
Abstract
Background:
Pediatric headache disorders are a significant public health issue, affecting school performance, social participation, and quality of life.
Objective:
Our aim was to explore the age- and gender-related changes in the characteristics and burden of headaches from childhood to adolescence, with a focus on diagnostic shifts, frequency, intensity, and quality-of-life.
Design:
We conducted a cross-sectional survey on five primary and secondary schools in the L’Aquila district, Italy.
Methods:
Using the translated Italian version of the Headache-Attributed Restriction, Disability, Social Handicap and Impaired Participation questionnaire, we collected data on headache frequency, intensity, duration, associated symptoms, and impact. Diagnoses were algorithmically assigned through International Classification of Headache Disorders, 3rd edition criteria. Statistical analyses examined the effects of age, gender, and their interaction on clinical and quality-of-life outcomes.
Results:
In total, 431 students were included (mean age: 9.82 ± 2.28 years; range: 6–15; 52.9% female). Findings indicated that as children grow older, headaches become increasingly frequent, longer in duration, and more intensely experienced. The progression from primary to secondary school was accompanied by a transition in diagnosis, with undifferentiated headaches giving way to more specific categories, such as probable or definite migraine and, to a lesser extent, tension-type headache. Age-by-gender interactions revealed that older females experienced greater frequency and a more pronounced impact, while headache frequency affected quality of life with increasing age.
Conclusion:
Findings highlight gender-specific developmental trends in headache, characterized by increased frequency, intensity, and diagnostic clarity from childhood to adolescence. The burden of headache, particularly among older students, underscores the need for early recognition and age-appropriate interventions.
Plain language summary
Introduction
Migraine is one of the most disabling diseases worldwide, affecting people across all age groups. According to the Global Burden of Disease, migraine ranks as the second most disabling neurological condition among adults aged 20–59 years, and, remarkably, it is the leading cause of disability among neurological conditions in individuals aged 5–19 years.1 –3 The prevalence of migraine in children and adolescents is 1%–3% in those aged 3–7 years, 4%–11% in those aged 7–11 years, and 8%–23% by age 15, with sustained migraine-related disability leading to reduced well-being, loss of productivity, and impaired social functioning. Diagnosis is based on clinical criteria from the International Classification of Headache Disorders, 3rd edition (ICHD-3), by the International Headache Society. 4 However, these criteria may not fully apply to younger age groups due to developmental differences, as migraine in children and adolescents often presents with clinical patterns that differ from those observed in adults. Furthermore, measures of migraine-related disability in younger patients are limited. Due to these discrepancies and gaps, the true prevalence of migraine in young people may be underestimated, which in turn reduces both the quantity and quality of care they receive. This creates a vicious cycle that exacerbates their disability. This is further compounded by the stigma associated with migraine due to its invisible nature. 5 Stigma leads to widespread societal stereotypes, promoting the misconception that migraine is used as an excuse to avoid responsibilities or to opt out of roles and functions, both in the workplace and at school. 5 Recently, a call to action has been made to raise awareness about migraine among both patients and society. 3 Raising awareness, improving access to treatment, and advancing research on new therapies for all age groups are the key priorities to address. Another priority, both for young people and adults, is to propose preventive therapy as early as possible in order to improve patients’ quality of life and the progression of the disease. 6 In this context, school-based studies may help identify the clinical characteristics of headaches in children and adolescents, quantify migraine-related disability, and pave the way for tailored management strategies for this age group, which deserves greater attention. The aim of this study was to investigate the age- and gender-related changes in clinical characteristics of headache and its burden from childhood (6–11 years) to adolescence (12–15 years) in a group of Italian students from the L’Aquila district (central Italy).
