
Abstract
New daily persistent headache (NDPH) is a subtype of chronic daily headache. The literature on NDPH is scant and its true aetiology is unknown. A retrospective chart review was carried out from a computerized database at the Jefferson Headache Centre from August 1997 to May 2000 to identify patients with NDPH using the Silberstein et al. criteria. Forty women and 16 men were identified. Age of onset ranged from 12 to 78 years. The peak age of onset was the second and third decade in women and the fifth decade in men. Eighty-two per cent of patients were able to pinpoint the exact day their headache started. Onset occurred in relation to an infection or flu-like illness in 30%. A prior headache history was found in 38% of patients. A family history of headache was documented in 29%. The duration of daily headache ranged from 1.5 h to 24 h; 79% were continuous. Nausea occurred in 68% of patients, photophobia in 66%, phonophobia in 61%, and lightheadedness in 55%. Laboratory testing and neuroimaging in all patients was normal except for Epstein-Barr virus antibody titres, which were positive in 71% of seven patients tested, representing past infection. NDPH appears to be a female-predominant disorder, marked by a continuous daily headache with associated migrainous symptoms. Over 80% of patients could state the exact date their headache began. One-third of patients developed NDPH with a flu-like illness.
Introduction
New daily persistent headache (NDPH) is a newly recognized subtype of chronic daily headache (CDH). The syndrome was first described in 1986 as a benign form of CDH, as most patients improved without therapy (1). Sadly, patients with NDPH, at least those that reach the physician's office, have a disorder that is anything but benign. It is the opinion of most headache specialists, that this form of CDH is one of the most refractory to treatment. Manuscripts on NDPH in the literature are sparse and the true clinical characteristics of this syndrome have not been adequately documented. It is well recognized that NDPH is a headache that starts daily from onset, typically in a patient without a history of headache, but little more is known of the syndrome.
Methods
A retrospective chart review was carried out using a computerized database of patients from the Jefferson Headache Centre (a large university-based headache specialty unit). We identified all patients who were seen at Jefferson between August 1997 and May 2000. To be included in this study the patient had to meet the Silberstein et al. (2) criteria for NDPH. (Table 1) All patients were given a full headache history that identified headache location, quality, intensity and duration of pain, associated headache symptoms, triggering and alleviating factors, possible precipitating events, and personal and family history of headaches. Secondary headache disorders were excluded (via laboratory and neuroimaging studies) before a diagnosis of NDPH was made. If the chart was not complete for the desired information then patients were contacted by telephone to retrieve any missing data. Patients with other forms of CDH, including hemicrania continua, transformed migraine and chronic tension-type headache, were excluded from the study.
Proposed criteria for new daily persistent headache

∗Disorders listed in groups 5–11 refer to International Headache Society diagnostic groups.
Results
Forty women and 16 men were identified with NDPH. Age of onset ranged from 12 to 78 years. Peak age of onset was the second and third decade in women and the fifth decade in men. (Fig. 1) Eighty-seven per cent of NDPH patients were Caucasian, 11% were black and 2% were Hispanic. Eighty-two per cent of patients were able to pinpoint the exact day their headache started. Headache onset occurred in relation to an infection or flu-like illness in 30%, extracranial surgery (e.g. hysterectomy) in 12%, and a stressful life event in 12%. Over one-third of patients could not identify any precipitating event. Some patients, for example, were sitting in a store when their headache began, others awoke from sleep one day with a headache and it never went away.

Age of onset in men (□) and women (▪) with new daily persistent headache.
At the time of presentation at Jefferson, NDPH had lasted at least 6 months in all patients, while many had experienced daily headaches for greater than 5 years duration. A prior headache history was found in 38% of patients (episodic migraine 19%, episodic tension-type headache 2%, unspecific headache 17%). No patient had a prior history of chronic daily headache or an increasing frequency of episodic headache just prior to the onset of their NDPH. The duration of the daily headache ranged from 1.5 to 24 h. In 79% of patients the pain was continuous throughout the day with no pain-free time noted. Baseline average pain intensity was moderate (4–6 out of 10 on a visual analogue pain scale) in 61% of patients, while 21% experienced severe pain (≥ 7 out of 10) all of the time. Headache location was bilateral in 64% of patients. Almost 60% of patients had some pain localized to the occipital-nuchal region, while 44% experienced retro-orbital pain and 18% had holocranial pain.
