
Abstract
Background
Lifestyle modification is widely recognized as the primary strategy for managing nocturia; however, the association between physical activity and nocturia remains unclear. This study aimed to examine this relationship.
Methods
We analyzed data from the National Health and Nutrition Examination Survey conducted between 2007 and 2016. Physical activity and nocturia frequency were assessed using questionnaires. Weighted logistic regression was applied to evaluate their association.
Results
Among 25,184 participants, 31.1% reported no nocturia episodes, 55.2% had one to two episodes, 11.6% had three to four episodes, and 2.1% had five or more episodes. Physical activity levels differed significantly across groups. After adjustment for multiple variables, vigorous physical activity was associated with a lower risk of nocturia (odds ratio, 0.92; 95% confidence interval: 0.86–0.98; P = 0.007). Participants who engaged in vigorous activity also reported fewer nocturia episodes (odds ratio, 0.96 for one to two episodes, P = 0.02; 0.80 for three to four episodes, P < 0.001; and 0.73 for five or more episodes, P = 0.007). This association remained consistent across most subgroups.
Conclusion
Vigorous physical activity is associated with a lower risk and severity of nocturia. These findings suggest that increasing physical activity may help prevent or reduce nocturia, although further cohort studies are warranted to confirm these results.
Keywords
Introduction
In 2002, the International Continence Society defined nocturia as a condition in which an individual awakens during the night to void at least once because of the sensation of urinary urgency. 1 Nocturia is highly prevalent, with studies reporting that its prevalence among men and women younger than 40 years ranges from approximately 11% to 35.2% and 20.4% to 43.9%, respectively. In contrast, the prevalence among older men and women above 70 years increases, ranging from 68.9% to 93% in men and 74.1% to 77.1% in women. 2 Furthermore, nocturia can substantially affect the sleep quality of the affected individuals and their partners. 3 Studies have shown that sleep disruption caused by nocturia is associated with an increased risk of depression, hormonal imbalance, immune system dysregulation, and metabolic disorders. 4 In older individuals, nocturia markedly increases the risk of falls, hip fractures, and cardiovascular diseases, thereby increasing mortality risk.5–7 Similarly, in younger individuals with nocturia, frequent nocturia episodes are significantly correlated with increased mortality. 7 Therefore, addressing nocturia is crucial for improving the quality of life of affected individuals and reducing mortality risk.
Treatment options for nocturia include lifestyle modification and pharmacotherapy, with lifestyle modification generally regarded as the first-line approach. 8 These strategies involve emptying the bladder prior to sleep, implementing nighttime fluid restriction, limiting dietary and fluid intake (such as avoiding caffeinated beverages and alcohol), adjusting medication timing (e.g. taking diuretics in the afternoon), elevating the legs at night to facilitate fluid redistribution, using sleep aids or medications, and employing protective undergarments, among others. 9 Some researchers have suggested that individuals with overactive bladder (OAB) perform pelvic floor muscle exercises to reduce nocturnal urgency, with varying degrees of success. 10 Recent studies have shown that physical activity substantially contributes to alleviating lower urinary tract symptoms (LUTS) associated with benign prostatic hyperplasia (BPH) 11 and urinary incontinence. 12 However, evidence regarding the effect of physical activity on nocturia remains limited. Previous research has demonstrated that physical activity is beneficial for improving nocturia in older individuals with BPH; 13 however, it remains uncertain whether such benefits extend to the general population with nocturia. Therefore, this study used data from the National Health and Nutrition Examination Survey (NHANES) database to conduct a cross-sectional analysis examining the relationship between physical activity and nocturia, thereby providing relevant clinical insights. This cross-sectional study has been reported in accordance with the Strengthening the Reporting of Cohort, Cross-sectional and Case–control Studies in Surgery (STROCSS) guidelines. 14
Methods
Study population
The NHANES is a major initiative by the National Center for Health Statistics (NCHS) to systematically collect data on dietary habits, health status, and other characteristics of the civilian population in the United States, thereby ensuring a comprehensive dataset. The NHANES protocol was approved by the Ethics Review Committee of the NCHS, and all participants provided written informed consent. Detailed information is available on the Centers for Disease Control and Prevention website: https://www.cdc.gov/nchs/nhanes/. For this analysis of the association between physical activity and nocturia, five NHANES cycles conducted between 2007 and 2016 were included.