Materials and methods
Study design
The study was a cross-sectional survey based on the administration of self-completed structured questionnaires. No formal a priori sample size calculation was conducted, as participation was determined by school consent and logistical feasibility within the selected district. Participating schools within the L’Aquila district (central Italy) were recruited based on willingness to participate following invitations sent to school principals. A total of five primary and secondary schools agreed to take part. Before starting, the characteristics of the survey were explained to principals and teachers at the participating schools. An information sheet summarizing the objectives, and the characteristics of the study was sent to parents, who were encouraged to complete the questionnaire together with their children. The questionnaire could be done either hand-written or digitally via a specially created link. Data were collected anonymously and analyzed in an aggregate manner, with no possibility of identifying individual participants. The reporting of this study conforms to STROBE guidelines (see Supplemental Material 1). 7
Survey instruments
We used the child and adolescent versions of the Lifting the Burden’s (LTB) Headache-Attributed Restriction, Disability, Social Handicap and Impaired Participation (HARDSHIP) structured questionnaire, 8 translated into Italian. The translation was performed in accordance with the guidelines proposed by the Translation Working Group for the translation of documents produced by the LTB group. 9 In detail, the following protocol was used to develop an Italian version of the HARDSHIP questionnaire:
(a) Preparation of the work and review of the guidelines proposed by the Translation Working Group for the translation of documents produced by the LTB group. 8
(b) Selection of the translation coordinator (F.P.), who has technical expertise, is bilingual in English and the target language and is skilled in mediating between different translators.
(c) Selection of two independent panels of translators (first panel F.G., D.D.G., G.S.—second panel E.T., P.S., S.C.) for forward translation into the target language.
(d) Production of a consensus-based translation.
(e) Back translation.
(f) Quality assessment (including linguistic review, target audience review, and production of final quality-assured translation).
(g) Final consensus and proofreading for dissemination.
The original questionnaires have been validated for children aged 6–11 and adolescents aged 12–17, showing acceptability, validity, usefulness, and feasibility for both diagnosing and assessing the overall burden of headaches in these age groups. 10
The HARDSHIP questionnaire has a modular format and includes demographic enquiries (gender was recorded as self-reported by participants or their parents), headache screening questions, and diagnostic enquiries based on ICHD-3 criteria. Additional information about headache-attributed burden investigate disability, missed day-schools, and reduced productivity due to headache. Information on the impact of headaches pertains to the last 4 weeks prior to administration, except for one form that examines the presence and impact of headaches on the previous day. The questionnaire is designed for data collection either through self-completion or by interviewers during face-to-face interactions, with interviewers not expected to diagnose the type of headache (migraine, tension-type headache (TTH), medication-over-used headache).9,10 Diagnosis is done algorithmically from the diagnostic question set.9,10 The translated versions of the questionnaires for children and adolescents, as well as the supporting questionnaires for mediators and teachers, are provided as Supplemental Material 2–5.
Diagnoses
Diagnoses were made algorithmically according to HARDSHIP methodology.9,10 H15+ (i.e., headache reported on 14 days in the preceding 28 days) was first identified and categorized according to reported medication use into probable Medication Overuse Headache (use on 14/28 days) or “other H15+” (use on 0–13/28 days). To all other reported headaches, the algorithm first applied criteria for undifferentiated headache (mild intensity and usual duration <1 h) and then the ICHD-3 criteria for definite migraine, definite TTH, probable migraine, and probable TTH in this strict order. Remaining cases were recorded as unclassified.
Data management and statistical analysis
All hand-written questionnaires were collected and transferred to the Department of Biotechnological and Applied Clinical Sciences of the University of L’Aquila. Data from hand-written questionnaires were combined with digital responses and entered into an Excel sheet. Descriptive statistics (mean, standard deviation, percentage) were performed: continuous variables were expressed as the mean ± standard deviation, while categorical variables were presented as frequency or percentage.
To mitigate the impact of potential selection bias arising from the relatively low response rate (23.5%), we deliberately avoided interpreting population-level prevalence estimates, as these could have been affected by the likelihood that families who chose to participate differed systematically from those who did not, possibly reflecting a greater concern about, or direct experience with, headaches. Therefore, we focused our analyses exclusively on respondents who reported at least one headache attack during the previous year (item 5, n = 300).
A proportional odds ordinal logistic regression (OLR) was conducted including age, gender, and their interaction as predictors, and the usual duration of headache episodes (item 6; categorized as “<1,” “1–2,” “2–4,” and “>4 h”) and their intensity (item 7; categorized as “Not intense,” “Slightly intense,” and “Very intense”) as dependent variables. To investigate the influence of variables such as age and gender on headache pain typology (items 8; “Throbbing” or “Pressing”) and lateralization (items 9; “Bilateral,” “In the middle,” and “Unilateral”), logistic and multinomial regression analyses were performed, respectively, with responses to each item treated as the dependent variable, and age, gender, and their interaction included as predictors.
