
Abstract
Introduction and objectives:
Stress urinary incontinence (SUI) and recurrent urinary tract infections (RUTIs) are highly prevalent diseases. Our purpose was to investigate the relationship between RUTIs and surgical correction of SUI with transobturator suburethral tape (TOT) and to describe the benefit gained from a sublingual polibacterial preparation on RUTIs developed after TOT.
Materials and methods:
A retrospective study was performed on 420 women who underwent TOT surgery due to SUI between April 2003 and October 2011. Group A: patients without urinary tract infections (UTIs) before TOT (n = 294). Group B: patients with UTIs before TOT (n = 126). Variables: age, personal history, number of UTIs/month prior to and after surgery, appearance of urgent urinary incontinence (UUI) with or without UTIs, response to International Consultation on Incontinence Questionnaire Short Form (ICIQ-SF) and Short Form 36 (SF-36) questionnaires.
Results:
Group A: 85% dry; 5% UUI; 4% de novo UTIs with good response to antibiotics over 6 days. No RUTIs during the follow-up period, 2% with sporadic UTIs. Group B: 47.61% RUTIs; 52.39% sporadic UTIs; greater incidence of diabetes mellitus (p < 0.0025) and smoking (p < 0.0031) than group A. After TOT: 79.36% dry; 10% RUTIs. After treatment with antibiotics for 6 days and bacterial preparation for 3 months, 82% of patients did not have a UTI anymore. Postoperative cystourethrogram revealed 38% of nondiagnosed cystoceles before TOT. No patient had a postvoiding volume greater than 100 cm3 after TOT. Improvement of ICIQ-SF (p < 0.001) and SF-36 (p < 0.0004) in both groups.
Conclusion:
After eliminating bias associated with the tape, the technique and the surgeon’s skills, SUI correction may decrease the number of UTIs and improve the quality of life. UTIs disappeared in 82% of patients with RUTIs after TOT.
Introduction
Stress urinary incontinence (SUI) and urinary tract infections (UTIs) are two problems with a high prevalence in women, which cause a decrease in quality of life, may have severe, even mortal complications, and are a high-magnitude social problem both because of the economical expense and associated sick leave.
Despite the coexistence of these two diseases in multiple patients, there are no publications which determine the benefits that SUI surgical correction with the transobturator suburethral tape (TOT) procedure bring to women with SUI and recurrent UTIs (RUTIs) in terms of the resolution or low frequency of UTI episodes.
There is a lack of data supporting the hypothesis that UTIs may be caused by the uncovering of a preoperatory hidden cystocele or other factors associated with the TOT procedure, eliminating technical and local problems, such as extrusion of the mesh and others.
Our aim was to investigate the relationship between SUI and UTIs, and the effect of the TOT procedure on this relationship, in two comparable groups using the same tape brand, the same surgical team, the same technique and the same surgical protocol. We also report the results of treatment of RTUIs developed after TOT using a sublingual polibacterial preparation.
Materials and methods
We performed an observational retrospective study on 420 women who underwent TOT surgical treatment due to SUI between April 2003 and October 2011. Of the 632 women who underwent TOT surgery by the same clinical indication during this period, we only included those who had intervention with the tape Kim System (Neomedic International, Calatayud, Spain). The exclusion criteria were the simultaneous diagnosis of cystocele, colpocele, rectocele, urinary lithiasis or neurogenic urinary bladder, and TOT with other tapes. All surgeries were executed by the same surgical team and the same protocol. Women underwent surgery with the TOT technique under a short stay surgery regimen, using Kim System tape with in–out surgery, leaving the tape without being cut at an inguinal level until review 48–72 h after the surgery to allow a deferred readjustment of the tape whenever necessary.
After applying these criteria, two study groups were established: group A included patients with SUI without RUTIs prior to TOT (n = 294); group B included patients with SUI with RUTIs prior to TOT (n = 126). Personal history, general physical examination, complete urological examination, gynecological examination, or if not, a report given by the department of gynecology, were performed in all patients. In addition, two specific questionnaires that are validated internationally [International Consultation on Incontinence Questionnaire Short Form (ICIQ-SF) and Short Form 36 (SF-36), respectively] for SUI and quality of life related to health were completed at the first visit (before surgery), and at 1, 3 and 12 months after TOT. All patients had the following tests: blood biochemistry, complete blood count, urine (biochemistry and culture) and urine cytology and cystoscopy in cases of macro- or microhematuria. When there was clinical suspicion of SUI, cystocele, vesicourethral reflux and other pathologies, urodynamics study and intravenous urography were performed.
