
Abstract
The objective of this study was to suggest that joint hypermobility (specifically of the cervical spine) is a predisposing factor for the development of new daily persistent headache (NDPH). Twelve individuals (10 female, 2 male) with primary NDPH were evaluated by one of two physical therapists. Each patient was tested for active cervical range of motion and for the presence of excessive intersegmental vertebral motion in the cervical spine. All patients were screened utilizing the Beighton score, which determines degree of systemic hypermobility. Eleven of the 12 NDPH patients were found to have cervical spine joint hypermobility. Ten of the 12 NDPH patients had evidence of widespread joint hypermobility with the Beighton score. Based on our findings we suggest that joint hypermobility, specifically of the cervical spine, may be a predisposing factor for the development of NDPH.
Introduction
New daily persistent headache (NDPH) is a recently recognized form of chronic daily headache (1). It is a unique headache syndrome that typically occurs in patients with no prior headache history and starts daily from onset. A certain percentage of NDPH sufferers will recall an inciting event surrounding the onset of their headache, such as a flu-like illness, stressful life event or a surgical procedure, but over 40% of NDPH patients will state the headache started spontaneously without a recognized trigger (2). NDPH is considered one of the most treatment refractory of all headache syndromes. This reflects our total lack of understanding of the pathogenesis of this disorder. Recently, we have noticed a similar body habitus in our NDPH patients who are tall and thin with a long neck, reminiscent of the physical characteristics seen in individuals with hereditary connective tissue disorders such as Marfan syndrome. On examination these patients also appeared to have lax joints, suggesting underlying joint hypermobility. As joint hypermobility has been recognized as a predisposing factor for the development of chronic pain in the rheumatology literature (3), we decided to look for the presence of joint hypermobility in our NDPH patients. We hypothesized that joint hypermobility, especially of the cervical spine, might be a predisposing factor for the development of NDPH.
Methods
The study population consisted of 12 individuals (10 female, 2 male) with primary NDPH, who were identified at the Michigan Head-Pain and Neurological Institute (MHNI) by the lead author over a 24-month time period. This was a consecutive series of patients who were given a diagnosis of primary NDPH and who were also evaluated by the physical therapists at MHNI. During this time period, two patients with suspected NDPH were not seen by the physical therapists and thus not included in the investigation. On further review they both had a remote history