A Chi-squared test was conducted to test the association between clinical diagnoses (undifferentiated, probable migraine, definite migraine, probable TTH, and definite TTH) and school level (primary, secondary). The same analysis was replicated for male and female participants separately to identify possible gender-related differences in the transition from primary to secondary school on clinical diagnosis rates. Moreover, we performed a binomial logistic regression to evaluate the role of gender, age, and their interaction (predictors) on the odd of receiving a specific diagnosis (probable migraine, definite migraine, probable TTH, or definite TTH) compared to an undifferentiated one (dependent variable).
A total score was calculated by summing the responses to items 27–32 (“Other questions about headache impact”), assigning scores of 0 for “Never,” 1 for “Sometimes,” 2 for “Often,” and 3 for “Always” (reverse coding was applied for item 31). This method produced a continuous variable reflecting the impact of headaches over the past month (“headache impact score”). Subsequently, a generalized linear model (GLM), was fitted using as dependent variables both the headache frequency over the past 4 weeks (item 18) and the headache impact score, using age, gender, and their interaction as predictors. For the headache frequency data, a negative binomial distribution was chosen over Poisson due to the nature of the frequency data and the violation of the equidispersion assumption (χ2/df = 4.72).11,12 Additionally, a total “quality-of-life score” was computed summing responses to items 33–44 after assigning scores of 0 for “Never,” 1 for “Sometimes,” 2 for “Often,” and 3 for “Always,” with reverse coding applied to items 35, 36, 40, 41, 42, and 44 (higher scores reflect poorer quality of life). To examine the role of headache frequency over the past 4 weeks on quality of life and its interaction with demographic features, the total quality-of-life score was used as the dependent variable in a GLM with headache frequency, age, gender, and their interaction as predictors.
In all models, significant interaction effects were further explored using simple slope analyses to elucidate the nature of these effects. Statistical analyses were performed using Jamovi software (Version 2.4.12.0), and results were interpreted with a significance threshold of p < 0.05 (two-tailed).
Variance inflation factors indicated elevated values for gender (VIF = 22.18) and the age × gender interaction (22.70), as typically occurs in moderated regression models. 13 This collinearity was expected and did not affect model interpretability; therefore, no corrective measures were taken.
Results
Participants
A total of 974 students attending primary school and 861 students attending secondary school were invited to participate in the survey. A total of 431 students (23.5%), who provided sufficiently completed questionnaires for the analysis, were finally included in the study (mean age ± SD: 9.82 ± 2.28 years, range: 6–15 years, 52.9% females). Out of them, 290 attended the primary school (8.54 ± 1.57 years, range: 6–11 years, 52.4% females) and 141 the secondary school (12.40 ± 0.88 years, range: 11–15 years, 53.9% females). Individual reasons for nonresponse (e.g., parental refusal, absenteeism, or scheduling conflicts) were not unequivocally identified, as invitations were digitally disseminated to all eligible families through the school communication platform.
Clinical characteristics of headache
At least one headache attack in the past year was reported by 178 primary schoolchildren (61.4%) and by 122 adolescents attending secondary school (86.5%). In both age groups, the pain was not strictly unilateral (primary school: 43.4% bilateral pain; 41.1% pain in the middle; 15.4% unilateral; secondary school: 46.7% bilateral pain; 33.6% pain in the middle; 19.7% unilateral), in most of cases lasted less than an hour (primary school: 54.5%; secondary school: 34.4%), and was described as slightly intense (primary school: 49.7%; secondary school: 63.3%). In the overall sample, the pain during attacks was equally described as either pressing (primary school: 52.1%; secondary school: 49.6%) or throbbing (primary school: 47.9%; secondary school: 50.4%). The most frequently associated symptom was phonophobia (primary school: 77.5%; secondary school: 79.5%), followed by photophobia (primary school: 34.3%; secondary school: 47.5%), nausea (primary school: 24.7%; secondary school: 23.8%), and vomiting (primary school: 10.1%; secondary school: 5.7%). Both primary schoolchildren (51.1%) and adolescents (55.7%) reported avoiding physical activity during headache. A detailed description of headache characteristics by sex and school level is provided in Table 1.
Distribution of headache characteristics stratified by gender and school level among participants reporting at least one headache episode in the past year.

Values are presented as counts and percentages within each subgroup.