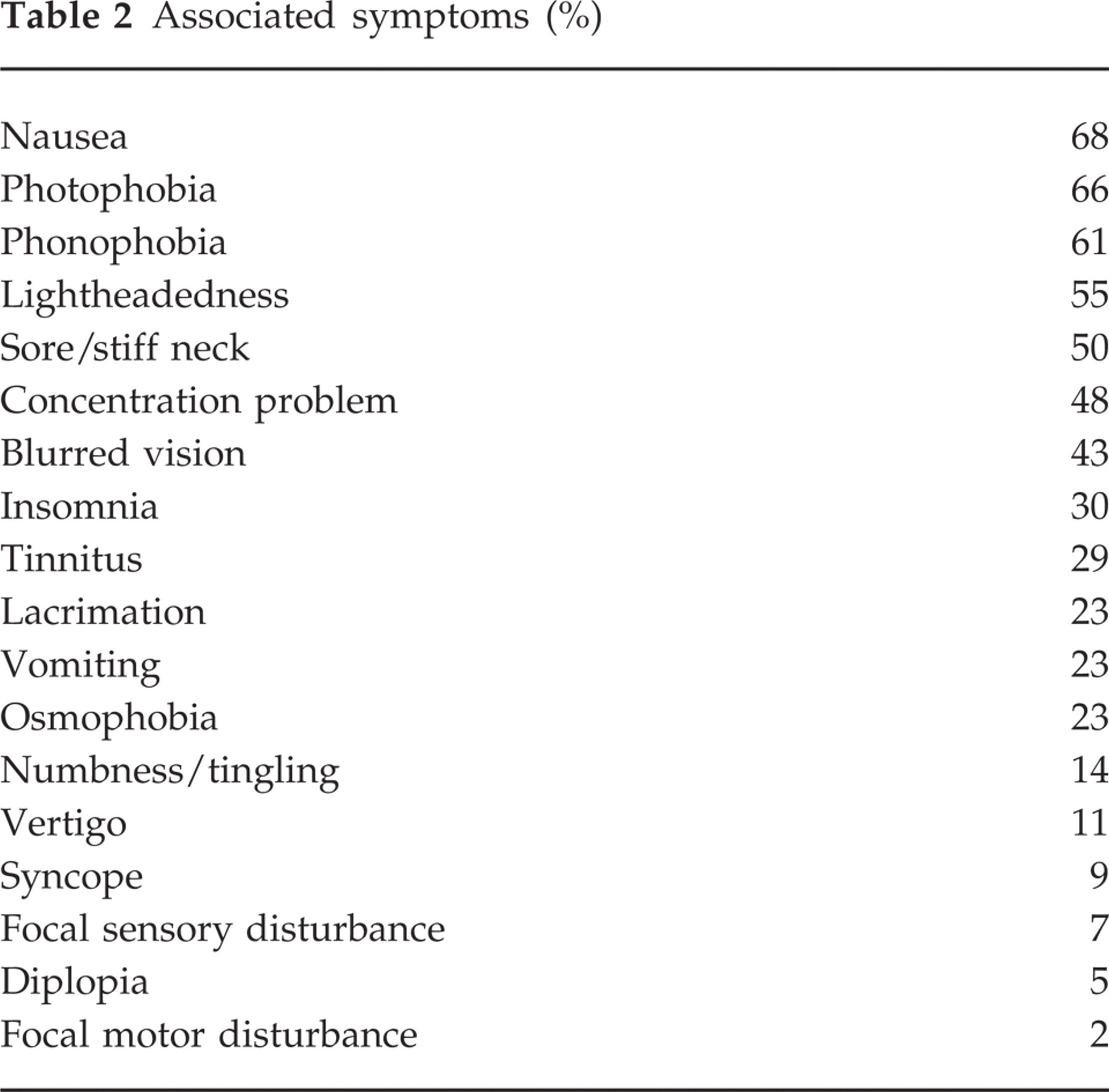
Headache quality was described as a throbbing sensation in 55% and pressure-like in 54%; other descriptions included stabbing (45%), ache (43%), dull (37%), tightness (36%), burning (23%) and searing (4%). Headaches were aggravated by stress in 40%, physical exertion in 32%, and bright light in 29%. Headaches were relieved by lying down (66%), being in a dark room (48%), with massage (23%) and with sleep (9%). With regard to associated symptoms, nausea occurred in 68% of patients, photophobia in 66%, phonophobia in 61%, lightheadedness in 55%, sore/stiff neck in 50%, blurred vision in 43%, vomiting in 23%, osmophobia in 23% and vertigo in 11%. All types of associated symptoms experienced are listed in Table 2. Aura-type symptoms also were present in some patients, including visual photopsias in 9% and seeing zigzag lines in 5%. A family history of headache was documented in 29% of patients, but headache type could not be elicited in most cases because of the patient's poor knowledge of their family member's headache symptoms.
Associated symptoms (%)
Most patients (82%) had a normal neurological examination. In those patients where abnormalities were found, they were typically felt to be non-specific findings (e.g. median neuropathy) and unrelated to the patient's headache condition. Greater occipital nerve trigger point tenderness was identified in 57% of patients and a number of these patients had evidence of cervical facet inflammation on neck extension and rotation manoeuvres.
A brain MRI or CT was completed in 49 patients, of which 66% had normal studies, while the remainder had non-specific imaging findings felt not to be related to the headache condition (e.g. nasal polyps). With regard to laboratory studies, in those patients tested, sedimentation rate (27 patients tested), antinuclear antibodies (22 patients tested) and serum lyme titres (20 patients tested) were normal. Twenty-three patients had a lumbar puncture and this was a normal examination in all tested. There was no evidence of past infection, inflammation or elevated opening pressures. Epstein-Barr virus antibody titres were only tested in seven patients, of whom five had positive titres indicating past but not active infection.
