
Abstract
Urinary tract infections (UTIs) are the most common outpatient infections, with a lifetime incidence of 50−60% in adult women. This is a narrative review aimed at acting as an introduction to the epidemiology and burden of UTIs. This review is based on relevant literature according to the experience and expertise of the authors. The prevalence of UTI increases with age, and in women aged over 65 is approximately double the rate seen in the female population overall. Etiology in this age group varies by health status with factors such as catheterization affecting the likelihood of infection and the pathogens most likely to be responsible. In younger women, increased sexual activity is a major risk factor for UTIs and recurrence within 6 months is common. In the female population overall, more serious infections such as pyelonephritis are less frequent but are associated with a significant burden of care due to the risk of hospitalization. Healthcare-associated UTIs (HAUTIs) are the most common form of healthcare-acquired infection. Large global surveys indicate that the nature of pathogens varies between the community and hospital setting. In addition, the pathogens responsible for HAUTIs vary according to region making adequate local data key to infection control. UTIs create a significant societal and personal burden, with a substantial number of medical visits in the United States every year being related to UTIs. European data indicate that recurrent infections are related to increased absenteeism and physician visits. In addition, quality of life measures are significantly impacted in women suffering from recurrent UTIs. Data suggest that nonantimicrobial prophylactic strategies offer an opportunity to reduce both the rate of UTIs and the personal burden experience by patients.
Introduction
