
Abstract
In this study, the causes, predisposing factors and clinical features of chronic daily headache in children and adolescents were studied within the population of patients attending a specialist headache. The International Headache Society's (IHS) criteria for the diagnosis of chronic tension type headache (CTTH) were assessed for their applicability in the paediatric age group. Over a period of three years, demographic and clinical data were collected prospectively on all children who attended the clinic and suffered from daily attacks of headache.
One hundred and fifteen children and adolescents (32% of all clinic population) had chronic daily headache, of whom 93 patients (81%) fulfilled the IHS criteria for the diagnosis of CTTH. They were between 3-15 years of age (mean: 11.1, SD: 2.3) and their female to male ratio was 1.2: 1. Around one third of the patients also suffered from migraine (mainly migraine without aura).
The headache was described as mild in 60.9%, moderate 36.5% and severe 2.6%. Headache was located at the forehead in 53% or over the whole of the head in 29.6%. Pain was described as ‘just sore’ or dull by 73.9%. During attacks of headache, at least half the patients reported light intolerance, noise intolerance, anorexia or nausea. Thirty-two percent of patients had at least one underlying chronic disease that may have contributed to the pathogenesis of the CTTH. Eleven percent had serious stressful events related to family illnesses and in four patients headaches were triggered by family bereavement. Fourteen percent were investigated with neuroimaging and 22% were referred for clinical psychology assessment and management.
In conclusion, CTTH is a common cause of headache in children attending a specialist headache clinic. The clinical features closely match those of adult population and the IHS criteria for the diagnosis of CTTH can be adapted for use in children. Predisposing stressful risk factors, physical or emotional, are present in a large proportion.
Introduction
Chronic tension-type headache (CTTH) is characterized by spells of almost daily attacks of headache and is the most common cause of chronic daily headache. Organic causes of chronic daily headache are rare in children and adolescents and may include brain tumours, benign intracranial hypertension and ocular refraction errors (1). In a small number of patients other underlying causes may include psychiatric illnesses or misuse of analgesia (2).
The International Headache Society (IHS) defined chronic tension type headache in adult patients as attacks of headache that occur on at least 15 days per month over a period of at least 6 months (3). The headache is described as mild to moderate in severity, pressing or tightening in nature, bilateral and does not worsen on physical activities. Headache may be associated with nausea, photophobia or phonophobia. Clinical studies suggest that chronic daily headaches is not a single uniform entity, but full and accurate subclassification is still needed (4). A study of the characteristics of 100 consecutive adults with daily headache referred to a headache clinic found that 39% of the patients had migraine symptoms, despite having daily headaches. Initial onset of headache peaked in the second decade of life, but headaches did not become a daily occurrence until much later (5).
The prevalence rate of CTTH in the general adult population is reported between 1.5 and 7% (6–8). with the majority of patients being females. Severe attacks of daily headache are less common and were reported by 0.5% of a population sample of around 20 000 people in the USA (9). Among patients attending headache clinics CTTH is a common disorder affecting about 30–75% of all the headache patients (10–12).
The prevalence rate of CTTH in children is uncertain. Population-based studies are limited by their use of variable definitions and diagnostic criteria. The prevalence rate of CTTH, as defined by the IHS criteria, was estimated at 0.9% in a population-based study of schoolchildren between 5 and 15 years of age in Aberdeen, Scotland (13). The prevalence rate of childhood CTTH in other populations and in primary care is not known. However, a study of headache in Dutch general practice found 5.7% of all children, consulting their general practitioners because of headache, suffer either episodic or chronic tension headache (14). In hospital practice, between 5 and 7% of all children attending paediatric neurology or specialist clinics, with headache as their main complaint, suffer from CTTH (15, 16).
The clinical features and causes of chronic daily headache in children are probably different from those in adults. It is suggested that daily headache in adults may have been transformed into daily pain episodes from either episodic tension headache or migraine. Chronic daily headaches have been classified in adults into the following four categories: transformed migraine, chronic tension-type headache, new daily persistent headache, and hemicrania continua (17). In children, such phenomenon has not been identified, but intermittent migraine was associated with CTTH in 35% of patients with no transformation of migraine symptoms were observed (18).
Assessment of the clinical features of CTTH in children and adolescents has been so far limited to a few small studies. A recent study reported on 30 children with CTTH and did not find any age-related differences in the associated symptoms between younger children under the age of 10 years and adolescents over the age of 11 years (19). A larger study, recruiting patients from 21 centres in Italy, reported clinical findings on 156 children with CTTH (16).
