
Abstract
The authors have published on a unique subset of patients whose headaches worsened in the Trendelenburg position and who on time-resolved MR angiography demonstrated left renal vein compression (nutcracker physiology) with retrograde left second lumbar vein (L2LV) flow and regional spinal epidural venous plexus (EVP) congestion. We hypothesized that the spinal EVP congestion subsequently causes a secondary congestion of the cerebral venous system, which then leads to an elevation of CSF pressure above that individuals CSF pressure set point. This results in a daily headache from onset. Thus, eliminating the spinal EVP could conceivably improve or eliminate the manifested headache syndrome. We now present a case series of four patients with long-term follow-up utilizing lumbar vein coil embolization as a new therapeutic approach. In each patient, the MR angiography findings were verified by catheter-based venography. Treatment consisted of endovascular embolization of the second lumbar vein. Four patients have had coil embolization of which three are 1 year or longer from their procedure while one is 10 months posttreatment. All patients were women. Duration of daily headache prior to embolization ranged from 4 to 8 years. Post-embolization: Three patients are either headache free or 90–95% improved with substantial pain free time. There were no procedure-related complications. Our results suggest that embolization of L2LV in a specific patient population with nutcracker physiology may substantially improve head pain issues. This is a minimally invasive outpatient technique with no apparent side effects.
Keywords
Introduction
There can be multiple reasons why a patient may develop a new onset persistent daily headache. Some of the secondary underlying causes can be readily elucidated with neuroimaging and/or laboratory testing while in others it may represent a quick chronification of their underlying primary headache disorder like migraine. 1 However, in patients without a prior headache history and with normal testing the pathophysiology of the headache may remain elusive. In this circumstance, the patient’s head pain may continue unabated, be treatment refractory and be very disabling. Thus, a continued search for an underlying etiology is needed as treating the cause of headache is more likely to bring headache improvement. The authors have recently published on a unique subset of patients with persistent headaches whose head pain worsened in the Trendelenburg position and who on time-resolved magnetic resonance angiography (MRA) demonstrated left renal vein (LRV) compression by the superior mesenteric artery and the aorta [nutcracker physiology (NP)] with retrograde left second lumbar vein (L2LV) flow and regional spinal epidural venous plexus (EVP) congestion.2,3 Interestingly the patients all possessed NP, but they did not have true nutcracker syndrome (flank pain, proteinuria, and hematuria) just a daily headache.2,4 We hypothesized based on our imaging findings that LRV compression leads to retrograde flow through a valveless L2LV, which then leads to spinal EVP congestion and subsequently causes a secondary congestion of the cerebral venous system, which then leads to an elevation of cerebrospinal fluid (CSF) pressure above that individuals CSF pressure set point. This results in a daily headache from onset. 2 Thus, eliminating the spinal EVP could conceivably improve or eliminate the manifested headache syndrome. Previously renal auto-transplant and other surgical techniques like renal vein transposition were the only treatments available to patients with symptoms related to NP. 5 Renal auto-transplant can carry significant morbidity including infection, bleeding complications, and organ failure as well as a risk of mortality; thus, it is somewhat hard to justify its use in a population whose only symptom of NP is a continuous headache. 6 Looking for alternative treatment possibilities, we theorized that percutaneous embolization of the L2LV may improve or eliminate spinal EVP by redirecting blood to other collateral pathways and thus could possibly alleviate secondary persistent head pain. This would also help to support our hypothesis that spinal EVP leads to persistent headache in a select patient population. 2 The authors recently published a single case report utilizing minimally invasive endovascular lumbar vein embolization as a new therapeutic approach in this specific headache population with a positive outcome, but with only a 5-month follow-up. 7 We now present a larger case series with long-term follow-up.