The OLR examining the effect of demographic factors on the usual duration of headache episodes showed that the odds of reporting a longer headache duration increased with age (exp(B) = 1.22, 95% confidence interval (CI) = 1.11–1.35, p < 0.001). Gender was not a significant predictor (exp(B) = 1.07, 95% CI = 0.97–1.16, p = 0.51), suggesting that males and females did not differ significantly in their likelihood of reporting longer headache durations. Similarly, the interaction between age and gender was not significant (exp(B) = 1.01, 95% CI = 0.83–1.23, p = 0.89), indicating that the relationship between age and headache duration did not vary by gender. As shown in Figure 1(a), the probability of reporting shorter headache durations (“<1 h”) decreases with age, while the probability of longer durations (“1–2,” “2–4,” and “>4 h”) increases progressively with age.

Predicted probabilities of usual headache duration (a) and intensity (b) categories as a function of age. The shaded areas indicate the standard error.
The OLR estimating the role of age and gender on the usual intensity of headache attacks indicated that the age significantly predicted headache intensity (exp(B) = 1.20, 95% CI = 1.08–1.33, p < 0.001). In detail, the probability of reporting lower headache intensities (“Not intense”) decreases with age, while the probabilities of higher intensities (“Slightly intense” and “Very intense”) increase with age (Figure 1(b)). In contrast, gender (exp(B) = 1.81, 95% CI = 0.21–15.38, p = 0.59) and the age × gender interaction (exp(B) = 0.92, 95% CI = 0.75–1.13, p = 0.43) were not significant, suggesting that neither gender alone nor its interaction with age played a meaningful role in predicting headache intensity.
Binomial logistic regression aimed to elucidate a role of demographic factors on headache pain typology (Throbbing” vs “Pressing”) suggested no significant effects of age (exp(B) = 0.99, 95% CI = 0.90–1.11, p = 0.99), gender (exp(B) = 0.74, 95% CI = 0.08–6.75, p = 0.79), and their interaction (exp(B) = 1.03, 95% CI = 0.83–1.27, p = 0.81).
Similarly, multinomial logistic regression showed that none of the predictors had significant effects on the likelihood of reporting either “In the middle” (age: exp(B) = 0.98, 95% CI = 0.87–1.10, p = 0.69; gender: exp(B) = 0.43, 95% CI = 0.04–4.68, p = 0.49; age × gender: exp(B) = 1.15, 95% CI = 0.91–1.44, p = 0.24) or “Unilateral” headache pain lateralization (age: exp(B) = 1.06, 95% CI = 0.90–1.24, p = 0.49; gender: exp(B) = 0.31, 95% CI = 0.01–8.70, p = 0.49; age × gender: exp(B) = 1.10, 95% CI = 0.81–1.51, p = 0.54) compared to “Bilateral.”
Clinical diagnosis
When considering the entire subgroup of participants reporting at least one headache episode, without stratification by sex or age, the most frequent diagnosis was undifferentiated headache (40.3%), followed by probable migraine (28.7%), definite migraine (15.3%), probable TTH (14.3%), and definite TTH (1.3%). No cases with a diagnosis of medication overuse headache were detected. Chi-squared test applied on the overall sample showed a significant association between school level and clinical diagnosis (Table 2). A reduced rate of undifferentiated headache was observed from primary to secondary school along with a proportional increase in cases of probable and definite migraine. Moreover, a reduction in probable TTH was observed when transitioning from elementary to middle school, accompanied by an increase in the rate of definitive TTH diagnosis. The changes appeared to depend on gender, as they are observed only in the male sample.
Clinical diagnosis rates by school level in the sample that reported at least one headache attack during the previous year, and within male and female groups.

The results of Chi-squared tests were also reported.
TTH, tension-type headache.
Binomial logistic regression showed that the probability of receiving a specific diagnosis (probable migraine, definite migraine, probable TTH, or definite TTH) compared to an undifferentiated diagnosis was not affected by age (exp(B) = 1.00, 95% CI = 0.86–1.15, p = 0.96). On the other hand, both the gender factor (exp(B) = 0.04, 95% CI = 0.004–0.41, p = 0.007) and its interaction with age were significant (exp(B) = 1.36, 95% CI = 1.09–1.70, p = 0.007). Simple slope analyses (Figure 2) indicated that the odds of receiving a specific diagnosis increased with age only in males (exp(B) = 1.35, 95% CI = 1.14–1.60, p < 0.001), while no variation was present in female participants (exp(B) = 1.00, 95% CI = 0.86–1.15, p = 0.96).