Following the recommendations of the European Association of Urology [Naber et al. 2001; Grabe et al. 2014], sporadic UTI was defined as an infection with less than two episodes every 6 months, and RUTI was defined as an infection that occurs more often than twice in 6 months.
The studied variables were age; UTIs prior to surgery; obstetric and pathological (including urologic) clinical history; number of monthly UTIs after surgery (controls were done monthly, at 3 months, 12 months and then every year); UTI treatment: empiric or according to antimicrobial susceptibility test, type of antibiotic, dose and plan; answers to questionnaires during the first visit and follow ups.
The results were analyzed with descriptive statistics, Student’s t test, χ2, Fisher’s exact test, analysis of variance (with Scheffe’s test for normal samples and Kruskal–Wallis for other distributions), Pearson’s and Spearman’s correlation studies. p < 0.05 was accepted as statistically significant. Analyses were done by the automatic statistic calculator NSSS2006/GESS2007 and Pearson Product Moment Correlation – Ungrouped Data (Server ‘Herman Ole Andreas’ Wold @ wold.wessa.net; ‘Gwilym Jenkins’ @ jenkins.wessa.net; Server ‘George Udny Yule’ @ yule.wessa.net; Server Gertrude Mary Cox @cox.wessa.net).
The study protocol was evaluated and approved by the Investigation Committee of the University Hospital of Salamanca.
Results
The average age of group A was 63.64 years [standard deviation (SD) 12.89] and that of group B was 62.78 years (SD 13.39), a difference which is not statistically significant (p = 0.56). We did not find differences in the gynecological and obstetric background of the patients between groups.
Following the definitions included in the ‘Materials and methods’ section, patients in group B who had RUTIs before surgery were older (p = 0.0005) than those who had sporadic UTIs. The average age of the RUTI subgroup was 60.88 years (SD 12.61) and the sporadic UTI was 50.80 years (SD 19.77). Patients with sporadic UTIs represented 52.93% of group B, while 47.61% of patients had RUTIs. In group A no RUTIs were associated with SUI as this is the characteristic which defines the group.
Group B patients with RUTIs had a clear predominance of infections with Escherichia coli (73.28), followed by Streptococcus agalatiae (4.90%), Proteus mirabilis (3.92%) and Enterococcus faecalis (3.92%). A wide variety of germs, including reclassified species of Klebsiella, such as Raoultella planticola, were also found in urine cultures (Table 1).