Design: Case series
Four case patients all presented to an academic headache clinic with a complaint of chronic persistent headache without any pain free time. They were originally seen between 2019 and 2021. They were evaluated and examined by a headache neurologist. All patients were in our original imaging case series which is presented elsewhere. 2 Neurologic examination for all patients was non-focal except the patient’s head pain immediately worsened in a 10°–15° head-down tilt (Trendelenburg position) using a mechanized table. In addition, each patient demonstrated cervical and systemic hypermobility which was verified by a licensed physical therapist. Neuro-ophthalmology examination was negative for disc edema in each patient. Neuroimaging including an magnetic resonance imaging (MRI) brain (with and without gadolinium) and magnetic resonance venogram (MRV) were negative with no mass lesion, Chiari malformation, cerebral vein thrombosis or transverse sinus stenosis noted.
Methods
To be considered for treatment each patient had to demonstrate NP with early retrograde L2LV flow and spinal EVP enhancement on our novel time-resolved MRA technique.2,3 To be considered for coil embolization, the case patients had to be treatment refractory failing at least four headache preventive medications and to be disabled by their headache syndrome. To verify the MRA findings each patient underwent catheter-based venography. Prior to the venogram, the patients consented for the coil embolization with the knowledge that if spinal EVP congestion was found the patient would receive treatment.
Procedure
The full procedure has been described in a previous publication. 7 In brief, while the patient was in the supine position, access to the LRV was obtained through a right internal jugular approach. Venography from the LRV demonstrated retrograde L2LV flow with regional spinal EVP congestion in all treated case patients. No pressure gradient was identified from the LRV to the inferior vena cava due to de-compression of blood into collateral pathways. Embolization of the L2LV was then performed using microcoils. A repeat LRV venogram post-embolization demonstrated no further flow into the L2LV with complete resolution of spinal EVP congestion.
Statistical analysis
This was primarily a descriptive case series, so no statistical analysis was completed.
Results
Four patients have had coil embolization with long-term follow-up. Three patients are 1 year or longer from their procedure while one patient is 10 months posttreatment. All patients were women. Their ages ranged from 19 to 59 years (Table 1). The duration of persistent headache prior to embolization ranged from 4 to almost 8 years (Table 1). In all, the daily headache was described as a constant holocranial pressure/pain sensation. Daily headache intensity averaged a 6/10 on visual analog scale (VAS) for all patients while pain exacerbations averaged 10/10. Post-embolization all four patients have had improvement in their headaches (Table 1). One patient is headache free and discontinued all headache medication. One patient was headache free for several weeks then had headache recurrence. A second embolization was performed to close an additional vein with retrograde EVP flow which developed after the first embolization. She is currently 90–95% improved with most days being completely headache free and requiring only low-dose as needed (prn) usage of acetazolamide if head pressure arises. A third patient was headache free for 5 months off any medication, but then had headache recurrence. 7 She is now 90–95% improved with a substantial amount of daily pain free time on a small dose of acetazolamide, which was ineffective prior to her embolization procedure. Finally, the youngest patient, who also had the longest duration of persistent head pain, has had only a 20–30% reduction in baseline daily pain intensity (from 6/10 to 4/10) with no pain free time. However, she no longer experiences periods of severe pain exacerbation which used to occur multiple times per week, thus her quality of life has improved. This patient had the least amount of NP on imaging. Of the three patients with the most improvement in headache, two awoke the day after the procedure with no pain, while a third was 75% improved within 48 h, experiencing periods of pain freedom. These three patients all developed a daily persistent headache at age 40 years or older (Table 1). There were no side effects from the procedure or procedure-related complications. Recovery time was brief and within several days, the patient’s felt back to their normal baseline. Three of our patients had follow-up venography 6 months post-embolization, and this confirmed no further abnormal retrograde flow through the L2LV.
Results of lumbar vein coil embolization.

Case presentations
Two of our treated case patient histories are presented.