The results of this study suggested that the number of headache episodes required for fulfilling the criteria for the diagnosis of CTTH in children and adolescents should be reduced from 15 to less than 10 per month. On the other hand, the paediatric committee of the American Association for the Study of Headache suggested that the headache frequency should be at a minimum of 5 days per week. The committee has also noted the variability of both the location and severity of pain in children (20). Association with significant psychopathology and disability were found to be of particular problem in children and adolescents in a study of 37 patients with CTTH (21).
Large detailed studies of chronic daily headache in children and adolescents are necessary due to its rare occurrence in the general childhood population and the relatively small number of patients seen in primary care or even in general paediatric clinics. Therefore, this study attempts to address important issues in relation to the causes of daily headache, the clinical features, the criteria for the diagnosis of CTTH, the relationship with other headache disorder, other organic illnesses, emotional or psychological difficulties and family stresses and anxieties.
Patients and methods
All patients attending the specialist headache clinic over the initial period of 3 years were studied prospectively. All patients were assessed within the department of paediatric neurology and the headache diagnoses were made on the basis of the IHS criteria. The diagnosis of CTTH was evaluated against the IHS criteria for the diagnosis of chronic tension headache (Table 1). Information regarding the child's age, sex, age of onset of headache, frequency, duration, severity, quality and location of headache and associated symptoms (anorexia, nausea, and vomiting, light intolerance and noise intolerance) were documented. Also information about other present personal or family illnesses in the household were collected. The source and reason for referral, previous investigation and treatment were also recorded. Also recorded were the investigations, management and referrals to other specialists. Patients' clinical details and demographic information were entered onto SPSS computer programme for analysis.
IHS criteria for the diagnosis of chronic tension-type headache

Results
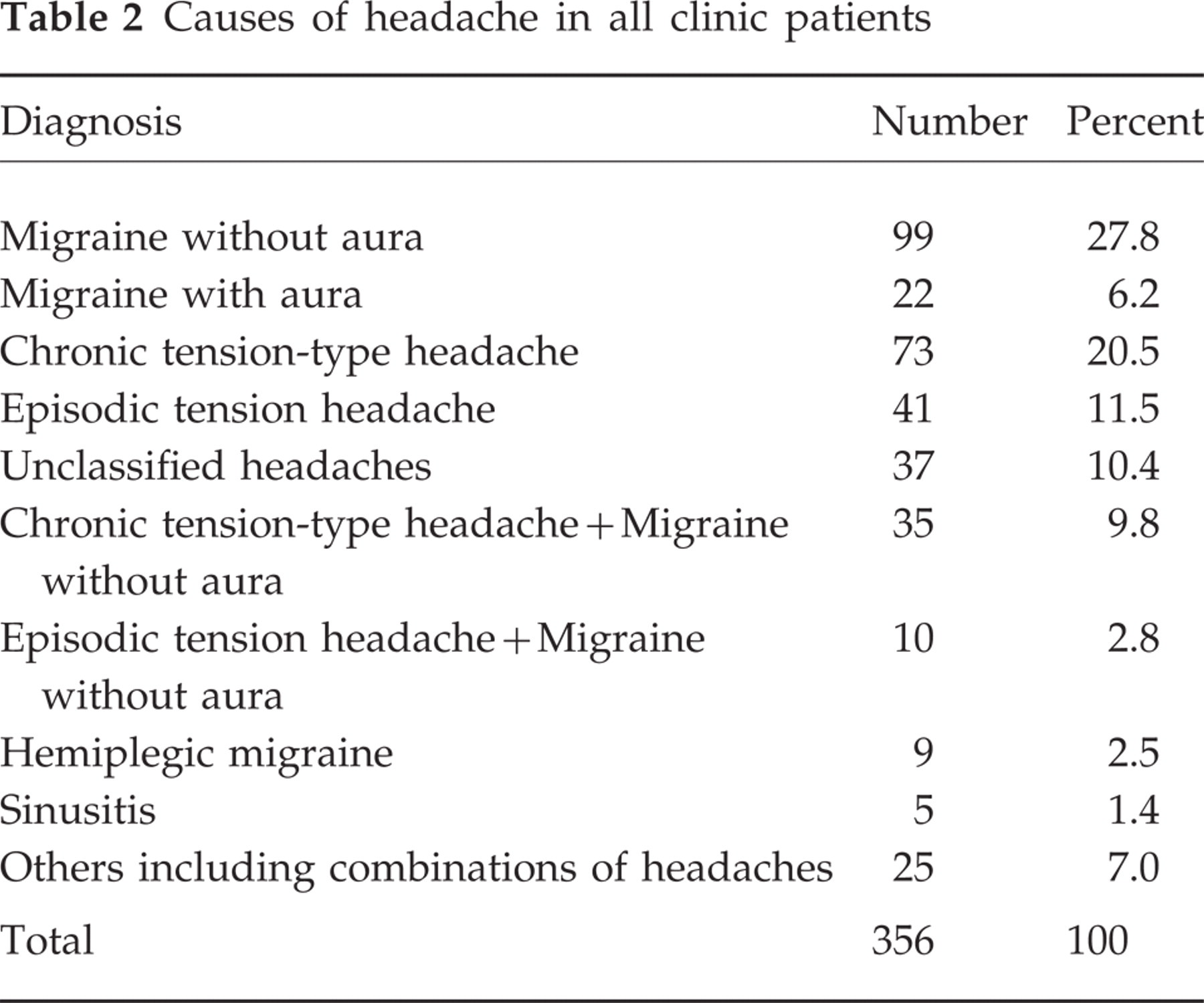
Three hundred and fifty-six children and adolescents were fully assessed at the headache clinic during the three-year period 1996–99. Migraine and tension-type headaches were the main causes of headache in this clinic population (Table 2).
Causes of headache in all clinic patients
Patients with chronic daily headache
One hundred and fifteen children and adolescents presented to the clinic with almost daily headache attacks. There were 63 female and 52 male patients with a ratio of 1.2 : 1. Mean age at presentation was 11.1 years (range: 3.3–15.8 years,