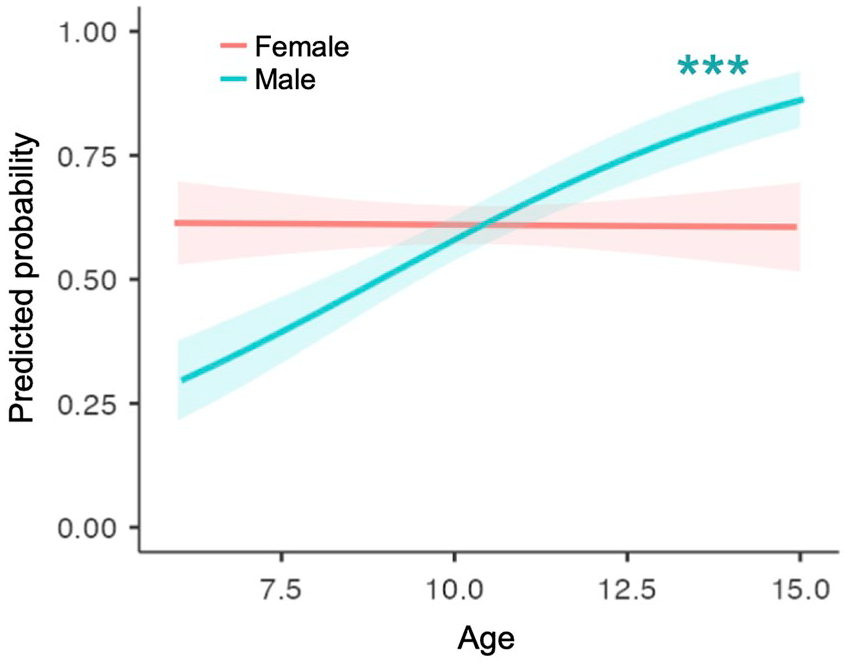
Predicted probabilities of receiving a specific diagnosis (probable migraine, definite migraine, probable TTH, or definite TTH) compared to an undifferentiated one as a function of age by gender. The shaded areas indicate the standard error.
Burden of headache and disability
A high percentage of participants (70.9%) reported at least one attack in the past 4 weeks (primary school: 1.52 ± 2.13 attacks; secondary school: 4.22 ± 5.53 attacks). More than one symptomatic drug was taken in 16.8% of cases. In both age groups, a high percentage of students day (primary school: 46.5%; secondary school: 65.7%) missed at least one school in the past 4 weeks due to headache. When assessing the impact on daily activities, the majority of participants reported being unable to participate in leisure and entertainment activities for at least 1 day due to headaches in the past 4 weeks (primary school: 54.2%; secondary school: 73.6%).
The negative binomial model showed a significant effect of age (exp(B) = 1.21, 95% CI = 1.14–1.30, p < 0.001) in predicting headache frequency. Analysis suggested no differences between male and females (exp(B) = 3.29, 95% CI = 0.81–13.44, p = 0.10), while a significant age × gender interaction emerged (exp(B) = 0.87, 95% CI = 0.76–0.98, p = 0.03). Simple slope analysis (Figure 3(a)) indicated a higher number of monthly headache attacks with increased age in both gender groups, with females that showed a stronger relationship (females: exp(B) = 1.31, 95% CI = 1.19–1.43, p < 0.001; males: exp(B) = 1.13, 95% CI = 1.03–1.24, p = 0.011).

(a) Relationship between age and (a) monthly headache attacks or (b) headache impact score by gender. Shaded areas represent standard errors.
The GLM evaluating the effect of age and gender on the headache impact score showed a not-significant effect of age (B = 0.11, 95% CI = −0.03 to 0.24, p = 0.13) and gender (B = 2.78, 95% CI = −0.08 to 5.86, p = 0.06). However, a significant age × gender interaction was obtained (B = −0.33, 95% CI = −0.60 to −0.06, p = 0.018). Simple slope analysis (Figure 3(b)) indicated a higher headache impact score with increased age only within females (females: B = 0.27, 95% CI = 0.08–0.46, p = 0.005; males: B = −0.06, 95% CI = −0.26 to 0.14, p = 0.57).