Initially, 50,588 individuals were recruited. Through a systematic screening process, the following participants were excluded: those younger than 20 years (21,387 individuals), those who lacked or did not provide information on nocturia (3936 individuals), and those missing data on physical activity and demographic variables (81 individuals). After applying these exclusion criteria, 25,184 participants were included in the final analysis (Figure 1).

Flowchart of participant selection.
Exposure variable
In this study, physical activity was used as the exposure variable. The World Health Organization defines physical activity as any bodily movement produced by any skeletal muscles that requires the expenditure of energy. In this study, we included moderate activity and vigorous physical activity based on questionnaire data.
Moderate work activity was defined as moderate-intensity activity, such as brisk walking or carrying light loads, that caused small increases in breathing or heart rate and was performed for at least 10 min continuously. Moderate recreational activity was defined as moderate-intensity sports, fitness, or recreational activity, such as brisk walking, bicycling, swimming, or playing golf, that caused a small increase in breathing or heart rate and was performed for at least 10 min continuously. Moderate activity was defined as engaging in moderate work and/or moderate recreational activity during a typical week.
Vigorous work activity was defined as vigorous-intensity activity, such as carrying or lifting heavy loads, digging, or construction work, that caused large increases in breathing or heart rate and was performed for at least 10 min continuously. Vigorous recreational activity was defined as vigorous-intensity sports, fitness, or recreational activity, such as running or playing basketball, that caused large increases in breathing or heart rate and was performed for at least 10 min continuously. Vigorous activity was defined as engaging in vigorous work and/or vigorous recreational activity during a typical week.
Daily sitting time referred to the total time spent sitting at work, at home, while traveling, or during leisure activities, including sitting at a desk, traveling in a car or bus, reading, playing cards, watching television, or using a computer. Time spent sleeping was excluded. Daily sitting time was assessed using the question, “How much time do you usually spend sitting on a typical day?” and categorized into four groups: <3 h, 3–5 h, 5–7 h, and ≥7 h.
Outcome variable
Information on nocturia was obtained from a questionnaire. Participants were asked, “During the past 30 days, how many times per night did you typically get up to urinate from the time you went to bed at night until the time you got up in the morning?” The frequency of nocturia was recorded and categorized into four groups: 0, 1–2, 3–4, and ≥5 times.
Covariable definition
Baseline data for participants were collected through a questionnaire, which included the following categories. 1. Sex was classified as male or female. 2. Age was categorized as <40 years, 40–60 years, 60–80 years, and ≥80 years. 3. Race/ethnicity was classified as Mexican American, non-Hispanic White, non-Hispanic Black, or other. 4. Alcohol consumption was categorized as nondrinker, 1–5 drinks per month, 5–10 drinks per month, and more than 10 drinks per month. 5. Smoking status was classified as nonsmoker, former smoker, or current smoker. 6. Education level was divided into two groups: high school and above versus high school and below. 7. Body mass index (BMI) was stratified into three categories: <25.0 kg/m2, 25.0–30.0 kg/m2, and ≥30 kg/m2. 8. Income was assessed using the poverty income ratio (PIR), which was calculated by dividing family income by the specific poverty threshold for that family size and was categorized as ≥3.0 or <3.0. 9. Information on the prevalence of hypertension and diabetes was obtained from self-reported questionnaires.
Statistical analysis
Sampling weights are essential for NHANES analyses, and data spanning five cycles over 10 years were obtained by multiplying the 5-year weights by 0.2. Baseline characteristics were described according to physical activity groups and nocturia levels. Continuous variables were assessed for normality. Variables with a normal distribution were analyzed using independent samples t-tests or analysis of variance (ANOVA), whereas non-normally distributed variables were analyzed using the Kruskal–Wallis test. The chi-square test was used to compare categorical variables.
To examine the correlation between physical activity and nocturia, multivariable-adjusted logistic regression was performed to estimate adjusted odds ratios (OR) and 95% confidence intervals (CIs). The crude model included no covariates, whereas the adjusted model accounted for sex and age. The fully adjusted model further included all covariates, including age, sex, race/ethnicity, alcohol consumption, smoking status, education level, BMI, income, and the presence of hypertension and diabetes. Subgroup analyses were conducted to explore potential differences among various populations. All analyses were performed using R version 4.3.2, and a two-sided p-value of <0.05 was considered statistically significant.