Results from positive urinary cultures (UC+) in samples from patients with RUTIs belonging to group B.
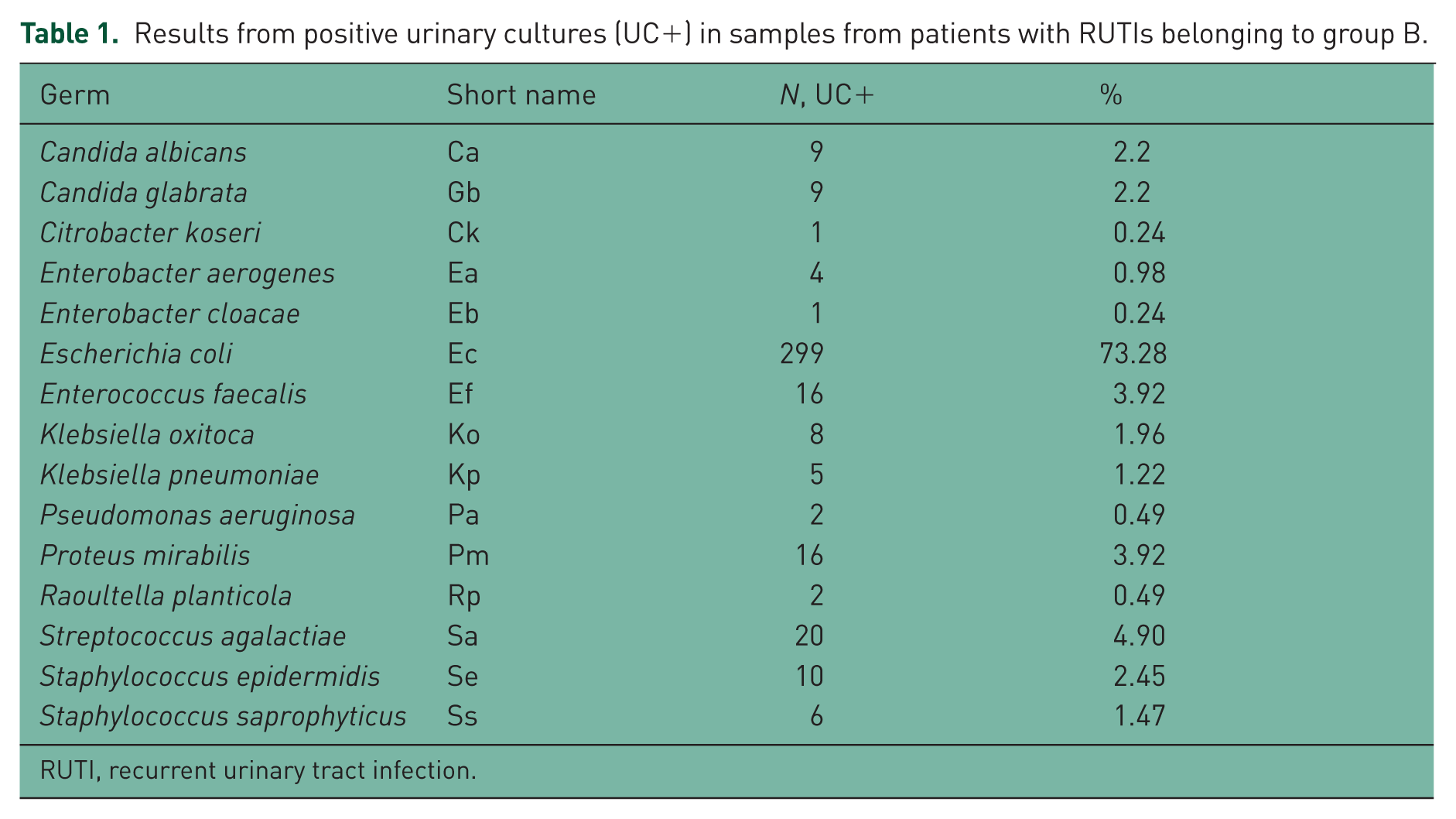
RUTI, recurrent urinary tract infection.
In group B we found a higher prevalence of diabetes mellitus (15.87%) than in group A (8.16%) (p = 0.0234). Smoking habit was also higher in group B (8.84% in group A versus 23.02% in group B) (p = 0.0019). After surgery, oral antibiotic treatment (oral ciprofloxacin 500 mg twice daily or trimethoprim 160 mg/sulfamethoxazole 800 mg) was administered for 6 days to patients with sporadic UTIs. In those with RUTIs, besides the first antibiotic course, a polibacterial vaccine (Uromune Inmunotek, Madrid, Spain) was added for 3 months. The vaccine consists of a suspension of inactive strains of E. coli (25%), K. pneumoniae (25%), P. mirabilis (25%) and E. faecalis (25%), in a concentration of 109 bacteria for each milliliter, with sublingual spray administration. The dosage is two spray pulses per day (1 ml per pulse). In 82% of cases, UTIs disappeared and 8% of sporadic UTIs were detected during the whole period of the study. In etiologic investigation of UTIs, seriated mictional cystourethrography (SMCU) was done, revealing a descent of the urinary bladder in 38% of women; most of them, cystoceles grade I–II, were not diagnosed prior to intervention although previous ultrasound and SMCU studies had been performed. No patient had a postvoiding volume greater than 100 cm3 after TOT.
In all patients from group A, a combination of amoxicillin and clavulanic was administered after the surgery, at an oral dose of 875 mg three times a day for 7 days, except in the case of allergy or intolerance (mostly because of diarrhea), in which case ciprofloxacin at an oral dose of 500 mg twice a day for 7 days or fosfomycin at an oral dose of 1 g three times a day for 7 days was administered. After these 7 days of treatment, UTIs appeared in 4% of patients (n = 12) between weeks 1 and 3 after surgery. Patients responded positively to antibiotic treatment over 6 days. In eight cases treatment was administered in an empiric form and in four cases, according to an antimicrobial susceptibility test. In patients with diabetes, intramuscular gentamicin, 80 mg/day, was administered for 4 days. Patients did not develop RUTIs, as confirmed during follow ups at 3 and 12 months and then annually. Sporadic UTIs were detected in 2% of patients during the whole period.