The impact of headache attacks on quality of life
The GLM estimating the role of headache frequency, gender, and age in predicting quality-of-life score indicated no significant effect of age (B = 0.05, 95% CI = −0.26 to 0.36, p = 0.75), gender (B = −0.27, 95% CI = −1.65 to 1.11, p = 0.70), headache frequency (B = −0.97, 95% CI = −2.12 to 0.17, p = 0.10), and the gender × headache frequency interaction (B = −0.19, 95% CI = −0.55 to 0.17, p = 0.30).
However, a significant age × headache frequency was highlighted (B = 0.10, 95% CI = 0.004–0.20, p = 0.04). Simple slope analysis showed that a positive relationship between headache frequency and quality-of-life score appears with increasing age (mean age − 1 standard deviation (8.02 years): B = −0.16, 95% CI = −0.54 to 0.23, p = 0.42; mean age (10.25 years): B = 0.11, 95% CI = −0.14 to 0.28, p = 0.51; mean age + 1 standard deviation (12.48 years): B = 0.30, 95% CI = 0.10–0.50, p = 0.004; Figure 4).

Relationship between number of monthly headache attacks and quality-of-life score by age. Higher scores reflect poorer quality of life. Shaded areas represent standard errors.
Discussion
Headache disorders in children and adolescents represent a significant and underappreciated public health issue, with far-reaching consequences for quality of life, school attendance, and social participation.14 –16 In this study, we aimed to characterize the epidemiology, clinical features, and burden of headaches in a cohort of Italian schoolchildren and adolescents, focusing on the roles of age, gender, and headache frequency in shaping headache characteristics and their impact.
Overall, our findings suggest that with increasing age, headaches in children tend to become more frequent, last longer, and are perceived as more intense. Furthermore, with the transition from primary to secondary school, a shift in diagnosis from undifferentiated headache toward more specific classifications such as probable or definite migraine and, to a lesser extent, TTH was observed. These results align with prior evidence indicating that the prevalence and severity of headaches evolve during pediatric development and underscore the importance of early recognition and appropriate management strategies.17 –20 It is worth noting that the proportion of participants meeting criteria for migraine diagnosis may partly reflect the inclusion of features such as throbbing pain, avoidance of physical activity, and phonophobia in the ICHD-3 algorithm. While these characteristics are commonly used to define migraine in adults, their diagnostic utility in children remains debated, given the developmental differences in symptom expression and reporting. Although the HARDSHIP diagnostic approach incorporates these features algorithmically, our findings underscore the need to revisit how these criteria apply to pediatric populations. Future revisions of diagnostic systems may benefit from age-adapted definitions that better reflect the developmental trajectories of childhood and adolescent headache. Previous studies have highlighted both the significance of pediatric headache frequency and associated disability, as well as the limitations of the ICHD-3 criteria in accurately capturing and reflecting this phenomenon.21 –24 These studies confirm that headaches in children and adolescents have specific characteristics that should be acknowledged and considered to avoid underdiagnosis and underestimation of the disease. Aspects such as pain duration and location, and the need to infer symptoms from behavior rather than verbal description have been previously highlighted. 21 Moreover, certain features in children have previously been recognized as age-dependent, and some associated symptoms—such as loss of appetite, stomach discomfort, dizziness, and cranial autonomic symptoms—have been pointed out as relevant for reaching a proper diagnosis. 21 Our findings showed that older children are more likely to experience both longer and more intense headache attacks, a pattern that may reflect the increasing complexity of headache disorders as youth approach adolescence. This observation is consistent with existing literature, which reports that migraine and other primary headaches often emerge or become more clinically distinct during early adolescence, potentially due to hormonal changes, brain maturation, alterations in sleep patterns, and an increase in academic and psychosocial stressors.19,25 Notably, while gender was not a predictor of headache duration or intensity, the interaction between age and gender emerged as significant for headache frequency and impact. The age-by-gender interaction in headache frequency, wherein older females showed a stronger association between age and frequency compared to males, could be attributed to the hormonal fluctuations and menarche-related changes occurring in adolescent girls.26 –28 In terms of diagnostic categories, we observed a reduction in undifferentiated diagnoses alongside an increase in both probable and definite migraine as children matured, which is consistent with the notion that diagnostic clarity improves as headache phenotypes become more characteristic over time. This finding is consistent with recent research that proposed undifferentiated headache as a precursor or immature expression of migraine or TTH in a developing brain,19,25 supporting the inclusion of this clinical classification in epidemiological studies to provide a more comprehensive understanding of the headache disorder spectrum. 25 Interestingly, the transition in headache diagnosis was more evident in males, confirming the notion that migraine incidence seems to peak earlier in men than in women over the lifespan.17,29
Our study also indicates a substantial burden of headache on daily life, with a high percentage of participants missing school days and forgoing leisure activities. These findings corroborate the broader literature on the substantial impact of pediatric headaches on academic performance, social participation, and general well-being.17,30 Importantly, while our results did not reveal significant main effects of age or gender on headache-related quality of life, the interaction between age and headache frequency was significant, suggesting that the detrimental impact on quality of life becomes more evident as children grow and encounter more frequent headaches. This may reflect increasing academic responsibilities, extracurricular demands, and the psychosocial complexities of adolescence, which can exacerbate the functional consequences of headache disorders.