Results
Baseline characteristics of participants
The study comprised 25,184 participants. Based on nocturia frequency, participants were divided into four groups: 0, 1–2, 3–4, and ≥5 times, accounting for 7844 (31.1%), 13,899 (55.2%), 2904 (11.6%), and 537 (2.1%) participants, respectively. As shown in Table 1, the proportions of sex, age group, race/ethnicity, alcohol consumption, smoking status, marital status, education level, PIR, BMI category, diabetes, hypertension, daily sitting time, and moderate and vigorous physical activity differed significantly across the nocturia frequency groups. Participants with higher nocturia frequency tended to have longer daily sitting times and were less likely to engage in moderate or vigorous activity.
Baseline characteristics of participants from the NHANES, 2007–2016.

Median (interquartile range) for continuous; n (%) for categorical
Pearson’s chi-square test
NHANES: National Health and Nutrition Examination Survey; PIR: poverty income ratio; BMI: body mass index.
Association between physical activity and nocturia
In the analysis of the association between physical activity and nocturia, Table 2 shows that daily sitting time was positively correlated with nocturia in the crude model (<3 h: Reference; 3–5 h: OR = 1.10, P = 0.038; 5–7 h: OR = 1.10, P = 0.024; ≥7 h: OR = 1.02, P = 0.6). In contrast, moderate activity (OR = 0.80, 95% CI: 0.76–0.85, P < 0.001) and vigorous activity (OR = 0.59, 95% CI: 0.55–0.62, P < 0.001) were negatively correlated with nocturia in the crude model. After adjusting for partial covariates, including age and sex, daily sitting time and moderate activity were not correlated with nocturia; however, vigorous activity remained negatively correlated with nocturia (OR = 0.84, 95% CI: 0.79–0.90, P < 0.001). Following adjustment for all covariates listed in Table 1, vigorous activity remained negatively correlated with nocturia (OR = 0.92; 95% CI: 0.86–0.98, P = 0.007).
