
Abstract
Aims:
Urinalysis is used as a first-line investigation throughout healthcare to indicate bacteriuria and guide treatment of potential urinary tract infections. In light of rising bacterial multi-resistance, we aim to analyse its diagnostic accuracy, determine its usefulness in a present-day setting and evaluate current antibiotic resistance patterns across a Trust population.
Methods:
A retrospective case series of 712 paired urinalysis and urine culture results was obtained over a 1-month period. Sensitivity, specificity and diagnostic accuracy were calculated, and resistance profiles of commonly used Trust antibiotics assessed using statistical analysis.
Results:
A high false negative rate of nitrites on urinalysis, with sensitivity of 38.4%, was found. Leucocyte sensitivity was 87.6% and specificity 39.7%, with no improvement in diagnostic accuracy seen when combining both. Positive urine culture growth demonstrated a substantial resistance pattern to trimethoprim of 48%, compounded by a statistically significant correlation with gentamicin resistance (p < 0.0001).
Conclusion:
Our study has highlighted a reduced accuracy of urinalysis compared with previous literature, questioning its usefulness in the real world. We have consolidated growing published trends doubting the efficacy of trimethoprim, revealing co-existing resistance patterns between commonly used antibiotics. This will have implications for future antibiotic-prescribing protocols and requires further research to ensure guidelines are progressive in consciously managing this growing concern in modern-day healthcare.
Introduction
Urinary tract infections (UTIs) are thought to cause around 92 million people worldwide to seek medical advice, with this figure increasing annually. 1 In the UK, 11% of women are affected every year and are thought to be three times more likely than men to contract UTIs. 2 Each UTI requiring hospital admission in the United Kingdome (UK) is thought to cost the National Health Service (NHS) £1331. 3 Almost one quarter of all hospital-acquired infections were attributed to a urinary source, with 4800 UTI-related, in-hospital deaths reported across England and Wales in 2012. 4 These figures are on the rise secondary to a multitude of factors, including antibiotic misuse, increased use of urinary tract foreign bodies and the accuracy of point-of-care testing. 5 Tenney et al. found that probable risk factors for multi-resistant UTIs in a literature review in 2018 consisted of catheterisation, recent antibiotic usage and recent hospital admission, demonstrating how crucial the iatrogenic impact is on this high burden disease process, through directly contributing to increasing resistance patterns. 6 The use of empirical antibiotics throughout healthcare settings appears to also add to reversible causes that must be addressed.
UTI is caused predominantly by gram-negative bacteria and, in most studies, the primary pathogen is Escherichia coli. 7 It is thought that certain strains of E. coli predispose to the persistent presence of urothelial bacteria and thus persistent and/or recurrent infections, through an ability to adhere to urothelial mucosa and form dormant intracellular bacterial groups. 8 These organic factors associated with certain subsets of bacteria offer a new problem in treating infections clinically and eradicating bacteriuria, and provide increasing complexity when added to the iatrogenic reasons discussed.
Urine dipstick testing, or urinalysis, remains a widely used initial diagnostic modality in evaluating the presence of bacteriuria, and subsequent antibiotic administration can often be based upon its results. The reagent strip contains pads indicating the presence of leucocytes, nitrites and erythrocytes as well as ketones, glucose and urobilinogen, and demonstrates urine pH and specific gravity. 9 Urinalysis is an inexpensive, quick and user-friendly tool that can be used in variety of clinical settings and scenarios. Previously reported reviews have suggested high levels of sensitivity and specificity; however, controversy has increased in the literature as to whether the urine dipstick test remains appropriate in light of present-day micro-organisms and their resistance patterns. This includes the ability of the test to not only confirm bacteriuria, but to even exclude it, with some studies suggesting samples should always be sent for microscopy, culture and sensitivities. Our aim is to re-evaluate the diagnostic accuracy of the urine dipstick test across a Trust population and determine its usefulness in a post-antibiotic era.
