
Abstract
Background:
Hyperglycemia has been considered a predictor of stroke outcomes. In this article we study the correlation between blood glucose levels within the first 24 h after stroke onset and patients’ outcomes in mortality and hemorrhagic transformations.
Methods:
Ninety-one non-diabetic patients with acute ischemic stroke admitted to a neurological intensive unit were recruited. Their blood glucose was measured twice within 6 h (baseline) and at every hour after stroke onset. Patients were collected into four groups as follows: those in which normoglycemia and no hyperglycemia were observed at either baseline or 24 h; those with baseline hyperglycemia and hyperglycemia only at baseline; those with 24 h hyperglycemia and hyperglycemia only at 24 h after stroke; and those with persistent hyperglycemia and hyperglycemia at both baseline and at 24 h. Endpoints were designated as the patient’s death within 30 days and/or hemorrhagic transformation under computerized tomography within the first 7 days after stroke onset.
Results:
Persistent hyperglycemia was correlated with an increased risk of mortality within 30 days (OR = 24.0; 95% CI = 2.8–199.3) and it was also correlated with hemorrhagic transformation (OR = 13.3; 95% CI = 2.7–66.1). Baseline or delayed hyperglycemia were not correlated with any outcome.
Conclusions:
Persistent hyperglycemia was correlated with mortality after acute ischemic stroke.
Introduction
Hyperglycemia is commonly found in patients suffering acute ischemic stroke, with an incidence of approximately 40%.1–3 Acute hyperglycemia can increase infarct volume, 4 risk exposure of secondary hemorrhagic transformation 5 and reduce recanalization after intravenous thrombolysis, 6 thus leading to poor prognosis. Although meta-analyses indicate that acute hyperglycemia is correlated with in-hospital mortality after ischemic stroke and poor functional recovery in non-diabetic stroke survivors, 3 a case-controlled retrospective study with better glucose monitoring should be carried out in a clinical practice to further explore the correlation between hyperglycemia and prognosis after acute ischemia.
Up to now, most studies in this regard focused on fasting glucose upon admission without dynamic monitoring of blood glucose after admission, a means to provide much more and accurate information on the associations among blood glucose, early dynamic stroke pathology and patient outcomes. Hyperglycemia falls into three types. The first is diabetes pointing to chronic hyperglycemia; the second is newly diagnosed diabetes confirmed after discharge; and the third is hospital-related hyperglycemia that reverts to the normal range after discharge. 7 In this sense, dynamic information on blood glucose can help determine the exact type of hyperglycemia, correlating with outcome after ischemic stroke.
In the present study, we probed the correlation between hyperglycemia at different phases and mortality within 30 days, and occurrences of hemorrhagic transformations within 7 days. Our study will define the precise phase of hyperglycemia that contributes to poor prognosis, and indicate proper interventions in clinical practice.
Materials and methods
Patients
We conducted a prospective observational study of consecutive patients, with non-diabetic patients admitted for acute ischemic stroke between 1 September 2014 and 30 September 2016 at the neurological intensive unit (NCU) of Tiantan Hospital. Patients in the study met the following criteria: (1) an ischemic stroke proven by initial diffusion weighted imaging (DWI) or head computerized tomography (CT) scan; (2) admission within 72 h from symptom onset; and (3) an admission score on the National Institutes of Health Stroke Scale (NIHSS) between 5 and 25. Symptom onset was defined as the last time the patient was seen in normal health conditions. The exclusion criteria were life-threatening conditions that limited follow-up visits, or absence of plasma glucose levels at admission. Diabetes was acknowledged if the patients were discharged from a hospital with a diagnosis of type 1 or type 2 diabetes and received prescriptions for either insulin or an oral antidiabetic agent, and/or with HbA1c level ⩾6.5% during the preceding 2 months.
The protocol for this prospective study was reviewed and approved by the Ethics Committees of Beijing Tiantan Hospital, Capital Medical University (IRB of Beijing Tiantan Hospital affiliated to Capital Medical University, KY2016-026-02). Each participant was well informed and signed written consent before participating in this study.
