
Abstract
Background:
Teriflunomide is a first-line oral immunomodulatory agent approved in China for the treatment of relapsing multiple sclerosis.
Objective:
To compare the treatment outcomes of teriflunomide and no disease-modifying therapy (DMT) treatment (in first year) in multi-center real-world Chinese multiple sclerosis patients.
Design:
Retrospective study.
Methods:
This study was conducted in five tertiary hospitals in different geographical regions of China. We collected clinical data of patients treated with teriflunomide and no DMT treatment (in first year) between 1 January 2017 and 31 August 2021. The effectiveness of teriflunomide was described. Potential factors influencing the effectiveness of teriflunomide were investigated.
Results:
A total of 372 patients treated with teriflunomide and 148 no DMT treatment patients were included. A total of 292 patients were treated with teriflunomide for at least 6 months, described as a stable teriflunomide cohort. The annualized relapse rate was significantly lower in the stable teriflunomide cohort than in the no DMT treatment cohort (0.23 ± 0.47 versus 0.87 ± 0.67, p < 0.001). The mean Expanded Disability Status Scale (EDSS) score of the stable teriflunomide cohort (1.77 ± 1.62) was slightly different from that of the no DMT treatment cohort (2.09 ± 2.00). A previous annualized relapse rate of ⩾1, a previous EDSS score of ⩾2, and a long disease duration of ⩾5 years were associated with better clinical effectiveness.
Conclusion:
Teriflunomide is associated with a lower relapse rate and less disability accumulation in Chinese patients with multiple sclerosis.
Introduction
Multiple sclerosis (MS) is a chronic autoimmune disease characterized by demyelination and axonal loss in the central nervous system (CNS). 1 There are four main types of MS: clinically isolated syndrome (CIS), primary progressive MS (PPMS), secondary progressive MS (SPMS), and relapsing-remitting MS (RRMS). 2 ‘Relapsing MS’ (RMS) is a term that encompasses all forms involving relapses, and these forms are the most frequently encountered. Many disease-modifying therapies (DMTs) have been approved in various regions of the world for the treatment of RMS.
Teriflunomide is a once-daily oral immunomodulatory agent approved for the treatment of RMS. 3 It reversibly inhibits dihydroorotate dehydrogenase, a key mitochondrial enzyme involved in pyrimidine synthesis for DNA replication. Consequently, the drug reduces T- and B-cell activation, proliferation, and function in response to autoantigens. 4 The efficacy and safety of teriflunomide in RMS have been robustly demonstrated through phase III clinical trials, including the TEMSO, 5 TOWER, 6 and TOPIC 7 trials. Moreover, large-scale observational studies such as Teri-PRO 8 and TAURUS-MS 9 have shown that patients report high treatment satisfaction, convenience, and tolerability with teriflunomide.
As the most widely used DMT in China, teriflunomide has been in the Chinese market for 4 years. Several single-center real-world studies have confirmed the effectiveness and tolerability of teriflunomide in Chinese patients with MS.10,11 However, owing to the limitations of single-center studies, such as poor representation and generalization, multi-center, real-world studies evaluating the effectiveness and safety of teriflunomide in Chinese patients with MS are needed. Moreover, DMT-naïve patients who do not receive any DMT treatment account for a considerable proportion of all MS patients in China. Furthermore, few studies have examined the predictors of treatment response, which are important factors when determining personalized treatment decisions.
Therefore, we conducted a multi-center, real-world retrospective study to evaluate the treatment outcomes of teriflunomide in Chinese patients with MS. We also investigated the factors influencing the effectiveness of teriflunomide treatment.
Materials and methods
Data sources
This multi-center, retrospective, observational study was conducted at five tertiary hospitals and regional MS centers in different geographical areas (east, middle, and west) of China. We collected historical clinical data of patients with MS who visited the neurology department of these hospitals between 1 January 2017 and 31 August 2021. The subjects’ data were extracted from anonymized medical records in a clinical setting during the study period and collected through an electronic case report form.
Study design
The study population included two cohorts of patients with MS. For the whole teriflunomide cohort, patients treated with teriflunomide between 1 January 2017 and 31 August 2021 were selected. Of these, patients who were treated with teriflunomide for at least 6 months during this same time period were selected as the stable teriflunomide cohort. Patients who had not received DMT within 1 year after the initial MS diagnosis (mainly due to the availability, cost of treatment, or the understanding of patients and clinicians about MS disease and DMT treatment) during the study period were selected as the “no DMT treatment” cohort. Patients who participated in other interventional clinical studies during the study period were excluded.
