
Abstract
To examine indices of behavioural and emotional problems and temperamental traits in clinically referred children and adolescents suffering from tension headache or migraine. Headache in childhood and adolescence (<18 years) has been associated with the presence of behavioural and emotional difficulties, but limited data are available on the relationship between these problems and different types of headache. Clinically referred children and adolescents (N = 114), 6–16 years of age, suffering from primary headache according to the diagnostic criteria of the International Headache Society, 47 with tension-type headache (TH) and 67 with migraine (M), and 36 normal controls without headache (NC) were assessed using the Parent Child Behaviour Checklist (CBCL), Children's Depression Inventory (CDI), Multidimensional Anxiety Scale for Children (MASC), Conner's Parent Rating Scale (CPRS), and Emotionality–Activity–Sociability–Shyness Scale (EAS). Psychological and personality self-rating assessments were obtained also on the children's parents and siblings. Although most headache patients had scores within the normative non-pathological range, both TH and M patients had higher CBCL total, internalizing, and externalizing scores than NC (P < 0.001), and TH patients had higher scores than M patients. TH and M had higher CDI and MASC scores than NC (P < 0.05), with no difference between the headache groups. TH patients had higher Emotionality and Shyness scores, and lower Sociability scores than M patients. Clinically referred children and adolescents with TH and M had higher scores of behavioural and emotional symptoms, both of internalizing and externalizing type, than normal peers. The TH group had greater psychological and temperamental difficulties than the M group.
Introduction
Headache is common among children and adolescents. Epidemiological studies suggest that 10–30% of children and adolescents report weekly or daily headaches (1). Migraine occurs in 3–15% of children (2–5) while 9–33% of patients suffer from non-migrainous headache at least monthly (4, 6). The Headache Classification ad hoc Committee of the International Headache Society (IHS) (1988) includes different types of headache (7). Among primary headache, a distinction is made between tension-type headache (TH) and migraine (M). In childhood, headache can be the expression of psychological difficulties, such as anxiety and depression, and stressful life events have been frequently implicated in the onset, exacerbation, and maintenance of headache (8). Conversely, headache itself can be a source of stress, leading to functional impairment, which can cause anxiety in both patients and families (9). The relationship between headache and psychological difficulties has been the object of considerable investigation especially in adults, but also in children, although the latter has received less attention (1, 10–14).
In clinical samples, anxiety and depression symptoms have been found to be associated with M, but not with TH in children (14), a finding that is consistent with epidemiological studies in adults (15, 16). Recently, in a population-based study in Finnish children, levels of internalizing symptoms, and somatic symptoms in particular, were increased among M children, but not among TH children, compared with non-headache children (12). Taken together, these data seem to indicate that anxiety, depression and somatic symptoms are more specifically related to M than to TH. An association between headache and certain personality traits or psychiatric disorders has also been reported in adults (17–20). In children, specific traits, such as rigidity and emotional inhibition, have been found among children with idiopathic headache (21).
The purpose of our study was to examine further the presence of behavioural and emotional symptoms among clinically referred children. Because of the relatively small sample size, this investigation was intended to be more exploratory than hypothesis testing. In particular our aims were:
To examine the association between headache and ratings of behavioural and emotional difficulties. It was predicted that children who were clinically referred because of primary headache would have higher levels of psychological symptoms in general, and depression, anxiety and somatic symptoms in particular, compared with children without headache.
To examine the possible specific association between type of headache and psychological symptoms. It was predicted that the association with internalizing symptoms in general, and anxiety, depression and somatic symptoms in particular, would be more evident among M children than TH children.
To examine the relationship between temperament and headache and its subtypes. It was predicted that children with headache would display traits of greater shyness, higher emotionality and lower sociability than non-headache children.
To examine temperament in relatives of cephalalgic children compared with relatives of non-headache children. It was predicted that relatives of cephalalgic children would have higher rates of shyness, higher emotionality and lower sociability than relatives of non-headache children.