Association between physical activity and nocturia.
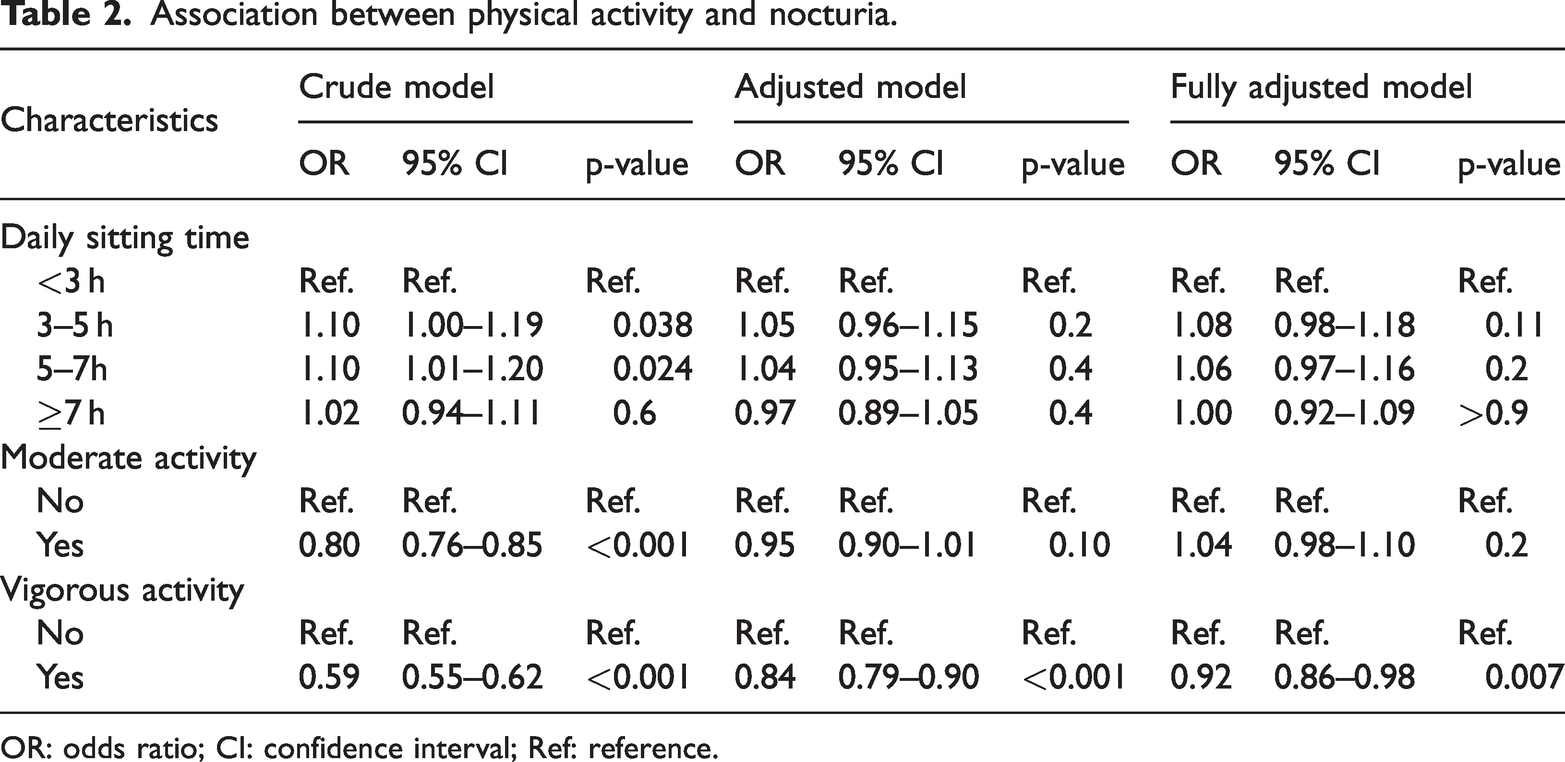
OR: odds ratio; CI: confidence interval; Ref: reference.
Association between vigorous activity and frequency of nocturia
In the analysis of the association between vigorous activity and frequency of nocturia, Table 3 shows that the higher frequency of nocturia was negatively correlated with vigorous activity in the crude model (0: Reference; 1–2 times: OR = 0.66, P < 0.001; 3–4 times: OR = 0.35, P < 0.001; ≥5 times: OR = 0.33, P < 0.001). After adjusting for age and sex, the frequency of nocturia remained negatively correlated with vigorous activity (0: Reference; 1–2 times: OR = 0.91, P = 0.002; 3–4 times: OR = 0.63, P < 0.001; ≥5 times: OR = 0.52, P < 0.001). Following adjustment for all covariates listed in Table 1, frequency of nocturia remained negatively correlated with vigorous activity (0: Reference; 1–2 times: OR = 0.96, P = 0.02; 3–4 times: OR = 0.80, P < 0.001; ≥5 times: OR = 0.73, P = 0.007).
Association between frequency of nocturia and vigorous activity.

OR: odds ratio; CI: confidence interval; Ref: reference.
Subgroup analyses
Subgroup analyses based on various covariates were conducted to evaluate the relationship between vigorous activity and nocturia, with the aim of identifying potential population differences. As shown in Supplemental Table 1, a consistent negative correlation between vigorous activity and nocturia was observed among participants who were non-Hispanic White (OR = 0.9, 95% CI: 0.82–0.99, P = 0.031), nondrinkers (OR = 0.83, 95% CI: 0.73–0.95, P = 0.005), nonsmokers (OR = 0.86, 95% CI: 0.79–0.93, P < 0.001), had an education level of high school and above (OR = 0.92, 95% CI: 0.85–1.00, P = 0.044), had a PIR of <3.0 (OR = 0.91, 95% CI: 0.84–0.99, P = 0.020), had a BMI of ≥30 kg/m2 (OR = 0.84, 95% CI: 0.75–0.94, P = 0.002), and did not have diabetes (OR = 0.92, 95% CI: 0.86–0.98, P = 0.013) or hypertension (OR = 0.92, 95% CI: 0.86–0.99, P = 0.023).