Blood glucose measurement
Blood glucose measured upon admission within 6 h after stroke onset was used as the baseline. Blood glucose was measured again at 24 h after stroke onset. Hyperglycemia was defined as glucose level ⩾7.8 mmol/L. Patients were divided into four groups based on the phase patterns of hyperglycemia: (1) hyperglycemia at baseline only; (2) hyperglycemia at 24 h only; (3) persistent hyperglycemia with hyperglycemia at both baseline and at 24 h; and (4) persistent normoglycemia with normoglycemia at both baseline and at 24 h.
Outcomes evaluation
Outcomes were evaluated in two aspects. One is death within 30 days after treatment and the other is hemorrhagic transformations within the first 7 days. Hemorrhagic transformations were defined according to ECASS-II criteria. 8 Hemorrhagic infarction (HI) was defined as petechia without a space-occupying effect, ranging from small petechiae along the margins of the infarct (HI1) to a confluent petechia within the infarct area (HI2); parenchymal hemorrhage was defined as blood clots with space-occupying effect, either ⩽30% (PH1) or >30% (PH2).
Statistical analysis
Data are presented as medians with interquartile ranges for continuous variables or frequencies for discrete variables. Chi-squared or Fisher exact tests were applied for the categorical variables, and a two-sided non-parametric Kruskal–Wallis test was used for continuous variables in univariate analyses. Multifactorial logistic regression models were used to assess the correlation between hyperglycemia and final outcomes. Adjusted ORs were then obtained after adjustment for factors at the threshold probability value of 0.05 in univariate analyses. Significance was accepted if p < 0.05. Data analyses were performed with the SAS Statistical Analysis System20 (version 8.0).
Results
Patient characteristics
Of the 91 non-diabetic patients, 37 (40.6%) were normoglycemic; 4 (4.4%) were baseline hyperglycemic; 20 (22%) were hyperglycemic only at 24 h; and 30 (33%) were persistently hyperglycemic. Basic characteristics of all the patients are listed and compared in Table 1. In general, patients with persistent hyperglycemia had more severe neurological deficits, higher occurrence of atrial fibrillation histories, higher systolic pressure, higher HbA1c levels and higher white blood cell count.
Baseline characteristics of 91 patients without diabetes according to hyperglycemic patterns.

BNP, brain natriuretic peptide; BUN, urea nitrogen; Cr, creatinine; CRP, C reactive protein; HDL, high-density lipoprotein; LDL, low-density lipoprotein; NIHSS, NIH Stroke Scale; PLT, platelet; SBP, systolic blood pressure; TC, total cholesterol; TG, triglycerides; UA, uric acid; WBC, white blood cell.
Association of hyperglycemic patterns with stroke outcomes in univariate analyses
The stroke outcomes such as death within 30 days (p < 0.001, Table 2) and hemorrhagic transformation (p = 0.001, Table 2) were different between the four hyperglycemic patterns.
Univariate correlation between hyperglycemic patterns and outcomes.

HI, hemorrhagic transformation; PH, parenchymal hemorrhage.
Correlation between hyperglycemic and stroke outcomes
Compared with patients with normoglycemia, patients with persistent hyperglycemia had increased risk of death, whereas baseline and 24 h hyperglycemic patients had no significant association with 30-day death (p > 0.05, Table 3). In respect of hemorrhagic transformation, persistent hyperglycemia patients had the highest risk (OR = 13.3, 95% CI = 2.7–66.1) whereas baseline and 24 h hyperglycemic patients were not associated with hemorrhagic transformation (p > 0.05, Table 3).
Logistic regression model: adjusted ORs (95% CIs) of hyperglycemic patterns in relation to the respective outcomes.