CTTH was the only type of headache in 73 children (63.5%). Other patients had mixed types of headache including 35 patients (30.4%) who suffered from CTTH and migraine without aura, 5 patients (4.3%) had CTTH and analgesia-induced headache, 1 patient had CTTH and migraine with aura and 1 patient had CTTH and jolting headaches. Eighty patients (69.6%) were referred to the clinic by their own general practitioners. About one third of patients (30.4%) were tertiary referrals from specialist paediatricians. The main reasons for referral were uncertain diagnosis and poor response to antimigraine treatment and prophylaxis.
Clinical features
The mean duration of headache disorder was 22.6 months (
The pain was described as mild (not interfering with normal daily activities) in 69 patients (60%), moderate (interfering with some, but not all activities) in 42 (36.5%) and severe (stops all activities) in only 4 patients (3.4%). Two of the 4 patients who described their headaches as severe were known to suffer from migraine as well. In the majority of patients, the pain was located at the forehead (53%) or the whole of the head (29.6%). Other sites were also described, but only occasionally (Table 3). Sixty-five patient (56.5%) were either unable to describe the pain or referred to it as ‘just sore’. The pain was described as dull in nature by 20 (17.4%) patients, throbbing by 17 (14.8%), tightening or pressure by 7 (6.1%), stabbing by 3 (2.6%), sharp by 2 (1.7%) and heaviness by 1 (0.9%) patients.
Site of pain

Application of the IHS criteria for the diagnosis of CTTH
In 93 patients (81%) the headache attacks were either not associated with nausea, light intolerance or noise intolerance (58 patients; 50.5%) or had no more than one associated symptom (35 patients; 30.4%) therefore fulfilling the IHS criteria for the diagnosis of CTTH. In 22 patients the headache attacks were associated with a combination of two symptoms of light intolerance, noise intolerance or nausea (Table 4).
Associated symptoms during attacks of headache in patients with CTTH

Predisposing risk factors
A total of 59 patients (51%) had at least one significant personal health problem, family illness or stressful family event that preceded or coincided with the onset of CTTH.
Twenty-six patients (22.6%) had significant chronic neurological or psychological disorders: Fourteen had neurological diseases (2 had epilepsy, 4 past head injury, 2 sensorineural hearing loss, 1 dysmorphic syndrome, 1 surgically corrected craniosenistosis, 2 learning difficulties and 2 paroxysmal vertigo). Twelve patients had significant behavioural problems requiring psychological assessment including 2 patients with depression and 2 patients with habitual tics.
Nine patients (7.8%) had serious or life threatening chronic diseases including renal failure (3 patients), congenital heart diseases (2), diabetes mellitus (1), leukaemia (1), craniopharyngioma and hypopituitarism (1) and cystic fibrosis (1).