Methods
Fully anonymised consecutive results of paired urine dipstick tests and culture results received in our laboratory were evaluated over a 1-month period, in December 2017, following approval from our ‘Clinical Governance and Audit’ team at our Trust. All dipstick analysis was undertaken using an automated Roche analyser as a near patient test and reported on a central server. Significant bacteriuria was defined as single culture >105 colony-forming units (CFU)/ml, as per our Trust reporting policy. The sensitivity and specificity were calculated for nitrites, leucocytes and combinations of both. Finally, the diagnostic accuracy was stratified according to resistance profiles to commonly prescribed antibiotics. These include trimethoprim, pivmecillinam, nitrofurantoin, ciprofloxacin and gentamicin. Finally, we aimed to establish if one antibiotic resistance, as defined by Falagas et al. and Magiorakos et al., resulted in an increased chance of other antibiotic resistance using the Chi squared test.10,11
Results
Overall, 3108 urinalysis results and 1088 urine culture results were obtained via central servers. From these, 712 directly paired results were found and analysed further. These were obtained after excluding:
Urinalysis results without subsequent sample sent for culture;
Urine cultures without prior urinalysis results (such as from general practice);
Duplicates.
Any incorrect labelling of samples was rejected by the server prior to our data collection and therefore not in our analysis.
From the paired results, 147 positive specimens were found. Over half of these were E. coli, with 16% Enterococcus and 14% Klebsiella pneumoniae. The final 16% included Proteus, Citrobacter and Staphylococcus. This distribution of bacteriuria is similar to that seen in the literature, as shown in Figure 1.
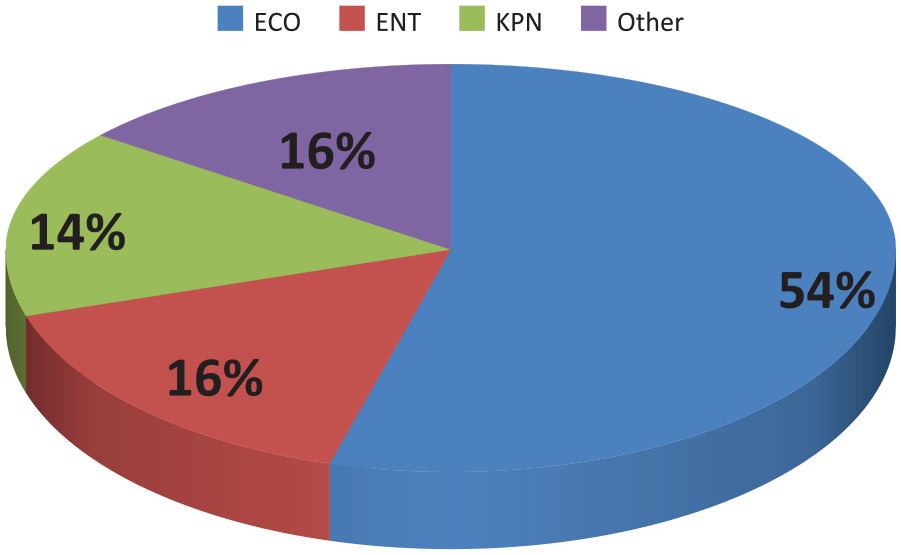
Distribution of cultured bacteria.
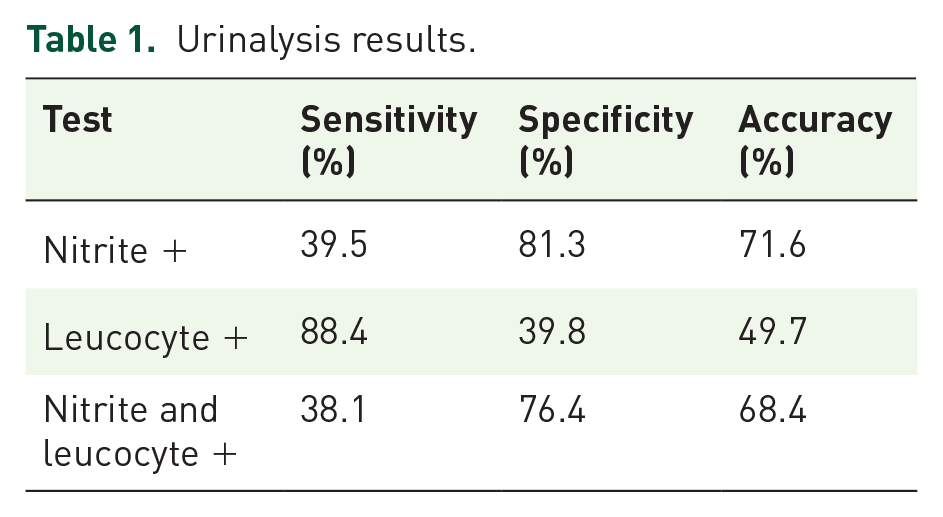
The urinalysis characteristics are highlighted in Table 1. We found nitrite sensitivity to be 39.5%, leucocyte sensitivity to be 88.4%, and combining the two offered a sensitivity of 38.1%. Nitrite specificity was 81.3%, leucocyte specificity at 39.8% and the combination showed specificity of 76.4%. Overall, nitrite showed the highest level of accuracy at 71.6%, with no improvement noted when combined with leucocyte positivity.