of head trauma, thus they would not have satisfied the criteria for primary NDPH and would have been excluded from the study anyway. Each study patient developed a daily headache from onset, with six patients identifying a triggering event (Table 1). Range of age of onset of NDPH was 8–33 years, with eight patients having their daily headache start before the age of 20 years. All of the patients continue to have persistent daily headache to this day. Range of duration of daily headache is from 2 to 14 years (Table 1). All patients met the new IHS criteria for NDPH prescribed in the second edition of the International Classification of Headache Disorders (1). A diagnosis of primary NDPH was only made after secondary causes of persistent daily headache were ruled out, including cerebral vein thrombosis, mass lesion, spontaneous CSF leak and vessel dissection. Each patient had extensive testing, including brain MRI with and without gadolinium, MRA of the intracranial and extracranial circulation and a MR venogram.
NDPH patient characteristics

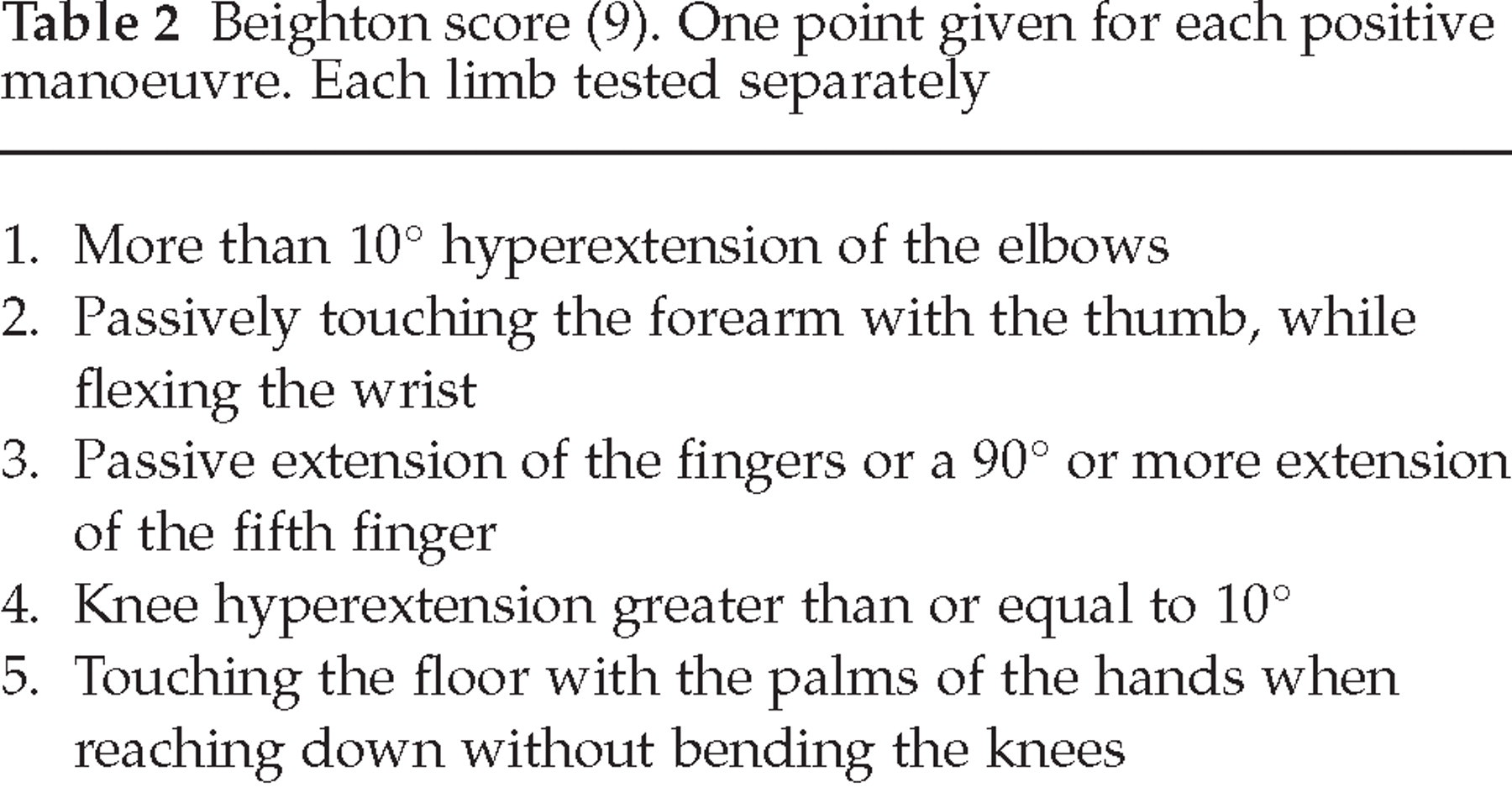
Each study patient was evaluated by one of two physical therapists, both with expertise in assessing headache patients and in osteopathic manual medicine. Each patient was tested in the same manner for active cervical range of motion (ROM) and for the presence of excessive intersegmental vertebral motion in the cervical spine. Active cervical ROM was considered excessive if cervical rotation allowed approximation of the chin to the plane of the shoulder, or if side-bending exceeded 45° (4). Passive intersegmental motion testing was performed in the supine position, using translational passive mobilization manoeuvres (5, 6, 7). Generalized cervical hypermobility was diagnosed if excessive intersegmental range of motion was found throughout the entire cervical spine (6). All of the patients were also screened utilizing the Beighton score, which determines the presence of systemic hypermobility (8) (Table 2). If a patient scored 4 or higher on testing they were deemed to have systemic hypermobility.
Beighton score (9). One point given for each positive manoeuvre. Each limb tested separately
Results
Eleven of the 12 NDPH patients were found to have generalized cervical spine joint hypermobility after evaluation by our physical therapists. Ten of the patients had evidence of widespread joint hypermobility with the Beighton score (Table 2). One of the study patients was diagnosed with Stickler syndrome, an inherited disorder of collagen. Several images (Fig. 1) are shown to document the similar physical appearance of the NDPH patients and some of the hypermobility manoeuvres (all patients provided written consent to allow their images to be used for educational purposes). The long thin neck (‘swan like neck’) was evident in many of the patients.
