
Abstract
Background:
The prognostic significance of resting heart rate (HR) in acute ischemic stroke (AIS) patients with large vessel occlusion (LVO) after endovascular treatment (EVT) remains to be elucidated.
Objectives:
To determine whether HR is differentially associated with functional outcomes in patients dichotomized by anterior (ACS) or posterior circulation stroke (PCS) after successful reperfusion.
Design:
A multicenter retrospective cohort study.
Methods:
We retrospectively analyzed consecutive successfully recanalized LVO-AIS patients with complete HR recordings at admission, 30 min, 12 h, 24 h, and 48 h post-EVT. A good outcome was defined as modified Rankin Scale (mRS) 0–2 for ACS or mRS 0–3 for PCS at 3 months. Binary logistic regression and receiver operating characteristic analyses were used to assess associations and predictive performance.
Results:
Among 505 patients (362 ACS, 143 PCS), lower HR at 12, 24, and 48 h post-EVT was independently associated with good outcomes in both groups. HR showed higher predictive accuracy for PCS (AUC: 0.872–0.885) than for ACS (AUC: 0.732–0.762).
Conclusion:
HR following EVT independently predicts functional outcome in LVO patients, demonstrating stronger predictive value for PCS than ACS. These results highlight the potential of HR monitoring in post-EVT management.
Introduction
Stroke poses a significant global health burden due to its high rates of incidence, disability, mortality, and recurrence. 1 For patients with acute ischemic stroke (AIS) caused by large vessel occlusion (LVO), endovascular treatment (EVT) has become the most effective therapeutic approach, substantially improving clinical outcomes.2,3 The brain-heart interaction, often manifested as brain-heart syndrome, is a well-recognized phenomenon that notably influences patient prognosis after stroke.4–6 In this context, heart rate (HR), a key prognostic marker in cardiovascular disease, has also been linked to stroke outcomes.7–9 Previous research has shown that elevated HR and increased HR variability are associated with higher risks of mortality and poor functional recovery after EVT in AIS-LVO patients.10,11 However, it remains unexplored whether the association between HR and clinical outcomes differs between anterior (ACS) and posterior circulation stroke (PCS) following EVT.
Due to anatomical distinctions, differential responses to thrombolysis and EVT, and distinct brain-heart interactions between ACS and PCS, we hypothesized that HR may be more closely associated with clinical outcomes in posterior versus anterior circulation stroke after EVT.
Methods
Patient selection
From the DETECT-China (Endovascular Treatment for Acute Ischemic Stroke in China) cohort, patients with AIS-LVO who achieved successful revascularization after thrombectomy were screened between February 2018 and February 2022 (NCT04752735). The inclusion criteria were: (1) age ⩾18 years; (2) successful recanalization via EVT within 24 h of onset; (3) pre-stroke modified Rankin Scale (mRS) score ⩽1. The following patients were excluded: (1) pre-stroke disability (mRS ⩾2); (2) unsuccessful recanalization (mTICI score 0–2a); (3) lack of 90-day mRS and complete HR data; (4) atrial fibrillation occurred when HR is recorded. We collected baseline characteristics, including demographic, medical history, and stroke risk factors, blood test results, clinical neurological scores (National Institutes of Health Stroke Scale (NIHSS), mRS), TOAST classification, neuroimaging data, EVT procedure data, and some critical clinical data. All patients underwent continuous electrocardiographic monitoring throughout hospitalization within 24 h following EVT. HR data were extracted from the electronic medical records as single measurements at baseline (pre-procedure) and at 30 min, 12 h, 24 h, and 48 h post-procedure.
Outcome measures
The primary outcome was a good outcome at 3 months, defined as mRS 0–2 at 90 days for ACS, and mRS 0–3 for PCS, respectively.
Statistical analysis
Categorical variables are presented as numbers (percentages), and continuous variables as mean ± standard deviation or median (interquartile range), based on their distribution. Group comparisons for continuous and categorical variables were performed using independent t tests, Mann–Whitney U tests, or Chi-square tests, as appropriate. Binary logistic regression was used to assess the association between HR at various timepoints and the primary outcome in ACS and PCS cohorts separately. Variables with p < 0.05 in univariate analyses were included in the multivariate models. The predictive performance of HR for functional outcome was evaluated using multivariable receiver operating characteristic (ROC) curve analysis, with the optimal cutoff determined by the Youden index. A two-sided p < 0.05 was considered statistically significant. All analyses were conducted using IBM SPSS Statistics version 27.0 (IBM Corporation, Armonk, New York, United States) and R version 4.4.0 (R Foundation for Statistical Computing, Vienna, Austria). The completed checklist is available as Supplementary Material.