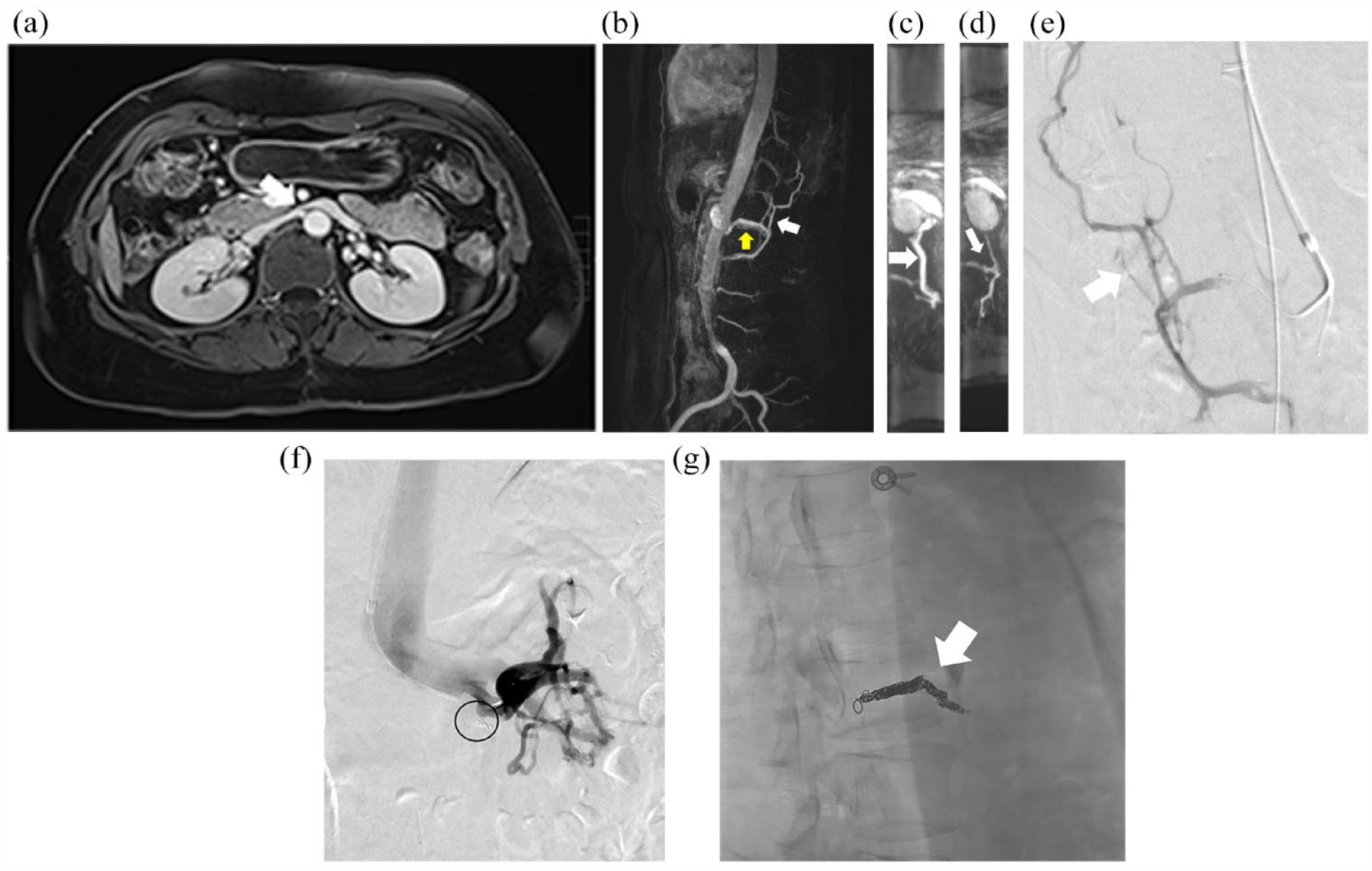
Patient 2 (Table 1): A 44-year-old woman with a history of episodic migraine presented with a daily persistent head pressure sensation for 2.5 years. This started daily from onset and was possibly triggered by airline travel. She awoke one day with the head pressure/pain, and it never ceased. It was always worst first thing in the morning, laying supine, bending over, and always exacerbated by exertion. She denied migrainous features with her holocranial pressure headache. It did feel as if her head was going to explode. Prior treatments included topiramate up to 150 mg/day with some benefit but no pain free time, low-dose naltrexone, tizanidine, amitriptyline, duloxetine, and daily indomethacin. Neuroimaging including an MRI brain and MR venography were read as normal. On exam she demonstrated cervical and systemic hypermobility. In the Trendelenburg position, she had immediate worsening of her baseline head pressure. She was started on acetazolamide and while she had some benefit, she could not tolerate dosing above 750 mg per day. Trial of onabotulinumtoxinA (migraine protocol) was ineffective. Rimegepant helped her intermittent migraines but did not affect the daily head pressure. Around this time, we started investigating patients with daily persistent headache and worsening in Trendelenburg for NP. The patient underwent a time-resolved MR angiography of the abdomen which demonstrated a moderate compression of the LRV by the superior mesenteric artery with evidence of retrograde flow through the L2LV and opacification of the EVP suggesting spinal EVP congestion [Figure 1(a)–(b)]. Because of the refractory nature of her headaches and the possible connection to NP, the patient underwent catheter venography 2 years after we first met her and 5 years and 3 months from the onset of her daily headache. On venography, the L2LV demonstrated retrograde flow into the spinal EVP [Figure 1(c)-(d)]. Post-embolization of L2LV, no further retrograde flow was demonstrated [Figure 1(e)]. Within 48 h, the patient felt dramatic improvement in her head pressure, so much so she began to exercise and lift weights again without exacerbation. By 1 month post-embolization her head pressure completely alleviated, and she remains headache free through 1 year follow-up. She still gets intermittent migraine. Her quality of life has completely changed.

(a) Contrast-enhanced MRI at the level of the renal veins demonstrates a beaked appearance of the left renal vein (white arrow) as it crosses between the superior mesenteric artery and aorta. (b) Time-resolved contrast-enhanced MRI angiogram demonstrates retrograde flow through the left lumbar vein (white arrow) with opacification of the EVP (yellow arrow). (c) Left renal vein venogram demonstrates retrograde flow through the left second lumbar vein with opacification of the EVP (white arrow). (d) Venography with the catheter tip in the left second lumbar vein demonstrates retrograde flow with opacification of the EVP (black arrows). (e) Post-embolization venogram from the left renal vein demonstrates no further opacification of the lumbar vein or the epidural venous plexus. Microcoils are seen in the lumbar vein (black circle).
