eGFR, estimated glomerular filtration rate; OR, odds ratio; T, tertile.
The results from the models indicated the same positive correlation between total PFCs, PFHS, MPAH, and PFNA with the occurrence of UUI. In the basic model, the aORs (95% CI) in higher tertiles of total PFCs were 1.23 (1.02–1.50) and 1.51 (1.24–1.83), compared with 1.17 (0.96–1.43) and 1.33 (1.09–1.63) in the core model. And the results of extended model indicated that the aOR (95% CI) in higher tertiles of total PFCs were 1.11 (0.93–1.38) and 1.21 (1.03–1.53). The dose–response relationship between ORs of UUI and serum PFCs are shown in Figure 3. A positive dose–response relationship between serum levels of total PFCs, PFHS, MPAH, and PFNA were found with the occurrence of UUI.

The dose–response analysis between kinds of PFCs with UUI in the weighted population, with eight kinds of PFCs including PFDE, PFHS, MPAH, PFBS, PFHP, PFNA, PFUA, and PFDO.
Discussion
The occurrence of UUI, which can be attributed to abnormalities in detrusor function and/or neural signaling, seriously threatens health in female patients and imposes a huge burden on society. 16 In this study, we conducted various analyses to investigate the relationship between serum PFCs and UUI occurrence based on the NHANES database, which represents the population in the US. It was found that serum levels of total PFCs, PFHS, MPAH, and PFNA were positively correlated with UUI occurrence, and higher than in participants without UUI based on the results in this work. To further confirm these results, we adjusted for age, race, marital status, education, vigorous/moderate recreational activities, hypertension, diabetes, BMI, and eGFR in multivariate logistic regression models and the results indicated that total PFCs, PFHS, MPAH, and PFNA in the higher tertile was accompanied with a higher chance of suffering from UUI compared with the lowest tertile.
For their unique structure, which is similar to fatty acids, PFCs as artificial compounds have been used widely in the generation of various industrial products for commerce, including textile stains; grease-proof, food-contact paper; flame-retardant foams, etc.17,10 The harmful impacts on human health of PFCs have been gradually recognized by society through continuous scientific research and reporting. PFCs accumulate primarily in the serum, kidney, liver, lung, and brain, which causes various adverse effects on the immune, reproductive systems, etc., due to their properties of indefinite persistence and long half-life. 18 In particular, excessive exposure to perfluorooctane sulfonic acid (PFOS) and perfluorooctanoic acid (PFOA), two common types of PFCs, can induce disorders in fetuses, high carcinogenicity, cholesterol metabolism impairment, toxicity for reproduction, etc.17,10,18,19 Since the beginning of this century, there have been continuous measures to reduce the production of PFCs for the protection of human health, and the major manufacturers agreed in 2000 to gradually decrease production capacity of PFOA and PFOS.20,21 However, PFCs still can be detected in human serum even after the implementation of protective methods, and the harmful effects of various PFCs on health warrant further exploration.
As an important component of excretory function, renal metabolism undertakes the task of eliminating toxic substances, causing the kidney to be the main target organ of the toxic effects of PFCs.10,22 Several previous studies had reported epidemiological evidence confirming the positive association between accumulative serum levels of PFCs with renal function decrease.10,23 Watkins et al. conducted a cross-sectional analysis of 9660 children aged 1–18 years investigating the relationship between PFC exposure and renal function, and found that PFOA was associated with renal function impairment in adolescents. 24 Through the cross-sectional survey from NHANES database, Mao et al. reported a positive relationship between serum total PFCs and PFHS with increased occurrence of kidney stones. 10 All the above evidence indicates that the nephrotoxicity of PFCs impaired renal function and caused irreversible harmful effects on human health.
The results of this study demonstrate the positive relationship between serum PFCs and UUI occurrence and the potential mechanism needs further exploration. The current evidence could not directly prove the potential molecular mechanism. We assume that oxidative stress functions as a stimulator in the process, which includes inflammation, reactive oxygen species (ROS), etc. The present study has confirmed inflammatory injury as the stimulator inducing the formation of UUI.25,26 Serum PFCs could increase oxidative stress, microvascular endothelial permeability, and up-regulation of the expression of Nrf2,27,28 which may lead to inflammatory injury and polyuria caused by renal impairment. Additionally, disorders in fatty acid β-oxidation related to serum PFCs could also be attributed to UUI occurrence. 29 The ROS generated during multiple cellular activities and the imbalance of ROS generation and elimination would contribute to inflammatory injury.30,31 This evidence indicates a potential molecular mechanism for the occurrence of UUI induced by serum PFCs. This study provides the first epidemiological evidence of the association between serum PFCs and UUI occurrence; it was found that increased serum PFCs could induce the occurrence of UUI though oxidative stress.
This study revealed the relationship between serum PFCs and UUI occurrence using data from the NHANES database. After adjusting for potential confounding variables, this work concluded that serum total PFCs, PFHS, MPAH, and PFNA were risk factors for UUI occurrence. However, the study had some limitations as follows. First, as retrospective research, the study contained inevitable bias. The mental state of the participants was not taken into account; therefore, neurological issues have not been ruled out. Second, the study lacked insight into the condition of patients regarding urge incontinence. Additionally, the conclusions drawn from this work need further multi-center prospective studies for verification.
Conclusion
This study investigated the relationship between PFCs and UUI in female participants in the nationally representative cross-sectional NHANES database. After adjusting for potential confounding variables, it was found that total PFCs, PFHS, MPAH, and PFNA were correlated positively with the risk of UUI occurrence. The results will contribute to developing individualized treatment for women suffering from UUI.
Footnotes
Author contributions
CX and SC: designed the experiments.
SC, SZ and QG: analyzed the data.
SC, CX, XZ and XC: wrote the paper.
Conflict of interest statement
The author(s) declare that there is no conflict of interest.
Funding
The author(s) received no financial support for the research, authorship, and/or publication of this article.
Ethical Statement
The present study was complied with the 1964 Helsinki Declaration and its later amendments or comparable ethical standards (as revised in 2013). This study used previously collected deidentified data, which was deemed exempt from review by the Ethics Committee of the Second Affiliated Hospital of Zhengzhou University.
Availability of data and materials
The datasets used and/or analyzed during the current study are available from the corresponding author on reasonable request.