Discussion
In this study, we conducted a cross-sectional analysis using data from NHANES to examine the relationship between physical activity and nocturia. Our findings indicate that vigorous physical activity acts as a protective factor against nocturia. Furthermore, the frequency of nocturia showed a dose–response relationship with vigorous activity, with stronger protective effects observed among participants who experienced more frequent nocturia episodes. After adjusting for confounding variables, vigorous activity remained independently and negatively correlated with nocturia. Subgroup analyses further revealed that participants who were non-Hispanic White, nondrinkers, nonsmokers, had an education level of high school and above, a PIR of <3.0, a BMI of ≥30 kg/m2, and did not have diabetes or hypertension appeared to benefit more from engaging in vigorous activity. To the best of our knowledge, this study provides the first evidence suggesting that physical activity serves as a protective factor against nocturia.
Physical activity has been associated with various urological conditions. Previous studies have shown that physical activity can improve the management of urinary incontinence in older women. Michelle et al. 15 analyzed data from 30,213 women in the NHANES database and found that 23.15% of women had stress urinary incontinence, 23.16% had urgency urinary incontinence, and 8.42% had mixed urinary incontinence. Moderate physical activity was found to be negatively correlated with the incidence of all three types of urinary incontinence. The authors suggested that physical activity may strengthen pelvic floor muscles and enhance mental well-being, thereby alleviating symptoms of urinary incontinence. Another systematic review investigated the association between physical activity and the incidence of urinary incontinence among older women. It found that a sedentary lifestyle and less than 150 min of physical activity per week were positively correlated with an increased risk of urinary incontinence, whereas moderate- to high-intensity physical activities were negatively correlated. 16 Furthermore, evidence suggests that physical activity can also ameliorate LUTS among older men with BPH. Fowke et al. 17 included 405 patients diagnosed with BPH to assess the relationship between physical activity levels and LUTS severity; they found a negative correlation between these variables. Notably, this negative association was particularly pronounced among patients with obesity. A subsequent systematic review examined the relationships between physical activity, BPH, and LUTS severity and reported significant negative associations for moderate (OR = 0.74, 95% CI: 0.60–0.92, P = 0.005) and vigorous activity (OR = 0.74, 95% CI: 0.59–0.92, P = 0.006) with respect to BPH and LUTS outcomes. 11 Additionally, research has indicated a link between physical activity and urolithiasis incidence. Ya et al. 18 conducted a comprehensive analysis utilizing the NHANES database, which included 19,188 participants, and found that increased daily sedentary time was associated with a higher risk of developing urinary urolithiasis. Notably, subgroup analyses showed that this association was not observed among individuals engaging in vigorous activity, suggesting that vigorous activity may mitigate the risk of urinary urolithiasis linked to sedentary sitting.
Nocturia is a prevalent clinical symptom within the urinary system, characterized by a complex etiology. Consequently, there is currently no standardized treatment protocol for individuals with nocturia. Most studies suggest that lifestyle modification is the primary approach to managing this condition. Although research indicates that physical activity can alleviate various LUTS, its specific impact on nocturia remains limited. Sugaya et al. 19 investigated whether moderate activity could ameliorate nocturia symptoms in older individuals and enrolled 31 older men in an 8-week program of moderate-intensity exercise. The results demonstrated a significant reduction in night urination frequency (3.3 ± 0.7 vs. 1.9 ± 0.8), with 67% of participants reporting deeper sleep following the intervention and 60% noting substantial improvements in their overall quality of life. Another study involving 56 patients with nocturia reported that lifestyle adjustments, including fluid intake restriction, minimizing excessive time spent in bed, engaging in moderate daily exercise, and maintaining warmth during sleep, significantly reduced the night urination frequency and total nighttime urine volume. 20 In patients with BPH, researchers have observed that those engaging in more than 1 h of physical activity per week experienced a 13% decrease in the incidence of nocturia and a 34% reduction in severe cases. 13 These findings align with our own results; however, subgroup analyses indicate that physical activity does not effectively reduce nocturia incidence among specific populations, such as smokers, drinkers, or individuals with hypertension or diabetes. Current literature identifies smoking, 21 alcohol consumption, 22 hypertension, 23 and diabetes 24 as definitive risk factors for nocturia, which may reduce the efficacy of physical activity interventions for this condition. Therefore, we believe that for individuals with specific comorbidities and triggers, controlling these factors should remain the primary approach to alleviate nocturia, and physical activity can be used as an auxiliary method to improve symptoms in this patient group.