Results
From February 2018 to February 2022, 1000 consecutive patients were screened. After excluding 186 patients with unsuccessful reperfusion (mTICI score 0–2a), and 138 patients with incomplete data about outcome, 151 patients with mRS ⩾2 before onset, 20 patients occurred atrial fibrillation when HR was recorded, 505 patients were included in the final analysis (Figure 1). Among these, 362 patients (71.5%) had ACS, and 143 patients (28.5%) had PCS.

Flowchart of the subject selection.
Of 362 ACS patients, 204 (56.4%) got a good outcome, while 57 patients (39.9%) got a good outcome in 143 PCS patients. Younger age, fewer postoperative intracerebral hemorrhage (ICH), lower admission NIHSS, higher Alberta Stroke Program Early CT Score (ASPECT), and slower HR at 12, 24, and 48 h after EVT were associated with a good outcome in ACS or PCS patients (Table 1). It is worth noting that HR within 30 min after EVT was obviously associated with clinical outcome in PCS (76.0 vs 84.0, p = 0.002), but not ACS (70.0 vs 74.5, p = 0.088, Table 1).
Baseline characteristics of 505 patients.

Data were expressed as n (%), mean (SD), and median (IQR).
BT, body temperature; DBP, diastolic blood pressure; DPT, door-to-puncture time; EVT, endovascular treatment; HR, heart rate; ICH, intracerebral hemorrhage; LAA, Large-artery atherosclerosis; NIHSS, National Institutes of Health Stroke Scale; OPT, onset-to-puncture time; ORT, onset-to-reperfusion time; pc-(ASPECTS), posterior circulation-(Alberta Stroke Program Early CT Score); SBP, systolic blood pressure.
Figure 2 shows that the probability of a good outcome decreased significantly with increasing HR at 12, 24, and 48 h after EVT in ACS patients (p < 0.05), and with increasing HR within 30 min, at 12, 24, and 48 h after EVT in PCS patients (p < 0.05). Multivariable logistic regression analysis revealed that, after adjusting for potential confounders (age, diabetes mellitus, NIHSS, ASPECTS, and intracerebral hemorrhage in ACS patients; age, NIHSS, pc-ASPECT, atrial fibrillation, body temperature (BT) in PCS patients), good outcome in ACS patients was independently associated with lower HR at 12, 24, and 48 h after EVT with best cutoff values of 81.5, 80.5, and 82.5 bpm, respectively (Table 2); whereas in PCS patients, good outcome was associated with lower HR at 12, 24, and 48 h after EVT with best cutoff values of 85, 82.5, and 87 bpm, respectively (Table 2). All included variables had variance inflation factors below 10, indicating no significant multicollinearity. Earlier postprocedural HR (30 min after EVT) may be more associated with clinical outcomes in PCS compared to the anterior circulation, though statistically nonsignificant (p = 0.067).

Probability of good functional outcome with HR.
Multivariable logistic regression analyses for the association of HR with the clinical good outcome.

Adjusting for age, NIHSS, ASPECTS, DM, and ICH in anterior circulation stroke, and age, NIHSS, pc-ASPECT, atrial fibrillation, and body temperature in posterior circulation stroke.
ASPECTS, Alberta Stroke Program Early CT Score; CI, confidence interval; DM, diabetes mellitus; EVT, endovascular treatment; HR, heart rate; ICH, intracerebral hemorrhage; NIHSS, National Institutes of Health Stroke Scale; OR, odds ratio; pc-ASPECT, Posterior Circulation Alberta Stroke Program Early CT Score; ROC, receiver operating characteristic.
In multivariate ROC analysis, HR was used to construct the model by adjusting for age, diabetes mellitus, NIHSS, ASPECTS, and ICH in ACS or age, NIHSS, atrial fibrillation, BT, and pc-ASPECT in PCS patients. The results showed that the HR exhibited better predictive ability for good outcome in PCS versus ACS (AUC: 12 h after EVT: 0.872 vs 0.741, 24 h after EVT: 0.885 vs 0.732, 48 h after EVT: 0.877 vs 0.762; Figure 3).