Patient 3 (Table 1): The patient was 58 years of age when she presented to our clinic for headache consultation. She had no headache history until 13 months prior when she began to experience a daily headache from onset. The initial headache started during the day, was non thunderclap in temporal profile and in the beginning was occipital nuchal in location but progressed to a holocranial pressure/pain. There were no migrainous associated symptoms. She also remarked that it felt like her head wanted to explode. She was at her worst when laying in a supine position and first thing in the morning. Prior to her evaluation at our clinic, she had some moderate improvement on acetazolamide 500 mg two times per day. She also had a lumbar puncture with a normal opening pressure of 17 cm H2O and with brief improvement of head pressure postprocedure. Prior failed therapies included: gabapentin, topiramate, baclofen, amitriptyline, acetazolamide, onabotulinumtoxinA, erenumab, and for a period of time daily opiates. On examination, she had evidence of cervical and systemic hypermobility. She had a dramatic and immediate worsening of her baseline head pressure in the Trendelenburg position. Her presentation suggested she may have an abnormal reset of CSF pressure to an elevated state.1,7 The patient was tried on spironolactone and then acetazolamide with some benefit but never had any pain free time. A specialized MR angiography of the abdomen showed severe compression of the LRV as it traversed beneath the superior mesenteric artery [Figure 2(a)]. There was an enlarged L2LV with marked opacification of the spinal EVP suggesting congestion [Figure 2(b)–(d)]. From the time of this imaging to the time of her venogram and coil embolization was 13 months, during which she was very disabled by her headaches. She was 4 years and 2 months since the onset of her headaches [Figure 2(e)–(g)] The day after embolization, she awoke headache free (the first time in four plus years), and she continued with pain freedom for about 2 weeks with immediate headache recurrence back to her baseline. It was then decided to complete a follow-up venogram to determine if any new venous collaterals developed post-embolization, which could account for additional retrograde flow into the EVP from the NP. This was completed 5 months after the original venogram. The study demonstrated no evidence of retrograde flow into the EVP from the LRV suggesting the original embolization was still successful. A catheter into the very proximal non-embolized portion of the second lumbar vein did however demonstrate a small amount of flow toward the spine from a venous collateral with possible opacification of the EVP; thus, this vein was embolized with GELFOAM [Figure 3(a) and (b)]. She is now 8 months from the second embolization and 1 year plus from the initial procedure and is basically pain free. Most of the time she is off any medication but occasionally, she feels her head pressure rising so she takes 125–250 mg prn of acetazolamide to alleviate the exacerbation. Her quality of life has been substantially improved.