Nine patients (7.8%) had emotionally distressing chronic physical disorders including chronic skin diseases; ichthiosis (1 patient), short stature (4), obesity (3) and chronic constipation (1). Fifteen patients also suffered from and received treatment for asthma, but were not considered of significant impact on the children's attitude and psychology.
Eleven patients (9.6%) had serious stressful events relating to family illnesses. The mothers of 4 patients were seriously ill (2 mothers had severe depression, 1 mother had neurological disability and 1 had cancer). The mother of a fifth patient died following an illness. The fathers of 4 children had physical disabilities due to multiple sclerosis (1), late treated craniosenistosis (1), road traffic accident (1) and glaucoma (1). Both parents of one patient were chronically ill and a sibling of another patient suffered from chronic fatigue syndrome.
Four patients had their headaches triggered by recent family bereavement (death of a grandparent).
Family history of headache
The mothers of 20 patients (17.5%) also suffered from recurrent headache (13 had tension-type headache and 7 had migraine). The fathers of 7 patients (6.1%) had headaches (3 had tension headache and 4 had migraine).
Investigations
A total of 17 patients (14.8%) were investigated with neuroimaging (either computerized tomography or magnetic resonance imaging of the brain) in the process of headache evaluation. All brain scans showed normal results. Eleven of them had brain scans before attending the headache clinic (31% of the 35 patients who attended the clinic as a tertiary referral). Six had neuroimaging as part of their clinical assessment at the headache clinic (7.5% of the other 80 patients).
Pre-referral treatment
Most of the children and adolescents treated their headaches with simple analgesics before attending the clinic. Most of the medications were bought over the counter and only a few were on prescription. The common analgesics were paracetamol, ibuprofen and rarely codeine. Seventeen (23.3%) of the 73 children who had CTTH as their only headache disorder, were treated with specific antimigraine prophylactic medications (15 were given pizotifen and 2 propranolol). One child with mixed CTTH and migraine without aura was given sumatriptan tablets, but without been aware of the coexistence of the two conditions.
Headache clinic management
Most patients were treated successfully simply by reassurance about the benign nature of the condition and the absence of sinister cause for the headache. Making the diagnosis of CTTH was the first step in starting the appropriate management of the headaches. Medical treatment was mainly by simple analgesics in 91.3% using paracetamol or ibuprofen in appropriate dosages and frequency for age and body weight. In 8 patients (7.0%) cessation of analgesia was advised to treat or prevent analgesia-induced headache. Two patients (1.7%) were treated with 4 and 8-week courses of regular low dose aspirin. Patients were asked to fill in clinical diaries to confirm clinical features of the headache disorder and to monitor response to treatment.
Clinical psychology intervention
Twenty-five patients (21.7%) were referred for further assessment and management within the department of clinical psychology. Patients were interviewed and counselled by trained clinical psychologists who gave them training sessions in mental and physical relaxation, biofeedback and pain management strategies.
Outcome
Fifty-eight patients (50.4%) were discharged back to the care of their referring physicians after reassurances regarding the diagnosis and the plan of management was drawn up. Twenty-five patients (21.7%) were followed up at the departments of clinical psychology and 17 (14.8%) patient were still under active reviews. Twelve patients (10.5%) have either cancelled their appointments due to remission of the symptoms or failed to attend subsequent clinic appointments for no known reason. Only 3 patients (2.6%) were re-referred to the clinic 12–24 months following discharge.
Discussion
A little is known about chronic daily headache in children and adolescents. Paediatricians and paediatric neurologists have started, over the past 10 years, to recognize and study the disorder. The current paediatric knowledge is based mainly on studies, reports and definitions of the disorder derived from the adult headache literature. In the 1988 IHS classification of headaches, separate entries were made for childhood migraines, but none for the episodic or the chronic subgroups of tension-type headache. Therefore, researcher used and adapted the IHS criteria for the diagnosis of tension headache in children. As a result of the limited knowledge about CTTH in childhood it was not surprising to see that the diagnosis of CTTH in those children, was not even considered by the referring physicians.
The fact that around one third of the patients also suffer from migraine is not surprising and should not be taken to represent a separate group of patients. Migraine is a common disorder with a relatively high prevalence rate in schoolchildren that may reach 20% in the teenagers (13). Also migraine is a chronic painful disorder that like all chronic diseases may become a predisposing risk factor for developing chronic tension headache. Therefore, it may be reasonable for the time being, at least, to consider patients with CTTH who also suffer from migraine as patients with mixed headaches. This distinction is very important in making clinical assessment, planning and monitoring response to treatment and educating patients. It is also of great importance to distinguish between types of headache when using specific antimigraine therapies. Data from this study of youngsters did not provide any evidence to support the notion that daily headache might have evolved from episodic tension headache or migraine. However, neither migraine nor episodic tension headache in children reaches a degree of chronicity comparable to that in adults to allow such an observation.