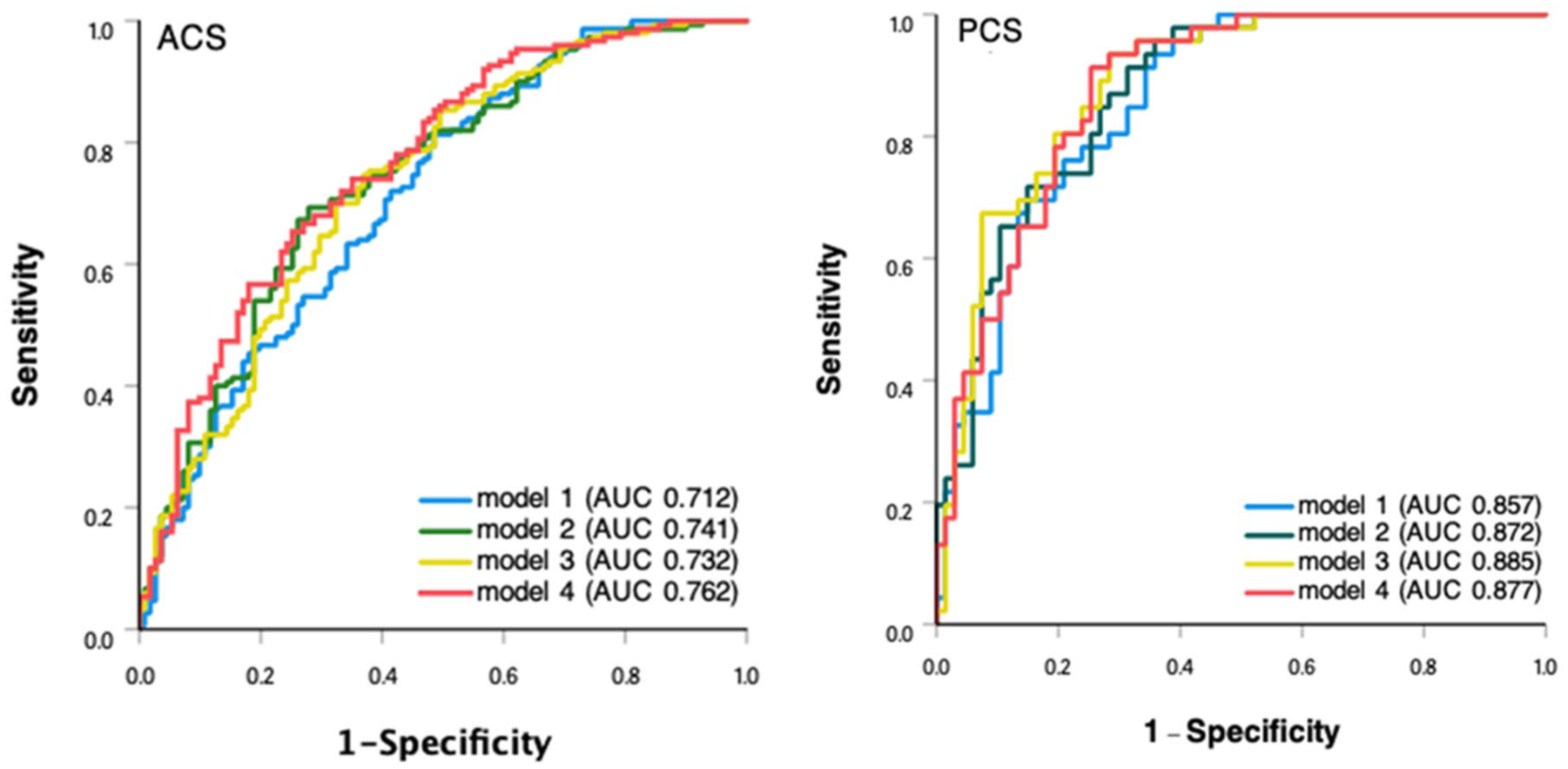
ROC analysis. Anterior circulation stroke: model 1 was adjusted for age, NIHSS, ASPECTS, DM, and ICH. Posterior circulation stroke: model 1 adjusted for age, NIHSS, AF, BT, and pc-ASPECT. Models 2, 3, and 4 were sequentially developed by incorporating postoperative heart rate measurements at 12, 24, and 48 h, respectively, as additional parameters to the baseline model 1.
Discussion
To our knowledge, this is the first study to examine the association between post-EVT HR dynamics and functional outcomes in AIS-LVO patients, stratified by anterior versus posterior circulation involvement. We found that HR after EVT was an independent predictor of clinical functional outcome in AIS-LVO patients with successful recanalization after EVT, with stronger predicting performance for PCS. Collectively, the current findings suggest the potentially distinct association of HR after EVT with clinical outcome in ACS versus PCS patients with successful reperfusion. Early strict control of HR after EVT may be a potential treatment strategy for AIS-LVO patients with successful reperfusion, especially for PCS.
Previous studies have established a correlation between HR and outcomes in general AIS populations, linking lower baseline HR, 12 lower HR within 24 h post-thrombolysis, 13 and higher HR with long-term vascular events. 14 However, evidence specifically for AIS-LVO patients after EVT remains scarce, with existing reports primarily associating higher HR with mortality.10,11 Consistent with this, our study confirms that lower post-EVT HR predicts good functional outcome in successfully reperfused AIS-LVO patients. Importantly, we extended this finding by revealing critical differences between ACS and PCS. Specifically, earlier HR (within 30 min) post-EVT showed a potential association with outcome in PCS but not in ACS. Furthermore, HR demonstrated superior predictive performance for PCS (AUCs: 0.872–0.885) compared to ACS (AUCs: 0.732–0.762).