(a) Contrast-enhanced MRI at the level of the renal veins demonstrates compression of the left renal vein (white arrow) as it crosses between the superior mesenteric artery and aorta. (b) Time-resolved sagittal contrast-enhanced MRI angiogram demonstrates retrograde flow through the left lumbar vein (yellow arrow) and early opacification of the EVP (white arrow). (c) Axial reformat of the time-resolved dynamic contrast-enhanced MRI angiogram demonstrates retrograde flow through the L2LV (white arrow). (d) Axial reformat of the time-resolved dynamic contrast-enhanced MRI angiogram demonstrates early opacification of the EVP (white arrow). (e) Venography with the catheter tip in the left second lumbar vein demonstrates retrograde flow with opacification of the EVP (white arrow). (f) Venography from the left renal vein demonstrates no further opacification of the lumbar vein or the EVP. Coils can be seen within the lumbar vein (black circle). (g) Lateral radiograph demonstrates coils along the length of the lumbar vein (white arrow).

(a) Venography from the left renal vein near the origin of the left second lumbar vein (previously embolized) demonstrates development of a new collateral vein (black arrows) providing retrograde flow to the EVP. (b) Post-embolization lateral radiograph demonstrates the previous microcoils in the left second lumbar vein (white arrow). The new collateral vein was embolized with GELFOAM (black arrow).
Discussion
We present a possible new therapeutic advance in the treatment of a secondary daily persistent headache in a specific patient population with underlying NP and secondary spinal EVP congestion. Their syndrome is marked clinically by a daily persistent headache from onset, a sense of holocranial head pressure which worsens in a supine position, is typically worst first thing in the morning and worsens with exertion. The headache is quickly exacerbated in the Trendelenburg position, which causes an immediate rise in cerebral intracranial pressure.8–10 All of these clinical symptoms and the worsening in head-down tilt is suggestive of a state of elevated CSF pressure. 11 The issue for our patients was what caused the rise in CSF pressure was not easily elucidated by neuroimaging, and only 25% of the patients were overweight. 2 In regard to diagnostic criteria, all of our patients originally met the International Classification of Headache Disorders, 3rd Edition (ICHD-3) criteria for new daily persistent headache (NDPH) because an underlying secondary cause could not be identified. 12 As currently presented, they no longer reach primary headache criteria and would now be considered a secondary headache condition presumably from the renal vein issues. It was a single case report of a patient with daily persistent headache and nutcracker syndrome who gained headache relief with renal auto-transplant plus the work by Scholbach suggesting midline venous congestion issues as a cause of the clinical features of nutcracker syndrome including headache that suggested to the authors that we should be looking for abdominal venous compression syndromes, specifically NP in some of our patients with specific clinical symptoms and a worsening in head-down tilt.13,14 We have subsequently published on a series of patients, utilizing a novel time-resolved MR angiography technique, that was able to identify patients with spinal EVP congestion.2,3 We then hypothesized that the spinal cord venous plexus engorgement secondarily led to cerebral venous congestion and that caused the patient’s CSF pressure/volume to rise above a pain threshold point leading to a daily persistent headache.2,15 Three of our patients had lumbar punctures with opening pressures (17–23 cm H2O) falling within the established normal range of 10–30 cm H2O (Table 1). 16 They all however improved with CSF volume removal although headache improvement typically lasted for only hours to a single day. We had one outlier (patient 1) who had headache resolution for 4 weeks. The theory is that all individuals appear to have their own unique set point of CSF pressure/volume that they are adjusted too and anything that alters that set point even by minimal amounts (high or low), and even with CSF opening pressures considered within the normal range, can produce a persistent headache for that individual.2,15 NP is one potential manner by which CSF pressure may be elevated toward the pain threshold point, and once reached, it can present as a daily headache out of the blue that can remain persistent as the patients theoretically cannot reset their CSF pressure/volume on their own secondary to their abnormal renal vein anatomy. It appears that in some individuals, this pain threshold event occurs without a defined trigger while in others seemingly innocuous