The clinical characteristic features of the 115 children and adolescents, presented in this study, suggest that the IHS criteria may be appropriate for clinical use and research purposes in children and adolescents with some minor modifications. Analysis of the clinical features suggests that the frequency of attacks has always been consistent. Spells of daily attacks of headache were seen in all patients. Each spell may last from one week every fortnight to almost constant headache over 1–2 months. Some children had spells of infrequent headache reaching a minimum of 8 days per month, but only to revert to high frequency headache attacks at other times. The diagnosis therefore should take into account an assessment over a prolonged period of time to correct for the fluctuation in frequency and duration of attacks, which seem to be of particular significance in children and adolescents.
The use of headache diaries has also helped to clarify some difficulties in reporting headache symptoms in children. Problems in clinical setting may arise from the tendency of children and their parents to describe the worst and most recent attacks of headache rather than all the attacks. Only by using diary recording during the time of headache accurate information can be collected and proper diagnosis can be made.
The severity of headache, as defined by the ability to continue with normal activities, is also consistent with that observed in the adult population. Only rarely children reported attacks that were severe enough to stop all activities, but even within this small group of 4 children, severity fluctuated between mild, moderate and rarely severe.
Concerning the number of associated symptoms in criterion C (2), 93 patients were within the IHS definition of no more than one associated symptom. However 22 patients (19.1%) fulfilled the rest of the criteria and followed the same clinical course of disease as the rest of the group. Only 2 of these children had headache that was described as severe and both of them also suffered from migraine. The daily headaches of the remaining 22 patients were typical, otherwise, of tension headache as confirmed by the accurate information obtained from the headache diaries and were similar to those of the larger group of 93 patients who fulfilled the criteria for the diagnosis of CTTH. Therefore, it is appropriate to adapt the diagnostic criteria to allow the presence of at least two symptoms of the three during attacks of headache in the paediatric age group. Variations from the IHS criteria have also been observed to a greater degree in adult patients. In a study of 100 patients with CTTH, 32 patients reported severe attacks, 29 reported throbbing quality of headache and 7 had unilateral headache (in 2 unilateral was the only location of headache described) (5).
Predisposing risk factors for CTTH seem to be specific for children and adolescents. Over half the children in this study suffered or were exposed to stressful events after or around the time of the onset of headache. The assessment of CTTH in children and adolescents should always include the search for obvious and salient risk factors. Health related risk factors are of great importance including potentially life-threatening conditions, disabling diseases or psychologically disturbing conditions. It is possible that these patients represent a highly selected group of children and adolescents with CTTH, attending a tertiary centre for headache. Therefore, population-based and primary health care studies of headache in children and adolescents are necessary to confirm these observations.
Providing a positive diagnosis based on specific clinical criteria has helped and facilitated the management of CTTH in this group of children and adolescents. Complete physical and neurological examinations have also contributed to the reassurances given to the patients and their parents. Therefore, the need for brain neuroimaging was limited to only a small number of patients. Medical treatment was also limited to either withdrawing analgesics in children with analgesia-induced headache or by the judicial use of paracetamol or ibuprofen in appropriate dosages and frequency. Clinical psychology assessment and treatment was an essential part of the management of almost one in five of the patients with CTTH. Multidisciplinary approach is necessary and may involve educational psychologists, the parents, the general practitioners and other community services.
In conclusion, this study of 115 children and adolescents has shown that CTTH is a common problem in children attending hospital clinics for headache as their main complaint. Children and adolescents with chronic diseases and stressful family events are probably at a higher risk of developing CTTH. The management is multidisciplinary in nature and investigations can be limited, if complete clinical history and physical examination have been carried out. The positive use of the diagnosis, based on appropriate definition and diagnostic criteria will help in understanding the child's disease and will also help in planning future research into childhood CTTH.
The IHS criteria for the diagnosis of chronic tension headache can be adapted to serve as an adequate tool for clinical use and possibly for research into childhood daily headache. Specific criteria for childhood CTTH, and tension headache in general, need to be included in the IHS classification of headaches. The IHS criteria for the diagnosis of CTTH in children should allow for at least two associated symptoms during the attacks of headache.