Urinalysis results.
The test characteristics of urinalysis stratified for fully sensitive and resistant bacteriuria, compared with characteristics in baseline diagnosing, are shown in Table 2. Of the fully sensitive bacteria, 87.6% demonstrated leucocyte positivity on urinalysis, and 38.4% demonstrated nitrite positivity. Of resistant bacteria, 95.8% were leucocyte positive and 43.6% were nitrite positive. No significant difference was noted.
Urinalysis results stratified for sensitive and resistant bacteriuria.

Of the 147 specimens, 75 (51%) demonstrated resistance to at least one of the five common antibiotics recorded at our Trust to treat UTIs, and the proportionality of this is shown in Figure 2. A comparison of the cultured bacteria between fully sensitive and resistant antibiotics (Figure 3) highlights the considerable height and breadth of trimethoprim resistance across a real-world distribution of positive urine cultures, as well as its disparate sensitivity profile in comparison. Table 2 highlights the comparison of resistance rates with the common antibiotics through all our positive culture specimens. All antibiotics remain under 20% resistance, aside from the 48.7% of bacteria cultured demonstrating resistance to trimethoprim. Figure 4 demonstrates the distribution of resistant bacteria from our study.

Comparing resistance profiles of the five common antibiotics used at our Trust.

Comparison of cultured bacteria across sensitive and resistant antibiotics.

Distribution of resistant bacteria.
Of the trimethoprim-tested urine cultures, 20 of 115 demonstrated sole resistance to trimethoprim, and thus would have been treated successfully by the use of one of our other five commonly used and available antibiotics – four of which are routine oral preparations.
Table 3 demonstrates associated p values following analysis of the resistance patterns; the chance of another antibiotic resistance when associated with trimethoprim resistance. Also presented is the proportion of trimethoprim-resistant cultures that also demonstrated resistance to the other antibiotic tested for, as well as the percentage of resistant cultures for that antibiotic when trimethoprim was found to be sensitive. We found that, when using the Fisher’s exact test, there was a statistically significant association between trimethoprim resistance and gentamicin resistance, with an increased proportion (38.9%) of bacteriuria demonstrating resistance to both. No statistically significant associations were found with nitrofurantoin, pivmecillinam or ciprofloxacin; however, all proportions are presented below.
Statistical analysis associating trimethoprim resistance against other antibiotics.

Upon analysing the bacteriuria, we found that both of our Citrobacter growths and all our Enterobacter faecalis growths showed resistance to trimethoprim and gentamicin, which is an expected finding. Proteus cultures, where tested for gentamicin, demonstrated 100% sensitivity, compared with 50% sensitivity for trimethoprim. All of these demonstrated full sensitivity for nitrofurantoin and ciprofloxacin, where tested.
Discussion
To the best of our knowledge, this is the largest retrospective analysis of paired urine cultures and corresponding dipstick results (n = 712). The sensitivity, specificity and diagnostic accuracy of urinalysis is reduced compared with the literature, without any diagnostic benefit to combining the two main indicators on the reagent strip; the leucocyte and nitrite parameters. Furthermore, trimethoprim resistance patterns, where tested, near 1 in 2, with a statistically significant relationship to gentamicin resistance noted. Urinalysis remains a popular and easily accessed initial diagnostic tool to evaluate bacteriuria, and hence lead clinicians in their work up and subsequent treatment of urinary tract infections.