The strengths of this study include the use of a validated and internationally recognized diagnostic tool (the HARDSHIP questionnaire). However, some limitations should be acknowledged. The cross-sectional design does not allow for causal inferences or the examination of longitudinal trajectories of headache evolution. Prospective, longitudinal studies are warranted to determine whether the observed increases in headache frequency and intensity over time and their relationship with quality of life persist into late adolescence or early adulthood. We also acknowledge that, while the questionnaire-based, algorithmic approach to diagnosis enabled standardized and large-scale data collection, it does not replace a clinical evaluation by healthcare professionals. Moreover, as this was an exploratory, cross-sectional survey conducted within the constraints of school-level availability and consent, a formal a priori sample size calculation was not performed. Although our study included a moderate sample size capturing a range of ages from 6 to 15 years, this remains below the recommended N > 2000 for population-based headache studies according to consensus guidelines. 31 Consequently, the sample sizes within each diagnostic group were not sufficient to support statistically robust analyses stratified by diagnosis. Future research with larger samples might combine similar survey methodologies with medical evaluations to better characterize headache diagnoses, severity, and associated comorbidities, allowing to address how clinical and functional outcomes vary across diagnostic subtypes. An additional limitation is that the survey was conducted in a single geographic area, where local demographic and socio-cultural factors might not reflect broader national populations, thus limiting the generalizability of our findings. Additionally, the participation rate was not optimal, which may lead to selection bias (i.e., participants might differ from non-participants in terms of headache severity, health-seeking behavior, or parental involvement). Although individual reasons for non-response were not unequivocally identified in this study, in our opinion, the main non-participation reason was represented by a general overload of information that needs to be daily shared with parents leading to scheduling conflicts for each individual initiative: an information sheet describing the study and invitations to participate, for everyone regardless of whether they have a history of headaches, were digitally distributed to all eligible families through the school’s communication platform, with each pupil asked to return the signed informed consent form from their parents. However, parents receive many communications through the platform, and their attention may not be fully focused on every initiative, especially for extracurricular ones. This is consistent with findings from other validation studies, which reported the highest refusal rates in high-income urban areas (67.2%), primarily due to the perception that the initiative was too time-consuming. 22 This limitation can be overcome, or at least mitigated, in future studies by ensuring that the dissemination of the participation request is preceded by awareness-raising events. Finally, although our analyses focused on age and gender as primary predictors, we acknowledge that other psychosocial and contextual variables (e.g., family history of headache, socioeconomic background, sleep quality, and academic pressure) may influence both headache characteristics and their burden. These factors were not assessed in the present study, representing a potential source of unmeasured variability. Future research should include these aspects within multivariable frameworks to offer a more comprehensive understanding of pediatric headache etiology and impact.
Conclusion
Our findings deepen the understanding of how headache disorders present and evolve during critical developmental periods. By documenting an age-related progression toward more frequent, intense, and distinctly classifiable headache disorders—especially migraines—this study confirms the importance of improved screening and referral pathways within school health services, ensuring timely access to specialized care. Moreover, the observed increase in headache burden particularly among older girls suggests that gender-specific preventive measures should be implemented starting from early adolescence. School-based educational programs could help in promoting early recognition of headache symptoms, reducing stigma, and encouraging appropriate healthcare-seeking behaviors.