Methods
Subjects
Children and adolescents, age 6–16 years, referred to the headache clinic of Child and Adolescent Neuropsychiatry of the Paediatric Department at the University of Catania, Italy, during the years 2002 and 2003, and meeting diagnostic criteria for TH or M according to the 1988 IHS criteria (7), were enrolled in this study. Patients were diagnosed according to the 1988 IHS criteria (7), as the more recent 2004 ICHD II was published after the data collection was completed (22). Normal controls (NC) were randomly selected from a database of healthy children attending a well-being paediatric clinic for routine checks.
Parents and siblings of the subjects participating in this study were also invited to participate in the psychological and personality trait assessments. Parental consent was obtained for each subject, and each child assented to participation.
Assessments
Each patient received a comprehensive physical and neurological assessment, including EEG, and ophthalmological examination. In a few cases, magnetic resonance imaging (MRI) was also obtained. Two child neuropsychiatrists trained in the diagnostic criteria set by the 1988 IHS (7) classified the patients as suffering from TH or M, with or without aura. The psychological evaluation included administration of the following instruments:
The Child Behaviour Checklist (CBCL), which is a 113-item questionnaire completed by the parents. The CBCL rates child behavioural and emotional problems both globally and along the two dimensions of ‘internalizing’ symptoms composed of subscales Anxious/Depressed, Withdrawn, and Somatic Complaints, such as anxiety and depression, and ‘externalizing’ symptoms, such as aggression and hyperactivity. Raw scores of each clinical factor were transformed to T scores based on published norms, and scores of≥70 were considered indicative of clinical impairment. Scores for specific subscales were also computed (23, 24).
The Children's Depression Inventory (CDI), which was completed by the child, was used to rate symptoms of depression (25). The CDI is a self-rating scale that consists of 27 items scored on a three-point scale (0, absent; 1, moderate; 2, severe) reflecting growing severity of symptoms. Total scores range from 0 to 54. A 19-point cut-off indicates the ideal threshold discriminating children at risk of depression from non-depressed children.
The Multidimensional Anxiety Scale for Children (MASC), which was also completed by the child to score symptoms of anxiety. The MASC is a 39-item four-point Likert-style self-report scale that has undergone extensive psychometric evaluation (26). MASC main and subfactors include (a) physical symptoms (tense/restless and somatic/autonomic), (b) harm avoidance (anxious coping and perfectionism), (c) social anxiety (humiliation/rejection and public performance fears), and (d) separation anxiety. The raw scores were converted into standard T-scores.
The Conner's Parent Rating Scale (CPRS), which was completed by the parents. We applied the latest revision of the CPRS, with a 27-item short form (CPRS-R:S) (27). Each item is a brief description of a potentially problematic behaviour that the parent rates on a four-point Likert-type scale (1, not at all; 2, just a little; 3, pretty much; and 4, very much). All scores for items loading on a particular scale are summed to produce a raw scale score. Raw scores were used in the absence of norms for the Italian population.
The Emotionality, Activity, Sociability and Shyness Scale for Childhood (EAS) was completed by the children, their parents and siblings, to rate four temperament traits: Emotionality (the tendency to become easily upset), Activity (the tendency to be restless), Sociability (the tendency to prefer the presence of other over solitude), and Shyness (uneasiness in novel or unfamiliar social situations) (28). For each child, parents were asked to rate each statement on a ‘five-point’ Likert scale, ranging from 0 (not characteristic or typical of the child) to 5 (very characteristic or typical of the child). Mothers and fathers were asked to rate each child; the child scores were obtained by averaging parents’ ratings. Higher scores on the EAS do not necessarily represent greater dysfunction, but subjects with higher scores have been found to be more likely to suffer from emotional problems (28).
Data analysis
Data were analysed with standard descriptive statistics: χ2 test, analysis of variance and non-parametric tests, as indicated in the text and tables. A two-end P-value of <0.05 was used as the cut-off point of statistical significance. When multiple tests were conducted within the same measure (e.g. in the case of the CBCL), P was corrected using a Bonferroni's method by multiplying the obtained P by the number of tests. However, when an omnibus test was significant at P < 0.05, explanatory pairwise comparisons were conducted without further correction of P.