A small study of 60 female patients by Leman in London concluded that urinalysis was sensitive for indicating UTI in 95.8% of patients, with both leucocyte and nitrite positivity offering a positive predictive value of 100%. 12 Then, 14 years later, Van Delft et al. evaluated a cohort of six Dutch general practices, comprising 234 patients, of which nitrites presence on urinalysis offered a sensitivity of 91%. 13
Conversely, a large meta-analysis conducted by Devillé et al. was able to conclude only that usefulness of urinalysis was primarily for excluding presence of infection if both leucocyte and nitrite results were negative. 14 They stated that the sensitivity of one or both of leucocyte or nitrite being positive was only 75%. This was broken down into nitrite sensitivity in the general population being 50%, and leucocyte sensitivity for bacteriuria 56%. Added to this, they concluded that combining the two with one or both showing positivity increased sensitivity significantly. Moore et al. evaluated 206 female patients and found leucocyte positivity offered 63% sensitivity when compared against urine microscopy, but 95% specificity. 15
Evidently, controversy remains with regards to the accuracy of the urine dipstick test as an initial diagnostic tool. We feel our data offers a retrospective evaluation of a larger cohort than previously performed in the literature. Overall, we found higher false negative rates in urinalysis compared with those seen in the literature. We have demonstrated a large false positive finding from leucocyte results, as well as a large false negative rate when using nitrites as a diagnostic marker, despite them often indicating the presence of bacteriuria. Furthermore, combination of leucocyte and nitrite testing to improve diagnostic accuracy was not found in our study. Our finding of nitrite sensitivity at 39.5% leads to a higher false negative rate than previously described, which can cause discrepancies in the investigation of UTIs and their subsequent treatment. Added to this, when combining the two markers, we only found a sensitivity of 38%, despite a specificity of 76%, leading to no increase in diagnostic accuracy. Over half of our cohort demonstrated resistance, where a nitrite sensitivity of fewer than 45% was found, considerably lower than when comparing bacteriuria to sterile urine; therefore, we can see added diagnostic problems and mistreatment of these serious infections. Furthermore, no significant difference in trends was seen when comparing the diagnostic yield of urinalysis in fully sensitive urine and resistant urine. There was a slight improvement in sensitivity of both diagnostic markers in resistant bacteriuria noted. It is evident that a vicious cycle exists, which is worsening with false findings on initial testing, antibiotic prescription and the incorrect or inadequate treatment of bacteriuria and UTIs.
Further from our study data, we found a significant resistance pattern against trimethoprim of up to 48% of all positive urine cultures grown. When compared with other commonly used antibiotics in our Trust, these remain sensitive to over 83% of bacteria where tested against. This is further compounded by the findings that up to 17% of urine samples tested for trimethoprim sensitivity were solely resistant to it instead, and would have been treated routinely by another oral preparation. We noted that trimethoprim potentially had a greater sensitivity to Proteus cultures than nitrofurantoin; however, where sensitive to trimethoprim, sensitivities to ciprofloxacin and pivmecillinam also existed, and links to this were highlighted in Table 3, where just over 1 in 10 trimethoprim-sensitive cultures were resistant to nitrofurantoin and ciprofloxacin.
From a pragmatic perspective, our analysis is, to our knowledge, the first to evaluate resistance patterns in bacteriuria. In almost one third of urine specimens with trimethoprim-resistant E. coli, gentamicin resistance co-exists. This clearly has implications for the generation of future antibiotic prescribing protocols, particularly for patients who may have failed first line oral antibiotics for UTI in the community. Interestingly, current European Association of Urology (EAU) guidelines describe how the use of trimethoprim should be reserved for areas with known E. coli resistance rates of less than 20%. 16 Despite this, aminoglycoside use is recommended; however, our research suggests a co-existing resistance pattern between the two, requiring further assessment across different geographical areas.