The mechanism of the correlation between HR and AIS outcome is still not completely clear. Several possible explanations have been proposed, such as increased HR induced by possible hypovolemia, 15 associated inflammation after stroke, 16 and higher BT,17,18 which may be attributed to poor outcome in acute stroke. In the current study, we argue that the anatomic difference may be involved, because higher HR after EVT was more closely associated with clinical outcomes in PCS versus ACS. It is well known that the cardiovascular center is localized to the medulla oblongata, and many nuclei in the brainstem maintain the dynamic balance of the autonomic nerve in the body,19–22 which may explain the higher HR occurring in PCS patients with poor outcomes. In addition, given that the thermoregulatory center located in the hypothalamus may be disturbed by PCS, 23 higher BT may be attributed to higher HR in patients with poor outcome, which was partially supported by the current results (poor vs good outcome, 36.6 vs 36.5, p = 0.005).
In AIS-LVO patients, an earlier HR increase after EVT often suggests autonomic dysfunction and intracranial hypoperfusion, potentially due to ischemia affecting brainstem-associated nuclei. 24 Previous studies25–27 have demonstrated that brainstem infarction is consistently associated with poorer outcomes. However, in ACS-LVO patients, the observed HR changes are more likely attributable to persistent postoperative intracranial hypoperfusion, impaired cardiac function, and systemic inflammatory responses, which may partially contribute to poor functional outcomes. In addition, the posterior circulation has fewer collateral pathways than the anterior circulation,28,29 while faster HR may compensate for less perfusion. These pathophysiological distinctions may collectively explain the superior predictive value of post-EVT HR in PCS. Conversely, the lack of association between pre-EVT HR and outcome in both cohorts suggests that elevated HR at this hyperacute phase likely represents a nonspecific, self-regulatory response to intracranial ischemia, rather than a determinant of long-term recovery.
The main strength was the first report that HR after EVT was independently associated with clinical outcome in LVO-AIS patients with successful reperfusion. Moreover, HR after EVT was a stronger predictor for clinical outcome in PCS than in ACS. These findings may provide insights for postoperative management and clinical trials in LVO-AIS patients after EVT, especially for PCS. For example, initiating beta-blocker therapy after EVT in PCS patients with higher HR (e.g., ⩾87 bpm) can be considered in clinical practice or be tested in future clinical trials, which was supported by some observational studies.30,31 We must acknowledge several limitations. First, as a retrospective study, our analysis was inherently constrained by the selection bias, introducing potential residual bias and unmeasured confounding factors. For example, a previous study 32 has confirmed that collateral status is an independent predictor of post-thrombectomy outcomes. However, the lack of standardized assessment data prevented its inclusion in our adjusted models. Second, a relatively small size was another limitation. For example, only 15 patients (HR ⩽ 45; 2.97%) in our study had bradycardia during HR recording, so we did not explore the relationship between severe bradycardia and patient outcome. Third, HR data came from routine clinical recordings rather than a standardized protocol, potentially limiting their hemodynamic interpretability. In addition, the lack of information on antiarrhythmic drug use further limited our analysis, as this constitutes a key confounding factor. Fourth, we excluded patients without successful recanalization after EVT, so this finding was not suitable in this population. Finally, the imbalance in the size of ACS versus PCS may make the conclusion less powerful.
Conclusion
This was the first report that HR after EVT was a good predictor for clinical outcome in LVO-AIS patients with successful reperfusion after EVT, and stronger predictive performance was found in PCS versus ACS.
Supplemental Material
sj-docx-1-tan-10.1177_17562864251413489 – Supplemental material for Heart rate and clinical outcome after endovascular treatment in patients with anterior versus posterior circulation large vessel occlusion
Supplemental material, sj-docx-1-tan-10.1177_17562864251413489 for Heart rate and clinical outcome after endovascular treatment in patients with anterior versus posterior circulation large vessel occlusion by Lu Zhang, Ying-Jia Wang and Hui-Sheng Chen in Therapeutic Advances in Neurological Disorders
Footnotes
References
Supplementary Material
Please find the following supplemental material available below.
For Open Access articles published under a Creative Commons License, all supplemental material carries the same license as the article it is associated with.
For non-Open Access articles published, all supplemental material carries a non-exclusive license, and permission requests for re-use of supplemental material or any part of supplemental material shall be sent directly to the copyright owner as specified in the copyright notice associated with the article.