Results
Clinical characteristics
A total of 114 patients with chronic headache (61 males and 53 females; age range 6–16 years; mean age ± SD 10.66 ± 2.05) were studied. Of them, 47 (41%) had TH and 67 (59%) M. Thirty-six subjects were included in the NC group. Demographic and clinical characteristics of the 150 children participating in the study are summarized in Table 1. There was no significant difference between the TH (N = 47), M (N = 67), and non-headache NC children (N = 36) as to age and gender distribution. About three-quarters of the children with headache had a family history of headache, compared with only 13.8% of normal controls. Headache children were also more likely to have had pre-, peri- or immediately postbirth complications. A family history of psychiatric disorders was more common among headache patients, especially the TH group. The socioeconomic status of families was similar in the groups.
Subject demographics and clinical characteristics

test for categorical variables and
In addition to headache, some patients suffered from other conditions, most commonly primary enuresis (N = 18), gastric pain (N = 8), obsessive–compulsive disorder (N = 6), panic attacks (N = 4), and tics (N = 4). These conditions were equally distributed between TH and M.
All the subjects had normal neurological and ophthalmological examinations. A few subjects had brain MRI or EEG tracing, which did not reveal any clinically significant abnormalities.
Psychological symptom ratings
Compared with NC, both TH and M had significantly higher scores on all the administered rating scales (CBCL, CDI, and MASC) except for the CPRS, whose mean score was elevated only for the TH, but not the M children (Table 2). The TH group had higher CBCL (total, internalizing and externalizing) and CPRS scores than the M group. Analysis of the three factors of the MASC indicated higher T scores of Physical Symptoms between TH (62.58 ± 7.60) and M (55.76 ± 9.92) than NC (42.38 ± 6.21, P < 0.001) with no statistically significant differences between TH and M. Likewise, Harm Avoidance scores were greater in TH (50.06 ± 11.79) and M (48.01 ± 9.74) than in NC (35.07 ± 9.42, P < 0.001), with no differences between TH and M. Social Anxiety scores, however, were greater in TH (62.54 ± 11.28) than M (53.21 ± 10.04, P < 0.001), with both headache groups being higher than NC (39.82 ± 12.03, P < 0.001), as shown in Fig. 1.

Multidimensional Anxiety Scale subscores (mean T-scores). TH, Tension headache; M, migraine; NC, normal controls. Significant group differences for each subscale (
Psychological and temperamental ratings (mean ± SD)

Parent Child Behaviour Checklist Total Score (T-scores).
Parent Child Behaviour Checklist Internalizing Score (T-scores).
Parent Child Behaviour Checklist Externalizing Score (T-scores).
Children's Depression Inventory (raw scores).
Multidimensional Anxiety Scale for Children (T-scores).
Conner's Parent Rating Scale (raw scores).
Emotionality–Activity–Sociability–Shyness Scale (raw scores).
Pairwise contrasts were conducted only if the overall P was statistically significant.
In case of multiple comparisons within each scale (i.e. CBCL and EAS), a Bonferroni correction was applied by multiplying the P by the number of comparisons.
Most of the patients, however, had scores within the non-pathological range, according to established norms (Table 3). A higher proportion of TH patients had pathological CBCL total and internalizing scales than NC, while the M group had a higher rate of children in the pathological range only for the CBCL internalizing scale. The number of patients with pathological scores on the CBCL externalizing scale, CDI, and CPRS was too small for the rates to reach statistical significance (Table 3).
Number of children with scores in the pathological range

test with Yates’ adjustment or Fisher's exact test as applicable; P for the three CBCL tests was Bonferroni corrected for multiple comparisons; NS, not statistically significant.
Pairwise contrasts were conducted only if the overall P was statistically significant.
Temperament of children with headache
EAS scale showed that TH children had higher Emotionality and Shyness scores than M children, who did not differ from NC. M children also had higher Sociability scores than TH and NC children (Table 2).
Temperament of first-degree relatives
The EAS scores of the parents and siblings of the probands of this study are shown in Table 4. Mothers of TH children had higher Emotionality scores than M or NC (P < 0.001), and lower levels of Activity than the other two groups. Fathers of TH and M children had higher levels of Activity than NC (P < 0.05). No statistically significant differences among the siblings of the three groups were found after adjustment for multiple comparisons.