events like riding in an airplane or visiting a location with higher altitude, or having a strong Valsalva can elicit the onset.2,15,17 All of these scenarios could potentially raise the patient’s baseline CSF pressure. We then surmised that if we could alleviate the spinal EVP by stopping venous influx through a dilated, valveless L2LV, we could possibly improve or completely alleviate the patient’s headache syndrome. We also wanted to avoid renal auto-transplant or other surgical procedures, if possible, because of the morbidity associated with these procedures and because we were dealing with a patient population who only presented with headache and not true nutcracker syndrome; thus, surgical adverse events seemed unwarranted in this population. We now present the first case series of lumbar vein embolization. This technique appears to permanently shut off spinal EVP via the L2LV. Overall, three of our four patients have had a dramatic improvement in their head pain syndrome, whereas our fourth patient is also better as she is no longer experiencing periods of pain exacerbation and her baseline pain intensity has decreased. Three of our treated patients have achieved either complete pain freedom or have a substantial amount of pain free time. None of them with any previous medication or procedure had achieved pain free status. This has not only been a very positive clinical outcome, but we also believe has potentially proven our hypothesis that NP-induced spinal EVP is the underlying etiologic cause of persistent daily headache in this secondary headache subtype. It makes the point that treating the underlying cause rather than the symptoms is imperative for successful headache treatment efficacy. Thus, an exhaustive approach even looking outside of the central nervous system (CNS) maybe necessary to determine the underlying etiology of headache. 1 Although this is a small patient cohort, we do have follow-up data greater than 1 year, suggesting the treatment is not only effective but also durable. Importantly, all our patients have a hypermobility syndrome (some reaching Ehlers–Danlos criteria). This patient population seems to be uniquely predisposed to developing abdominal venous compression issues including nutcracker phenomenon and May–Thurner venous physiology. 18 How common NP is in the hypermobile population and especially in the daily persistent headache/hypermobile population needs to be determined. It is important to note that from our small investigations so far, the majority of patients with daily headache and NP do not have congestion of the spinal EVP and thus some other cause for their headaches needs to be elucidated.2,3
From our current case series, it appears that early dramatic improvement post-embolization procedure maybe a positive predictive factor for long-term improvement. This may suggest that immediately post-embolization there are no other secondary collaterals present causing spinal EVP congestion, but as we saw with patient 3 (Table 1), collaterals may develop with headache recurrence.
Implications for clinical care
We appear to be the first group to utilize abdominal venous coil embolization, specifically for the treatment of headache. This technique, however, has been employed in various other abdominal venous compression disorders including pelvic congestion syndrome.18,19 Cerebral venous insufficiency/congestion has already been linked to various headache disorders including idiopathic intracranial hypertension, cough headache, exertional headache as well as NDPH.20–23
Most importantly, our minimally invasive technique, completed in an outpatient setting, offers an effective treatment without the need of surgical intervention (renal auto-transplant, renal vein transposition), which can cause significant morbidity and prolonged recovery time. Not only do our patients go home the same day, but they can also show relief of their refractory headache within 24–48 h. In addition, they are back to normal activity within 1–5 days.
Conclusion
For some selected headache patients with specific symptoms and a worsening of headache in the Trendelenburg position, investigation for NP and spinal EVP should be performed. Outside of this specific patient population, looking for these secondary venous compression issues in some treatment refractory patients with suspected NDPH may also be suggested. Our case series demonstrates that embolization of L2LV in the setting of LRV compression, retrograde L2LV flow, and regional spinal EVP congestion may greatly improve persistent headache. Lumbar vein embolization is a minimally invasive outpatient technique with no apparent side effects. It is less morbid than standard of care surgical techniques. Further prospective studies are now needed to confirm our results.