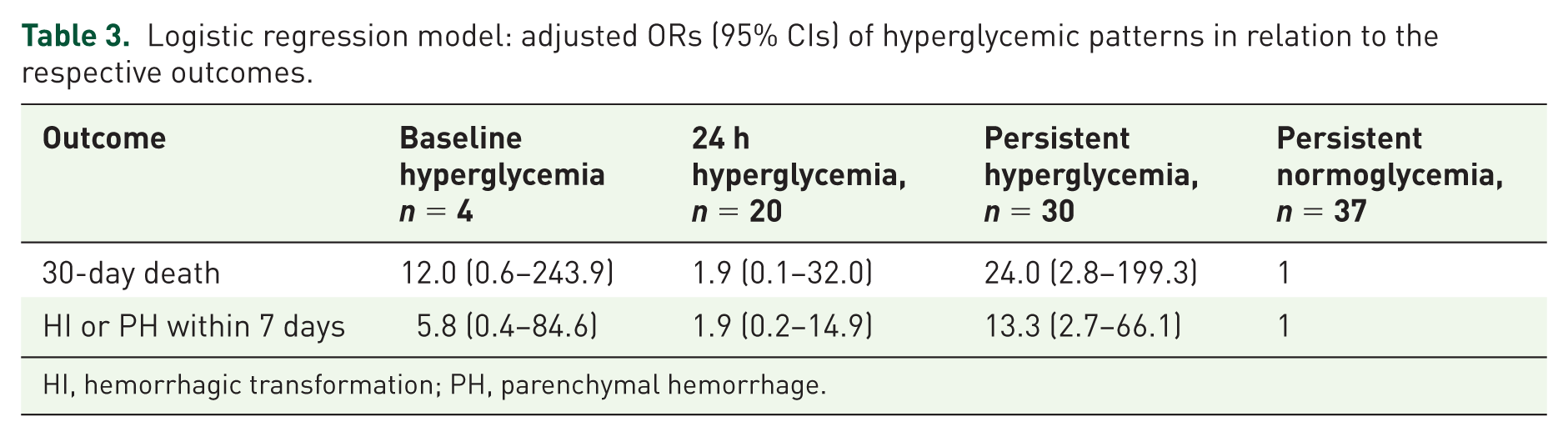
HI, hemorrhagic transformation; PH, parenchymal hemorrhage.
Discussion
In this study we monitored the blood glucose levels of non-diabetic patients with acute ischemic stroke upon and 24 h after admission. We found that persistent hyperglycemia in the 24 h period after admission was associated with 30-day mortality after acute ischemic disabling stroke and parenchymal hemorrhage within the first 7 days.
Previous studies have shown that hyperglycemia is an important predictor of increased risk of poor outcomes in acute ischemic stroke without diabetes,3,9–11 which is in line with the present study in that hyperglycemia after stroke was associated with bad outcomes. Thus, our study as supported by all other evidences proves the contribution of hyperglycemia on poor functional outcome after acute ischemic stroke. Such findings suggested that upon admission, lowering blood glucose could be beneficial for better prognosis in stroke patients without diabetes. But up to now, no beneficial effect of intensive glucose control on clinical outcome after acute ischemic stroke has been reported. 12 However, an ongoing prospective randomized clinical trial with a large sample size (SHINE) might offer optimal management strategies against hyperglycemia for better outcomes in patients suffering acute stroke. 13
Stress response has been seen as a cause of post-stroke hyperglycemia that may affect stroke outcome adversely. In the present study, the weak correlation between baseline glucose level and NIHSS score (r = 0.10, p < 0.004) does not convincingly verify that hyperglycemia is caused by the severity of stroke, which may relate to stress responses. Instead, persistent hyperglycemia was correlated with poor outcome. This indicates that the extent of injury and outcomes of patients depends, instead of the acute level of serum glucose, on the sustained state of hyperglycemia. This assumption was also supported by a study by Baird and colleagues.4, 14
Patients with persistent hyperglycemia are often found with hemorrhagic transformation. It is consistent with findings of Paciaroni and colleagues in that hyperglycemia during acute ischemic stroke predisposes to parenchymal hemorrhage, which in turn determines a non-favorable outcome at 3 months. 15 Recent experimental studies suggest that the main mechanism contributing to hemorrhagic infarction is the disruption of the blood–brain barrier and neuronal cell death. High glucose exposure leads to endothelial apoptosis resulting from mitochondrial dysfunction 16 and enhanced inflammation and oxidative stress17,18 in which matrix metalloproteinase-2 (MMP-2) and matrix metalloproteinase-9 (MMP-9) have been suggested be involved.19,20
In conclusion, our study revealed that persistent hyperglycemia after stroke was correlated with higher 30-day mortality. This suggests that high blood glucose during acute ischemic stroke should be carefully managed, especially during the first 24 h after stroke onset. Further investigation for developing optimal strategies to target hyperglycemia is of great importance for better prognosis in patients suffering from acute ischemic stroke.
Footnotes
Funding
This research received the National Natural Science Foundation of China (81601015) and Beijing Talents Fund(2015000021469G220) and Beijing Tiantan Hospital Fund(2015-YQN-13).
Conflict of interest statement
The authors declare that there is no conflict of interest.