Family temperament scores (mean scores and standard deviation of EAS)
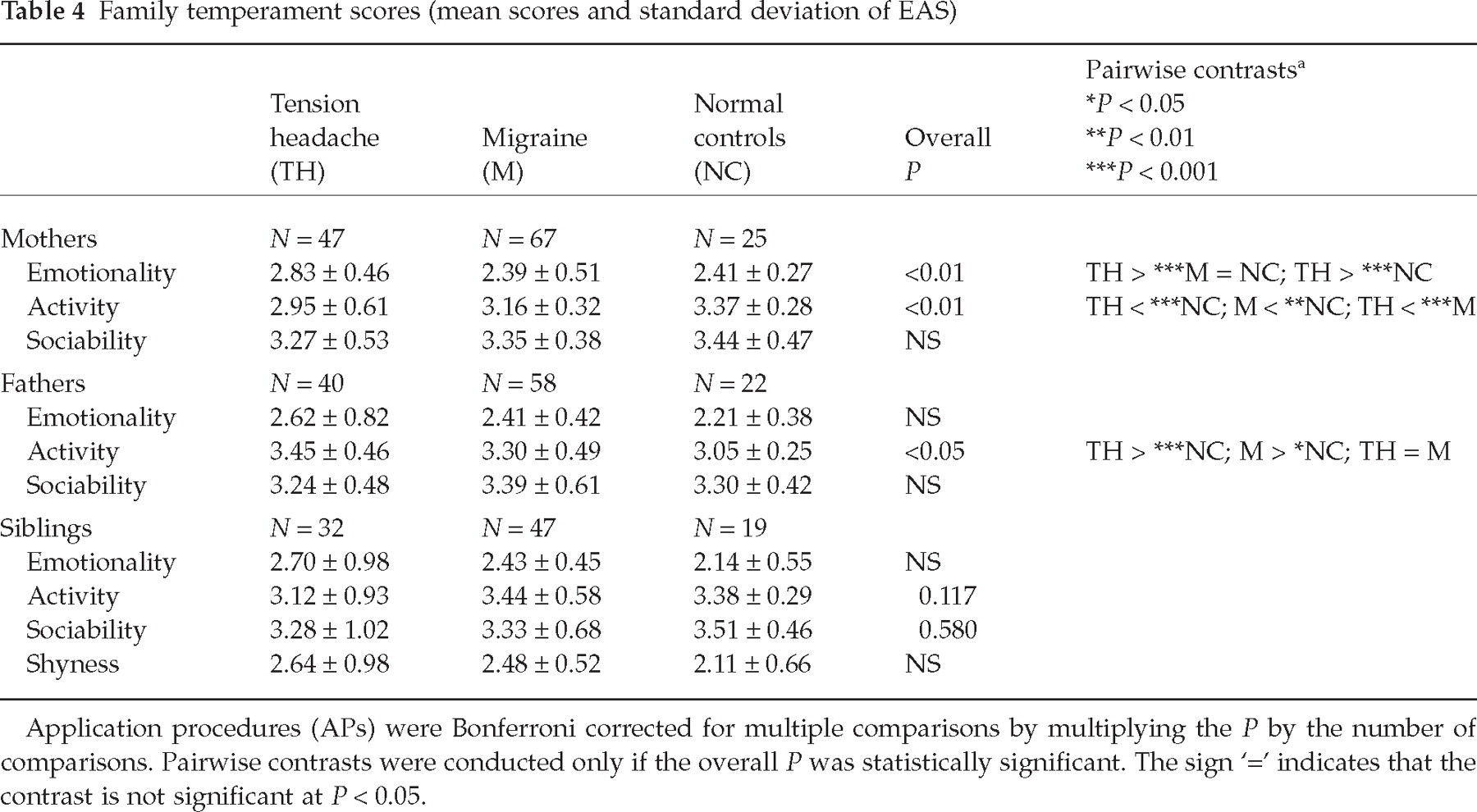
Application procedures (APs) were Bonferroni corrected for multiple comparisons by multiplying the P by the number of comparisons. Pairwise contrasts were conducted only if the overall P was statistically significant. The sign ‘=’ indicates that the contrast is not significant at P < 0.05.