Hirsh et al. evaluated oral antibiotic sensitivities to urine isolates and found a resistance rate to trimethoprim/sulfamethoxazole of 59.8%. 17 They further found low resistance rates for nitrofurantoin however ciprofloxacin was 62.6%. Ahmed et al. recently evaluated 273 urine samples finding a resistance rate to trimethoprim/sulfamethoxazole of 50%. 18 Other antibiotics tested for included gentamicin, which had low resistance rates in keeping with our findings; however, nitrofurantoin had resistance rates of 50.6%. This is an interesting finding that we did not find in our study, especially considering recent National Institute for Health and Care Excellence (NICE) guidelines regarding initial oral antibiotic agents to use in both males and females, and the contrary points made in the EAU guidelines.2,16,19 Both studies also demonstrated a similar bacteria cohort cultured as our study.
We can see that, over the past few years and in more recent literature, trimethoprim resistance is not only evident, but growing. As previously alluded to, trimethoprim and nitrofurantoin remain the first line antibiotics from NICE guidelines to treat suspected lower UTIs in all patients, where no prior susceptibility or culture suggests otherwise. There has been an established link between specific antibiotic prescribing and the development of resistance to said antibiotic for many years.20,21 A recent study by Public Health England evaluating trimethoprim sensitivities in Enterobacteriaceae samples in 2018 established that the geographical variation found regarding trimethoprim resistance could be related partly to the use of trimethoprim in differing locations, alongside certain penicillin-derivatives, including amoxicillin and ampicillin. 22 Interestingly, it was shown that nitrofurantoin use was one of the very few antibiotics that can aid a drive down in trimethoprim resistance, possibly due to reducing the direct selection pressure, and is potentially an option for reducing future resistance complications with trimethoprim. This pattern was not seen with other antibiotics used commonly on the urinary tract. It is worth mentioning that our study does not aim to delineate UTIs from bacteriuria, only the accuracy of the initial test in finding bacteria. High quality studies have also demonstrated that treatment of asymptomatic bacteriuria increases risk of antibiotic resistance as opposed to decreasing the frequency of symptomatic infections in females. 23
Our study has demonstrated that a large resistance pattern to trimethoprim exists, in keeping with recent literature findings. Considering this, the use of trimethoprim as a first-line antibiotic in national guidance will undoubtedly continue to exacerbate this situation. Our Trust guidelines also advise gentamicin use as a first-line intravenous antibiotic for the treatment of UTI requiring hospital admission, and significant links have been shown to exist between their resistance patterns. As described, an alternative in both the guidelines and from co-selection studies is nitrofurantoin. The penetration, or lack of, of nitrofurantoin into the acid milieu of the prostate is well described, and thus its primary ability to treat a UTI in males is controversial, despite its positive selection for current resistance rates.24,25 Nevertheless, NICE supports its initial use in males as a first-line oral antibiotic agent where required.
Conclusion
In conclusion, we can state from our study that urinalysis has a lower than previously reported ability to determine bacteriuria. This is seen by the increased false negative rate of nitrites and the lack of improvement when combining both leucocytes and nitrites. Furthermore, the large pool of resistant bacteria towards trimethoprim has been established, and is seemingly growing, in no small part due to continuing antibiotic pressures and misuses impacting on the diagnostic accuracy of our initial tests. This is significantly associated with coinciding resistance patterns to gentamicin – a first-line intravenous antibiotic used to treat urinary tract infection and sepsis – which is a worrying trend. Further research and long-term data are required in order to scrutinise the causes of antibiotic resistance patterns and inadequacies, aiming to prevent the exponential increase in one of current medicine’s most dangerous problems.
Footnotes
Author contributions
SYT collected and analysed the data. SYT wrote the first and final drafts. ZJG and JED edited. All authors reviewed the results and approved the final version.
Conflict of interest statement
The author(s) declare that there is no conflict of interest.
Funding
The author(s) received no financial support for the research, authorship, and/or publication of this article.
Ethical approval
This study was approved by our ‘Clinical Governance and Audit’ team as our institution does not require ethical approval for reporting retrospective fully-anonymised case series. There were no other ethical concerns from the study.