Effective screening strategies and age-appropriate interventions during a critical window of neurodevelopment are necessary to mitigate the indirect academic and social repercussions. 32 Furthermore, considering that the relationship between headache frequency and quality of life becomes more pronounced with age, healthcare providers and educators should remain vigilant about older children who may require more targeted support. Finally, improving our knowledge of pediatric headache patterns and their determinants will contribute to the design of more personalized, developmentally informed interventions that reduce disability, enhance well-being, and potentially improve long-term outcomes.
Supplemental Material
sj-docx-2-tan-10.1177_17562864251356066 – Supplemental material for Developmental trends in headache: an Italian school-based study of age- and gender-related changes in clinical characteristics and burden from childhood to adolescence
Supplemental material, sj-docx-2-tan-10.1177_17562864251356066 for Developmental trends in headache: an Italian school-based study of age- and gender-related changes in clinical characteristics and burden from childhood to adolescence by Federico Salfi, Gennaro Saporito, Simone Cesarano, Federica Guerra, Pamela Silva, Dina Di Giacomo, Elisabetta Tozzi, Michele Ferrara, Bruno Colombo and Francesca Pistoia in Therapeutic Advances in Neurological Disorders
Supplemental Material
sj-docx-3-tan-10.1177_17562864251356066 – Supplemental material for Developmental trends in headache: an Italian school-based study of age- and gender-related changes in clinical characteristics and burden from childhood to adolescence
Supplemental material, sj-docx-3-tan-10.1177_17562864251356066 for Developmental trends in headache: an Italian school-based study of age- and gender-related changes in clinical characteristics and burden from childhood to adolescence by Federico Salfi, Gennaro Saporito, Simone Cesarano, Federica Guerra, Pamela Silva, Dina Di Giacomo, Elisabetta Tozzi, Michele Ferrara, Bruno Colombo and Francesca Pistoia in Therapeutic Advances in Neurological Disorders
Supplemental Material
sj-docx-4-tan-10.1177_17562864251356066 – Supplemental material for Developmental trends in headache: an Italian school-based study of age- and gender-related changes in clinical characteristics and burden from childhood to adolescence
Supplemental material, sj-docx-4-tan-10.1177_17562864251356066 for Developmental trends in headache: an Italian school-based study of age- and gender-related changes in clinical characteristics and burden from childhood to adolescence by Federico Salfi, Gennaro Saporito, Simone Cesarano, Federica Guerra, Pamela Silva, Dina Di Giacomo, Elisabetta Tozzi, Michele Ferrara, Bruno Colombo and Francesca Pistoia in Therapeutic Advances in Neurological Disorders
Supplemental Material
sj-docx-5-tan-10.1177_17562864251356066 – Supplemental material for Developmental trends in headache: an Italian school-based study of age- and gender-related changes in clinical characteristics and burden from childhood to adolescence
Supplemental material, sj-docx-5-tan-10.1177_17562864251356066 for Developmental trends in headache: an Italian school-based study of age- and gender-related changes in clinical characteristics and burden from childhood to adolescence by Federico Salfi, Gennaro Saporito, Simone Cesarano, Federica Guerra, Pamela Silva, Dina Di Giacomo, Elisabetta Tozzi, Michele Ferrara, Bruno Colombo and Francesca Pistoia in Therapeutic Advances in Neurological Disorders
Supplemental Material
sj-pdf-1-tan-10.1177_17562864251356066 – Supplemental material for Developmental trends in headache: an Italian school-based study of age- and gender-related changes in clinical characteristics and burden from childhood to adolescence
Supplemental material, sj-pdf-1-tan-10.1177_17562864251356066 for Developmental trends in headache: an Italian school-based study of age- and gender-related changes in clinical characteristics and burden from childhood to adolescence by Federico Salfi, Gennaro Saporito, Simone Cesarano, Federica Guerra, Pamela Silva, Dina Di Giacomo, Elisabetta Tozzi, Michele Ferrara, Bruno Colombo and Francesca Pistoia in Therapeutic Advances in Neurological Disorders
Footnotes
References
Supplementary Material
Please find the following supplemental material available below.
For Open Access articles published under a Creative Commons License, all supplemental material carries the same license as the article it is associated with.
For non-Open Access articles published, all supplemental material carries a non-exclusive license, and permission requests for re-use of supplemental material or any part of supplemental material shall be sent directly to the copyright owner as specified in the copyright notice associated with the article.