Discussion
We found that indices of behavioural and emotional difficulties (CBCL) and of anxiety (MASC), depressive (CDI) and hyperactivity symptoms were elevated among clinically referred children suffering from TH or M compared with normal peers (Table 2). Most headache patients, however, had behavioural and psychological scores within the normative, non-pathological range (Table 3). The results confirm a significant association between childhood headache and presence of symptoms of emotional and behavioural challenges than children without headache, and are consistent with previous reports (12, 29–33). Future prospective research is needed to determine if behavioural and psychological problems antecede the onset of headache, emerge concurrenly with headache symptoms, or follow the manifestation of headache.
We also found that indices of global, internalizing and externalizing symptoms and hyperactivity were higher among TH children than M children, while depression and anxiety scores did not differ between the two headache groups (Tables 2 and 3). The TH group had higher temperamental traits of emotionality and shyness, and less sociability, than M (Table 2). A higher emotionality score were also found among the parents and siblings of TH children (Table 4). High scores of emotionality and shyness can be considered symptoms of ‘behavioural inhibition’ (34, 35).
School-age children who present with this trait are often irritable, shy, fearful and introverted. Different studies suggest that this temperamental trait increases the vulnerability to depressive and multiple anxiety disorders (36, 37). High Emotionality and Shyness scores on the EAS were reported in youths with anxiety with or without depression, and in their parents and siblings (38).
Taken together, these data suggest that children clinically referred for TH may have, as a group, more behavioural, emotional and temperamental difficulties than children referred for M. Although only a relatively small proportion of headache patients had scores that were actually in the psychopathological range based on normative references, the higher scores indicate the presence of significantly more subclinical behavioural and emotional difficulties than in normal controls.
This finding seems to be in contrast with the conclusions of a recently reported epidemiological study in Finland, which found that psychiatric symptoms tended to be more strongly associated with M than with TH, without any difference, however, in anxiety symptoms (12). The difference in findings can be explained by the fact that our sample was clinically referred and not population based. Our results derived from children who were not representative of children in the general population, but of children who were clinically referred for treatment of primary headache.
One can only speculate on why clinically referred children with TH may be more likely to present with psychological symptoms than clinically referred children with M. It is possible that TH children with concurrent anxiety, depression, behavioural disturbances, or excessive shyness and emotionality are more likely to be clinically referred than TH children without these psychopathological and temperamental features. The symptoms of M, in contrast, may be so distinctive and acute as to trigger clinical referral even in the absence of emotional and behavioural problems.
The interface between headache and psychological symptoms remains unclear and the design of this study does not allow us to distinguish headache-induced psychological difficulties from pre-existing symptoms. The association between headache and indices of behavioural and psychological difficulties that were elevated compared with normal controls, but on average still in the normative range, suggests that headache and psychological symptoms may be related, thus underscoring the need for a broad and comprehensive approach to children referred for headache. Further research is needed to elucidate the mechanism underlying the observed association.
This study has a number of important limitations that must be taken into account in interpreting the data. Most notably, the sample size is relatively small and more appropriate for exploratory analyses than for definitive hypothesis testing. Furthermore, the sample was entirely derived from a single university clinic and may not reflect other academic and non-academic settings. As already pointed out, this was a clinically referred sample and not intended to be representative of children with headache in the general population. Finally, symptom scores were entirely derived from self-report assessment scales completed by the parents or the children themselves. While these rating scales have been shown to be valid instruments for screening children with psychiatric disorders, formal diagnoses of psychiatric disorders cannot be inferred. Since higher scores of Emotionality were found for TH children and their parents, based on parental report, it cannot be excluded that the informant's emotionality affected the ratings of the child, resulting in over-reporting of emotional and behavioural symptoms. Future studies should include data from informants other than the parents or the child, such as, for instance, teacher and clinician ratings.
In conclusion, in a clinically referred sample, both TH and M were significantly associated with elevated indices of behavioural and emotional symptoms, including anxiety and depression. This association was stronger for TH than for M. TH children were also more likely that M to have temperamental traits of shyness and irritability. Larger, more representative, and prospective studies of clinically referred children with headache are needed to clarify the relationship between type of headache and psychological difficulties or temperamental traits.