Table 2 shows the surgical success in treating urinary incontinence in groups A and B, as well as SUI and urge urinary incontinence (UUI) in each group. Significant differences between the two groups were not found (Table 2).
Surgical success and percentages of SUI and UUI in groups A and B.

SUI, stress urinary incontinence; UUI, urge urinary incontinence; postS: post-surgical.
The cases with miccional urgency were treated as follows: anticolinergic for 3–6 months: oral tolterodine 4 mg once daily; oral solifenacin 5 or 10 mg once daily; oral amitriptyline in combination with perphenazine (Mutabase 2/25; Schering, Plough, USA); or intrabladder injection of 100 units of botulinum toxin in cases of severe UUI.
Figures 1 and 2 respectively show the responses to the questionnaires assessing quality of life (ICIQ-SF and SF-36) before and after surgical treatment with TOT in groups A and B.
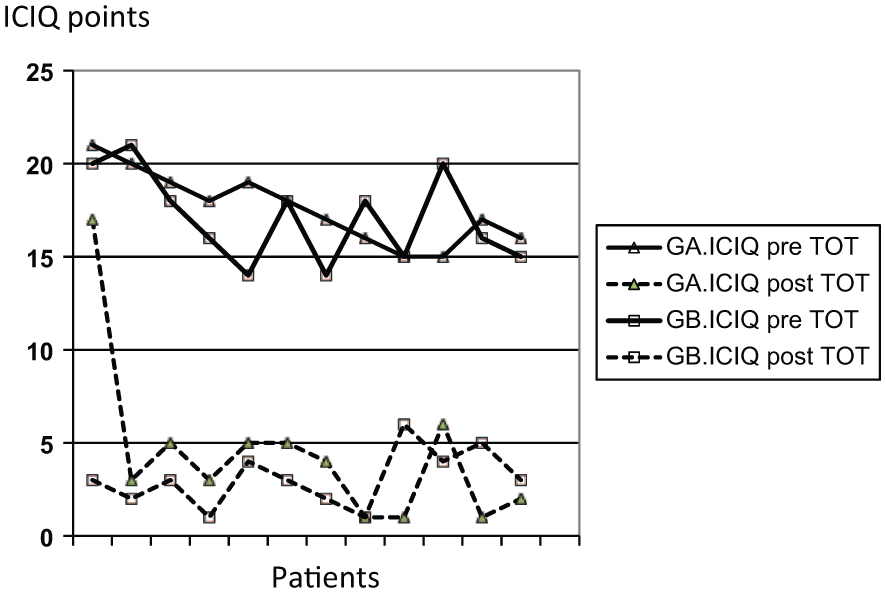
Responses to International Consultation on Incontinence Modular Questionnaire Short Form (ICIQ-SF) before and after surgical treatment with TOT in groups A and B. GA, group A; GB, group B; TOT, transobturator suburethral tape; CV, quality of life.

Responses to Short Form 36 (SF-36) before and after surgical treatment with TOT in groups A and B. GA, group A; GB, group B; TOT, transobturator suburethral tape. CV quality of life
Discussion
Urinary incontinence has been calculated to affect around 5–69% of the female population and around 1–39% of the male population [Irwin et al. 2006]. Many patients delay consultation with a doctor because of embarrassment, because they are prudish or because they believe that urinary incontinence is an ageing natural process. Therefore, at least 25% of patients take 5 years before they have a consultation [Norton et al. 1988].
In our study, group A has a higher average age compared with group B, although it does not reach statistical significance. According to different prevalence studies, UTIs with few symptoms or asymptomatic bacteriuria are present in 10–15% of women from 65 to 70 years, 15–20% of women older than 80 years, 30–40% of elderly women hospitalized or in geriatric institutions, and 100% of women with permanent urinary catheter [Andreu and Planells, 2008; Grabe et al. 2014].