The following narrative review is based on presentations from the 2° Foro en Infecciones Urinarias Recurrentes (FIUR2) symposium, a Latin American forum to discuss current trends and challenges in treating recurrent urinary tract infections (UTIs). The literature herein was compiled based on a nonsystematic review of the current literature and the expertise of the authors/presenters.
Understanding the different classifications of UTIs is essential when considering their epidemiology. Broadly, UTIs are classified based on their location in the urinary tract, the presence of relevant complicating factors, and the presence or absence of symptoms. Definitions of some of the major categories of UTIs, based on the most recent German guidelines, are summarized in Table 1. 1
Key classifications of UTIs. 1
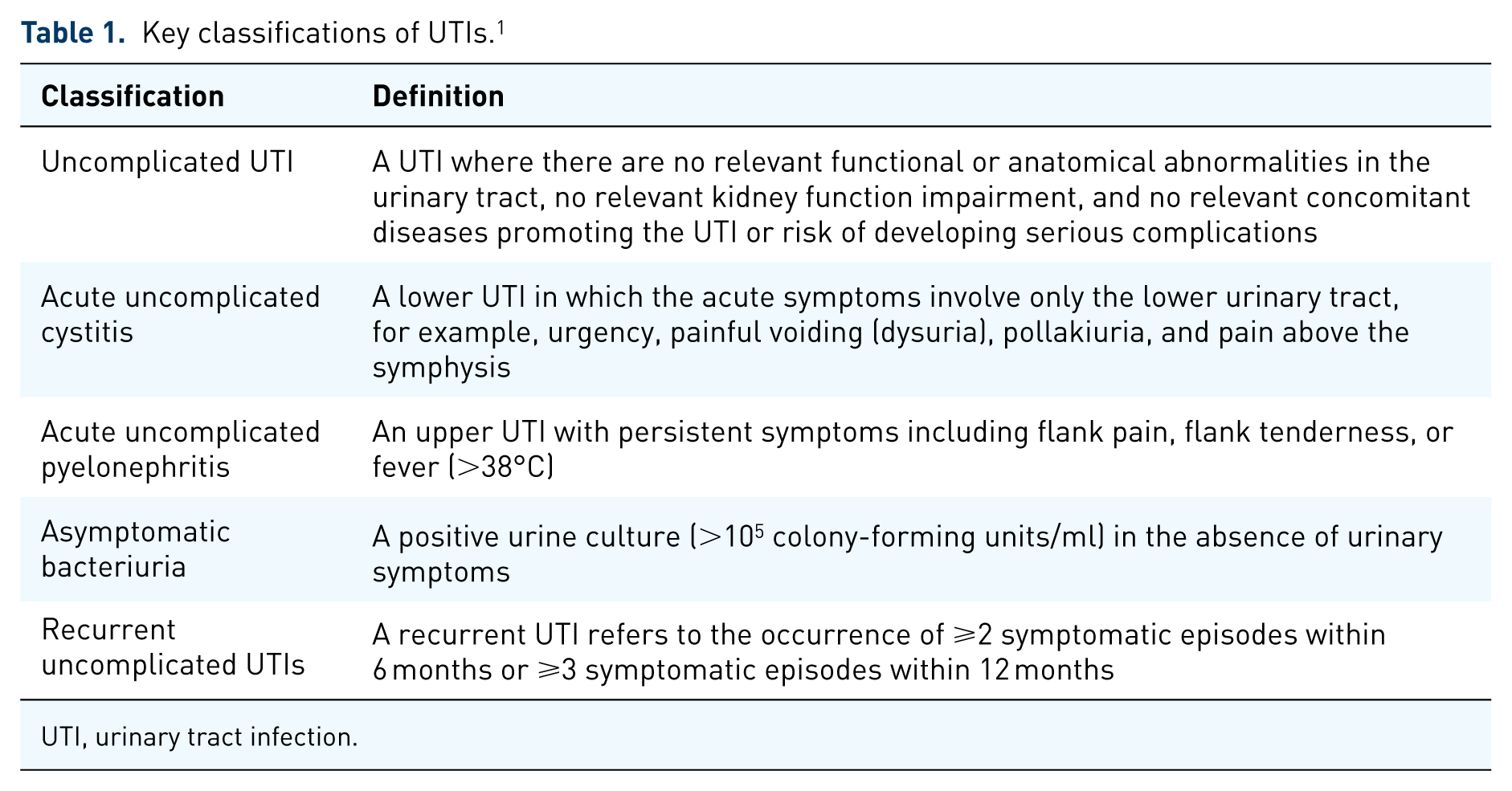
UTI, urinary tract infection.
UTI epidemiology
Uncomplicated UTIs
UTIs are the most common outpatient infections in the United States (US). With the exception of a spike in young women aged 14−24 years old, the prevalence of UTIs increases with age. 2 The prevalence in women over 65 years of age is approximately 20%, compared with approximately 11% in the overall population. 3 Between 50% and 60% of adult women will have at least one UTI in their life, and close to 10% of postmenopausal women indicate that they had a UTI in the previous year. 4
Etiology in older postmenopausal women varies depending on their health status, residential status (institutionalized or not), age, the presence of diabetes mellitus, history of/current catheterization, spinal cord dysfunction, and a history of antibiotic use. Most UTIs in noncatheterized older adults are caused by a single bacterial species. However, in the presence of structural abnormalities and catheterization, it is not unusual to isolate more than one species in the urine culture. The increased use of catheters and instrumentation in these patients predisposes them to UTIs caused by Gram-negative rods such as Proteus, Klebsiella, Serratia, and Pseudomonas. In patients with diabetes mellitus, infections caused by Klebsiella, Enterobacter, and Candida are more common.