Discussion
NDPH is a newly recognized subtype of CDH that is marked by patients experiencing a daily headache from onset. The literature on this disorder is sparse, with only a handful of publications. NDPH can be a very disabling condition. It has been basically treatment refractory in the clinic and it appears to be able to afflict patients for many years. At the Jefferson Headache Centre several patients presented with a history of NDPH for over 10 years. The goal of the present study is to better define the syndrome of NDPH.
From this investigation NDPH has a female predominance. The female to male gender ratio was 2.5 : 1. Women who develop NDPH do so at an earlier age than men. The peak age of onset of NDPH in women was the second and third decade of life, while the largest incidence of NDPH in men came in the fifth decade. Vanast (1), in his initial description of NDPH, noted a female predominance; of 45 patients diagnosed, 26 were women. In addition, an earlier age of onset of NDPH in women compared with men was also demonstrated; age range of onset in women was 16–35 years, in men 26–45 years.
Over 80% of our patients were able to pinpoint the exact date their headache started. A precipitating event was noted in 54% of the patients. The most common inciter was a cold or flu-like illness. The headache would come along with flu-like symptoms; the non-headache symptoms would resolve but the headache would remain. In addition to infection, NDPH also started post-surgery (12%); all of the surgeries were unrelated to the central nervous system. Finally, a stressful life event triggered NDPH in 12% of patients. Recently, Stewart et al. (3) showed that stressful life events are a risk factor for chronic daily headache in the general population. In the year before or same year of onset of CDH, individuals who developed headache compared with controls more frequently had a change in personal relationships, had moved, had a problem with their children or had an extremely stressful ongoing situation. The study did not define CDH subtypes, so the number of patients who developed NDPH after a stressful life event could not be deemed from this study.
Only 38% of our NDPH patients had a prior history of headache, of which migraine was the most common subtype. None of the patients experienced atypical forms of migraine (hemiplegic migraine, migraine with prolonged aura, basilar migraine).
NDPH was a continuous pain in almost 80% of patients and was of moderate to severe intensity in 82%. The headache could occur anywhere on the head but was typically bilateral, with involvement of the occipital-nuchal region in 60%. Headache quality was throbbing or pressure-like in most patients. The most common associated symptoms were nausea, photophobia, phonophobia, lightheadedness and neck stiffness. These are recognized as typical ‘migrainous’ associated symptoms. Recent literature on cluster patients has shown that symptoms such as photophobia and phonophobia are as common in cluster as migraine, suggesting that these symptoms may be manifestations of activation of the trigeminovascular system, rather than manifestations of a specific headache subtype (4). The presence of these associated ‘migrainous’ symptoms in NDPH suggests a common underlying anatomy for NDPH, migraine and cluster.
The clinical characteristics of NDPH that we found in our patients match the characteristics of the headaches found in Vanast's (1) original description of NDPH. Vanast (1) noted that the pain of NDPH was constant in 72%. Pain location was temporal in nine of 45 patients, temporal plus other areas in 14 patients, occipital and in extra sites in 20 patients, and holocranial in five patients. ‘Migrainous’ associated symptoms were noted in a number of patients: nausea (55%), vomiting (12%), photophobia (34%) and phonophobia (37%). Other associated symptoms included drowsiness and lethargy in 15%, vertigo in 13% and near fainting spells in 1%. Outside of the initial description by Vanast (1) no one else has even attempted to document any of the clinical characteristics of NDPH. In other case reports all that is mentioned is that the patient's met the Silberstein et al. (2) criteria for NDPH, but this criteria does not describe or define headache characteristics.
Laboratory testing in our patients was negative, including neuroimaging studies and spinal fluid analysis. Several patients who initially fitted the description of NDPH were found to have pachymeningeal enhancement on MRI with gadolinium, suggestive of an underlying CSF leak. These patients were treated with intravenous caffeine and or epidural blood patch, with alleviation of their headaches. Vanast (1) also noted that general laboratory studies as well as brain imaging were normal in NDPH patients.
As at least a third of NDPH patients have a cold or flu-like illness when their headache begins, an infectious aetiology for NDPH can be hypothesized. Some authors have linked Epstein-Barr virus infection with NDPH. One study of 32 NDPH patients found 20 who were excreting Epstein-Barr in their oropharynx (5). Almost 85% of the NDPH patients were found to have an active EBV infection, as opposed to eight in a control group. The authors hypothesized that activation of a latent EBV infection may have been the trigger for the development of a chronic daily headache from onset. Epstein-Barr virus titres were only tested in seven of our patients, of whom five had positive titres indicating past but not active infection. As most of our patients had had their headache for years before they were examined in our clinic it is not possible to determine if they did indeed have active EBV infection at the time of headache onset.
NDPH is a newly recognized subtype of chronic daily headache that has not been well characterized in the literature. NDPH appears to be a female-predominant disorder, marked by a continuous daily headache with associated ‘migrainous’ symptoms. Most NDPH patients can state the exact date their headaches began. NDPH needs further studying, as it appears to be one of the most treatment-refractory headache disorders in the clinic.