RUTIs are frequent in healthy women without any anomaly of the urinary tract, who show symptomatic cystitis that appears to occur in bouts. Frequently young women without any risk factors with RUTIs have a nonsecretor serotype of blood groups and show two unique globosides in the membranes of epithelial cells: sialosilgalgloboside and disialosilgalgloboside, which do not appear in women with secretor serotype and act like uropathogenic E. coli receptors [National Kidney and Urologic Diseases Information Clearinghouse, 2011]. In these women most recurrences are produced by the same E. coli strain (carrying pap-encoded adhesins) [Stapleton et al. 1998]. Between episodes, this strain can accumulate either in the intestine, as during these periods we can frequently find the reinfective strains in feces, or in the interior of the superficial cells of the urinary bladder, where they create biofilms or pods that may contain bacteria bathed in a matrix rich in polysaccharides and rounded by a uroplactine wrapping. In our research group, using the immunomodulator treatment, we want to prove the role of immunoglobulin A induced by the polibacterial vaccine against these biofilms or pods, once its clinical efficacy is demonstrated [Lorenzo-Gómez et al. 2013].
Antimicrobial prophylaxis to prevent RUTIs should only be considered after the patient has received information about the main causes of infection and behavioral modifications. Before initiating any type of prophylaxis regimen, eradication of the UTI should be confirmed with a negative urinary culture for 1–2 weeks after treatment. Continuous antimicrobial or postcoital prophylaxis should be considered to prevent noncomplicated recurrent cystitis in those women in whom antimicrobial measures for prevention have failed. Nowadays, the European sanitary authorities recommend using RUTI therapeutic strategies other than antibiotic administration [Grabe et al. 2014].
Surgical reparation of the prolapsed pelvic organs may lead to the start of postoperative symptoms of SUI which did not exist previously or that women did not report before. There are several methods of evaluating the possibility of this postsurgical incontinence before doing the intervention (urodynamics with pessary, manual reduction of the prolapse, using a speculum, etc.). The sensitivity of detecting hidden incontinence is different according to the technique used. Hidden incontinence detection in a presurgical study is usually associated with an increased percentage of postsurgical incontinence, but this relationship is not absolute [Visco et al. 2008]. Some of our patients were readmitted for urinary incontinence consultation after showing this symptom as a consequence of postsurgical correction of genital prolapse, mostly after hysterectomy, with or without adnexectomy [Collazos-Robles et al. 2013].
Questionnaires to objectify data about subjective issues that affect the patient and from which we can only obtain information by talking about them are highly recommended. They are not only useful for the patient’s clinical evaluation but also for their monitoring. Questionnaires are designed to assess specific aspects of patients, such as inferior urinary tract symptoms, urinary incontinence, quality of life, psychological alterations due to urinary symptoms, sexual disturbances due to urinary symptoms, among others. It is necessary to use validated questionnaires for the language we will be using. Usually questionnaires are compiled to be completed by the patient autonomously [Alonso et al. 1995; Espuña-Pons et al. 2004]. When we find a successful treatment for both SUI and RUTIs, a significant improvement of quality of life is shown in the questionnaires of these patients.
Although evaluation of the upper urinary tract is not necessary in patients with non-neurogenic urinary incontinence, we performed a bilateral renal and bladder ultrasound examination in each patient in our study groups. We found two renal carcinomas and four cases of lithiasis susceptible to lithotripsy, curiously in patients who did not have RUTIs. These patients were not included in the present study. We took into consideration the treatment of lithiasis prior to the correction of incontinence to prevent possible difficulty in expelling the stones due to the increase in urethral resistance that usually occurs with TOT surgery [Athanasiou et al. 1999; Robinson et al. 2002]. We did not perform a voiding cystourethrogram as a routine diagnosis technique, only if we suspected cystocele or other bladder or urethral factors which could lead to the diagnosis of complicated female urinary incontinence.
Conclusion
In women who were treated with TOT because of SUI, after eliminating bias associated with the tape brand, the technique and the surgeon’s skills, SUI correction decreased the number of UTIs compared with previous surgeries in 82% of patients. In addition, we identified 4% of short-term de novo infections and 8% of long-term infections, excluding the perisurgical period.
The surgical correction of SUI with TOT is more successful (dry patients) in women without concomitant UTIs (85%) than in those who do have concomitant UTIs (79.36%), although this is not a significant difference.
UTIs resolved in 82% of patients with previous RUTIs after performing TOT.
Footnotes
Acknowledgements
MFLG: project development, data analysis, manuscript writing; RECR: data collection, state-of-the-art revision; AJVR: data collection; MBGC: data analysis; JAMC: data analysis; BPF: project development, data management, manuscript writing and editing.
Funding
This research received no specific grant from any funding agency in the public, commercial, or not-for-profit sectors.
Conflict of interest statement
The authors declare no conflicts of interest in preparing this article.