The frequency of uncomplicated cystitis in young sexually active women in the US is approximately 0.5 episodes per person per year. The peak rate of uncomplicated UTIs occurs during the years of maximum sexual activity, usually between the ages of 18 and 39. Uncomplicated recurrent UTIs are also frequent in young women. After a first episode of a UTI, 27% of women have a confirmed recurrence within the next 6 months, and 2.7% have a second recurrence within the same period of time. 4
There are an estimated 250,000 cases of pyelonephritis annually in the US, with a higher frequency among females. In women aged 18−49 years, the estimated incidence of pyelonephritis is 28/10,000; 7% of cases require hospital admission. Cultural and genetic factors may influence prevalence (e.g. in South Korea 59/10,000 patients experience pyelonephritis). Recurrence is less common than with uncomplicated UTIs, with 9% of females and 5.7% of males having a second episode within a year. 4
Uropathogenic Escherichia coli (E. coli) (UPEC) is the dominant infectious agent in both uncomplicated and complicated UTIs. Enterococcus spp. and Candida spp. are substantially more common in complicated infections, while Staphylococcus saprophyticus (S. saprophyticus) is rare (Table 2). 5 Infection with UPEC increases the likelihood of recurrence within 6 months. 4
Epidemiology of infectious agents in uncomplicated and complicated UTI. 5

Healthcare-associated UTIs
Infectious complications following urological procedures are a major issue, particularly in the context of increasing antimicrobial resistance. Over 4 million patients acquire healthcare-associated infections in the European Union every year, 20−30% of which are considered preventable. Healthcare-associated UTIs (HAUTIs) represent the largest subtype among all healthcare-associated infections. The prevalence of HAUTIs assessed in regional studies ranges from 12.9% in the US and 19.6% in Europe, to up to 24% in developing countries.6–8
The large, ongoing Global Prevalence Study on Infections in Urology (GPIU study) aims to gain a global perspective on HAUTIs. Between 2003 and 2010, 19,756 patients were assessed, 9.4% of whom were diagnosed with a HAUTI (70.4% of whom were female). The mean age of the study group was 59 years, and 75% of UTIs were diagnosed via urine culture. Asymptomatic bacteriuria (ABU) was the most common diagnosis (27%), followed by cystitis (26%), pyelonephritis (20%), and urosepsis (10%). The dominant pathogen in all conditions was UPEC (39.7%), although it made up a lower proportion than in UTIs in general (Table 2); Enterococcus spp. (11.5%), Klebsiella spp. (11.1%), and Pseudomonas aeruginosa (P. aeruginosa) (10.8%) comprised approximately one-third of infections. 9 An Asian substudy of GPIU (n = 6707) underlined some regional differences: while the overall prevalence was similar (9.8%), the breakdown of UTIs classifications differed; pyelonephritis was the most common diagnosis (30.7%), followed by cystitis (29.9%), ABU (17.9%), and urosepsis (11.1%). 10
Prevalence of UTIs in Latin America
Overall, regional data for Latin America are currently lacking. In a Colombian study including 226 pregnant women, ABU was found in 10.6% of participants; UPEC was the most common pathogen (25%), followed by Enterococcus faecalis (E. faecalis) (20.8%). 11 Another Columbian study showed a prevalence of acute UTIs for women and men, respectively, of 23.3% and 6.8%, and a prevalence of recurrent UTIs of 54.2% and 15.7%, respectively. 12 In a third Colombian study (n = 1959), UTI prevalence was 31%, and the major causative agents were E. coli (69%), Enterococcus spp. (11%), and Klebsiella spp. (8%). 13
A small Argentinian study (n = 87) examined HAUTIs (48% of participants) and community-acquired UTIs (52% of participants). Again, UPEC was more common in the community-acquired UTI group (74%) than in the HAUTI group (47%). Klebsiella pneumoniae (K. pneumoniae) and E. faecalis infection rates were 12% versus 20% and 5% versus 7% in the community and healthcare settings, respectively. 14
The burden of recurrent UTIs
The burden of recurrent UTIs has both personal and societal aspects. The societal burden includes the clinical and economic burden of the illness, and the personal burden includes social and psychological effects which have a negative impact on quality of life (QoL). The high prevalence of recurrent UTIs represents a modifiable determinant for both societal and personal burdens, hence the importance of disease prophylaxis. Consultations for UTIs represent between 1% and 6% of all medical visits (~7 million visits and ~US$1.6 billion annually). They are associated with a significant burden of morbidity and mortality in the elderly, among whom UTIs are most prevalent.15,16
Recurrent UTIs are associated with symptoms of anxiety and depression. The sudden, rapid, and painful onset of a UTI is often a source of anxiety in patients. Feelings of guilt related to a patient’s inability to perform their usual activities, or the impact of recurrent infections on their social activities, may lead to clinical symptoms of depression. The social impact of recurrent UTIs may be particularly marked in premenopausal, working women. Treatment of a UTI alone is often not enough to improve a patient’s QoL. However, the often-neglected impact of therapy on QoL should be considered as part of treatment efficacy. In the elderly, the potential for a substantial impact on general health, including issues such as incontinence, is also associated with a significant psychological burden. 17
The personal and societal impacts of recurrent UTIs often overlap. For example, in cases where multiple urine cultures or imaging studies may be required, the diagnostic burden both affects QoL and has a substantial negative economic impact. Costs may be both direct and indirect: work absenteeism, for example, can impact both the economy and a patient’s sense of wellbeing. Costs include those associated with medical visits (for ambulatory patients), prescriptions for antimicrobials, hospital expenses, nonmedical travel-related costs, days of sick leave due to the disease, and the treatment of related comorbidities.