The mechanisms through which physical activity mitigates nocturia may involve several dimensions. First, engaging in physical activity has been shown to improve sleep quality and increase the duration of deep sleep, thereby partially alleviating symptoms of nocturia.25,26 Second, nocturia is often associated with psychological conditions such as stress, anxiety, and depression. 27 Current research suggests that physical activity can effectively reduce psychological stress and anxiety while promoting overall mental well-being, consequently resulting in improvements in nocturia. 28 Third, physical activity is known to increase renal blood flow, which may result in increased urine output during the day. 29 Therefore, we propose that engaging in daytime vigorous physical activity may facilitate greater fluid excretion from the body, thereby reducing nighttime urine volume and mitigating symptoms of nocturia. Nevertheless, further empirical evidence is required to substantiate this hypothesis.
The strengths of this study are as follows. 1. This research utilized the NHANES database to investigate the relationship between physical activity and nocturia, effectively representing the actual conditions of the US population and demonstrating strong generalizability. 2. The study included a large sample size with clearly defined research and outcome indicators. By adjusting for confounding factors, it provides a more accurate reflection of the association between physical activity and nocturia. However, this study has several limitations: 1. As the NHANES database is derived from a cross-sectional survey design, it can only assess correlations between physical activity and nocturia without establishing definitive causal relationships; therefore, cohort studies are needed to further elucidate these associations. 2. The diagnosis of nocturia and the assessments of physical activity were based on self-reported questionnaire data, which may have introduced recall bias. 3. Several factors that may influence nocturia, such as sleep apnea, diuretic use, depressive status, and OAB, were not available in the NHANES database. Consequently, the possibility of residual confounding cannot be ruled out. 4. As the study was based on data from the US population, the generalizability of the findings to non-US populations requires further validation in other ethnic or national groups. Although our findings indicate a significant association between physical activity and nocturia, the underlying mechanisms remain unexplored and warrant further investigation.
Conclusion
Our study identified a significant association between physical activity and nocturia. Participants who engaged in vigorous activity demonstrated a negative correlation with nocturia, and the severity of nocturia symptoms was inversely associated with vigorous activity. These findings suggest that physical activity may contribute to reducing the incidence and severity of nocturia; however, further cohort studies are needed to validate these results.
Supplemental Material
sj-pdf-1-imr-10.1177_03000605251394177 - Supplemental material for Association between physical activity and nocturia: A cross-sectional study using National Health and Nutrition Examination Survey 2007–2016
Supplemental material, sj-pdf-1-imr-10.1177_03000605251394177 for Association between physical activity and nocturia: A cross-sectional study using National Health and Nutrition Examination Survey 2007–2016 by Yayong Qiang, Bin Yang, Wei Guo and Ruotao Xiao in Journal of International Medical Research
Footnotes
Acknowledgments
The authors express gratitude to the NHANES database for providing access to this valuable dataset.
Author contributions
Yayong Qiang and Bin Yang conducted data collection, analysis, and interpretation. Ruotao Xiao contributed to literature review and data visualization. Yayong Qiang and Ruotao Xiao drafted the initial manuscript, and all authors made critical revisions. Wei Guo verified the underlying data. All authors read the manuscript and approved the final draft. All authors confirm that they had full access to all the data in the study and accept responsibility to submit for publication.
Availability of data and materials
Consent for publication
Not applicable.
Declaration of conflicting interests
The authors declare no competing interests.
Ethics approval and consent to participate
Not applicable.
Funding
This study received support from the Key Clinical Projects of Peking University Third Hospital (No. BYSYZD2023050) and the Yan’an Science and Technology Plan Projects (Number: 2023-SFGG-098).
Supplemental material
Supplemental material for this article is available online.
References
Supplementary Material
Please find the following supplemental material available below.
For Open Access articles published under a Creative Commons License, all supplemental material carries the same license as the article it is associated with.
For non-Open Access articles published, all supplemental material carries a non-exclusive license, and permission requests for re-use of supplemental material or any part of supplemental material shall be sent directly to the copyright owner as specified in the copyright notice associated with the article.