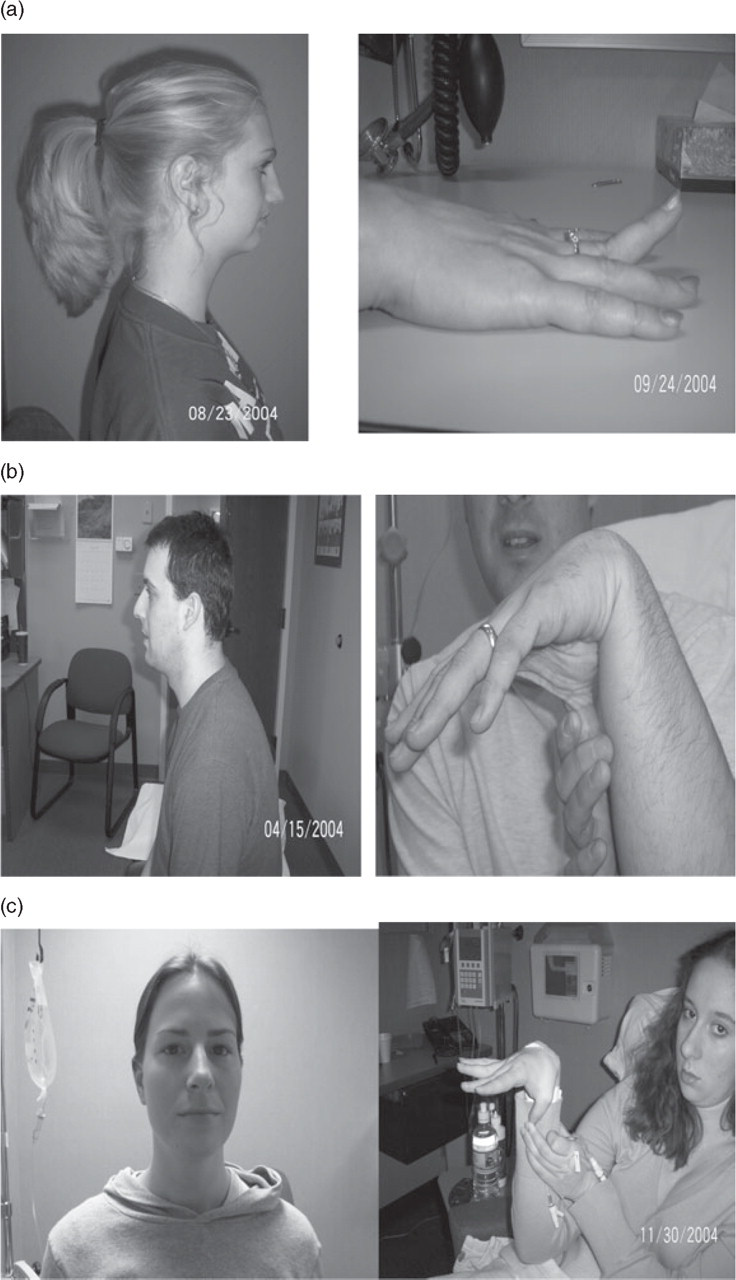
(a–c) Multiple images of NDPH patients and manoeuvres demonstrating joint hypermobility (12).
Discussion
Based on our findings we suggest that joint hypermobility, specifically of the cervical spine, is a predisposing factor for the development of NDPH. Joint hypermobility was found in 92% of our NDPH patients, whereas only 10% of the western population has been noted to have hypermobile joints (9). The majority of our patients were female and adolescent, both of which are known features of NDPH (2, 10). Joint hypermobility is a more common phenomenon in adolescent females than adolescent males (11). Joint hypermobility, however, is not very prevalent in adolescents, with no more than 14% of this population affected, which is far less than that found in our patients (12, 13).
For years joint hypermobility was felt to represent just the outer end of the Gaussian curve and a variant of normal (9). However, more recently there has been evidence to suggest that joint hypermobility may be pathological and can lead to significant morbidity (pain, recurrent joint dislocation) in individuals who have it (11). The rheumatological literature suggests that simple changes in lifestyle, such as initiating a new exercise regime, can be a major triggering factor for the development of morbidity in previously healthy hypermobile individuals (14). This is very reminiscent of what is seen in NDPH, which in many patients appears to occur out of the blue, or with minimal triggering events.
How joint hypermobility in the cervical spine could lead to persistent daily head pain is unknown at present. Evidence exists that there is a convergence of trigeminal and cervical afferents in the trigeminal nucleus caudalis (TNC) (15). Thus, cervical spine pathology can present as head pain typically in a trigeminal nerve V1 distribution (16). Cervical spine joint hypermobility in some manner may influence cervical afferent input into the TNC, with the subsequent development of head pain.
This study was not conceived and designed to validate an association between joint hypermobility and NDPH. It is an initial observation of a possible association. There are limitations to this study. The sample size was small so we cannot state with any certainty that joint hypermobility is found in a large percentage of NDPH patients. Each of our study subjects was examined by only one of the two physical therapists so the reliability of the findings is in question. A double-blinded examination by both physical therapists would have strengthened our results. In addition, the true reliability of manual examination of passive intersegmental motion to determine cervical hypermobility is unknown. Finally, an age and gender matched control group population with non-NDPH chronic daily headache and which demonstrated no evidence of cervical spine hypermobility, would have strengthened our results.
Further investigation is now needed to see if other NDPH patients, diagnosed outside of our institution, show evidence of cervical spine joint hypermobility. In addition, if the majority of NDPH patients have joint hypermobility then do they also have an underlying genetic-based connective tissue disorder? Finally, if cervical spine joint hypermobility is an essential predisposing factor in the development of NDPH, would long-term physical therapy, working on neck strengthening/stabilization, improve pain and headache-related disability in patients with NDPH?