The recent multinational web-based GESPRIT study assessed both the personal and economic burden of recurrent UTIs in Europe (Germany, Switzerland, Poland, Russia, and Italy). Adult women (⩾18 years of age) with a history of recurrent infection and who currently had an acute infection (n = 1275) or had suffered an infection within the previous 4 weeks (n = 666) completed an online questionnaire. Recurrent UTIs were associated with an economic burden due to both sick leave and physician visits. Participants also reported a significant impact on QoL as evaluated by the SF-12 v2 health survey. The majority of women surveyed (approximately 80%) reported having received treatment with antibiotics. Prophylaxis was frequently delayed beyond the point where recurrence was established (⩾3 UTIs in 12 months), and the behavioral measures used for prophylaxis were often ineffective. 18
Appropriate prophylaxis may have the potential to ameliorate the impact of recurrent UTIs on QoL. In a recently published open-label, multicenter, prospective trial, 699 patients with recurrent UTIs were assessed using the Hospital Anxiety and Depression Scale (HADS) and the Leicester Impact Scale which measures QoL in patients with urological problems. At trial entry, 61.9% of the patients exhibited some degree of depression. Participants received prophylaxis with the bacterial lysate OM-89 daily for 90 days. At the end of the 6-month study, the frequency of UTIs decreased by 59.3% (p ⩽ 0.0001), the total HADS score decreased by 32.1% (p ⩽ 0.0001), and the Leicester Impact Scale score decreased by 44.0% (p ⩽ 0.0001), compared with baseline measurements. 17 These data suggest that effective utilization of prophylaxis has the potential to ease the burden of UTIs on both individual patients and society.
Conclusion
UTIs remain one of the most common forms of infection both in the community and, particularly, within the healthcare setting. HAUTIs are of significant concern and cause a substantial personal and societal burden due both to their prevalence, and to the ability of microbes to share resistance mechanisms. Studies focusing on understanding regional differences in UTI epidemiology are necessary, particularly in Latin America, where there is currently a paucity of data. The burden of UTIs on both individuals and society is multifactorial and is likely to increase in the context of antibiotic resistance. Both regional and national studies on the burden of UTIs remain an unmet need in Latin America.
Footnotes
Acknowledgements
Writing assistance was provided by Mariella Franker, PhD, Franker Medical Communications, Netherlands, and Ewen Legg, PhD, Halcyon Medical Writing Ltd., UK.
Funding
The symposium was organized and funded by Vifor Pharma Group, Switzerland. Writing assistance was funded by OM-Pharma, a company of Vifor Pharma Group. This supplement was supported by an educational grant from OM-Pharma.
Conflict of interest statement
Dr Medina and Dr Castillo-Pino have acted as a speaker for the Vifor Pharma Group.