The treatment duration of the whole teriflunomide cohort was described. Among MS patients treated with teriflunomide for at least 6 months, described herein as the stable teriflunomide cohort, the differences in annualized relapse rate (ARR) and Expanded Disability Status Scale (EDSS) scores before and after teriflunomide treatment were calculated. We further compared the differences in ARR and EDSS scores between the stable teriflunomide and no DMT treatment cohorts. We also explored potential factors influencing the effectiveness of teriflunomide using a multinomial logistic regression model.
A safety analysis was conducted on the whole teriflunomide cohort. Adverse events (AEs) occurring during the study period were also recorded. We further investigated the reasons for drug discontinuation among patients who discontinued teriflunomide treatment during the study period using the medical records.
Statistical analysis
First, a descriptive analysis of the patients’ clinical characteristics was performed. Continuous data were summarized as mean [standard deviation (SD)] or median [interquartile range (IQR), 25th percentile–75th percentile) and compared between groups using Student’s t tests or Mann–Whitney U tests. Categorical data were summarized as counts (percentage) and compared between groups using the chi-square test or Fisher’s exact test.
Subsequently, the Mann–Whitney U test was used to assess whether there were significant changes in the ARR and EDSS scores of patients before and after teriflunomide treatment. A comparison of ARR and EDSS scores was also conducted between stable teriflunomide and no DMT treatment cohorts.
Propensity score matching (PSM) using a logistic regression model was conducted to balance covariates between patients receiving teriflunomide treatment for at least 6 months and no DMT treatment patients. Patients in the no DMT treatment arm were matched in a 1:2 ratio to those in the stable teriflunomide treatment arm with a similar predicted probability using the nearest neighbor matching technique with a caliper of 0.20 SDs of the propensity score. Matching factors included age of initial symptom, gender, MS duration, initial symptom, and type of MS. Standardized mean differences (SMDs) were calculated, and SMD >0.2 was considered to be an imbalance.
Potential factors influencing the effectiveness of teriflunomide included gender, age of onset (continuous variable measured in years), ARR before treatment (<1, ⩾1), EDSS before treatment (<2 or ⩾2), MS disease duration (<5 years, ⩾5 years), previous DMT use (defined as the use of any DMTs before teriflunomide treatment), and teriflunomide treatment duration (6–12 months, 12–24 months, ⩾24 months). The effectiveness of teriflunomide was defined by two endpoints: relapse (ARR) and disability evaluation (EDSS). The change in ARR was classified according to three categories: increased or unchanged after treatment, a 0–70% reduction, and a 70–100% reduction. The change in EDSS was also divided into three categories: disability worsening (an increase of ⩾1.0 points in the EDSS score from baseline for patients with baseline EDSS scores <5.5 or ⩾0.5, for patients with baseline EDSS scores ⩾5.5), disability stabilization (EDSS score remained stable or with an increase but did not meet the criteria for disability worsening), and disability improvement (a reduction in EDSS score from baseline). Multinomial logistic regression was performed to evaluate the impact of potential factors on the changes in ARR and EDSS in patients treated with teriflunomide. The ordinal logistic regression model was not applied because it failed the parallel regression assumption.
All analyses were conducted using the R statistical package v.4.1.2 (R Foundation for Statistical Computing, Vienna, Austria).
Results
Clinical characteristics
During the study period, a total of 372 patients treated with teriflunomide and 148 no DMT treatment patients were identified (Table 1). The mean ages of the whole teriflunomide and no DMT treatment cohorts were 31.89 and 39.04 years, respectively. Women accounted for 69% of the whole teriflunomide cohort and 67% of the no DMT treatment cohort. The mean age of onset was 27.74 ± 9.11 years for the whole teriflunomide cohort, and the mean disease duration was 4.90 ± 5.07 years. The whole teriflunomide cohort had a mean ARR before treatment of 1.00 ± 0.73 and a mean EDSS before treatment of 1.92 ± 1.49. The most common initial symptoms were limb numbness (39%), weakness (17%), and blurred vision (15%) among the whole teriflunomide cohort. Corticosteroids (22%) and interferons (15%) were the most commonly used medications in patients treated with teriflunomide.
Clinical characteristics of the whole teriflunomide cohort versus the no DMT treatment cohort.
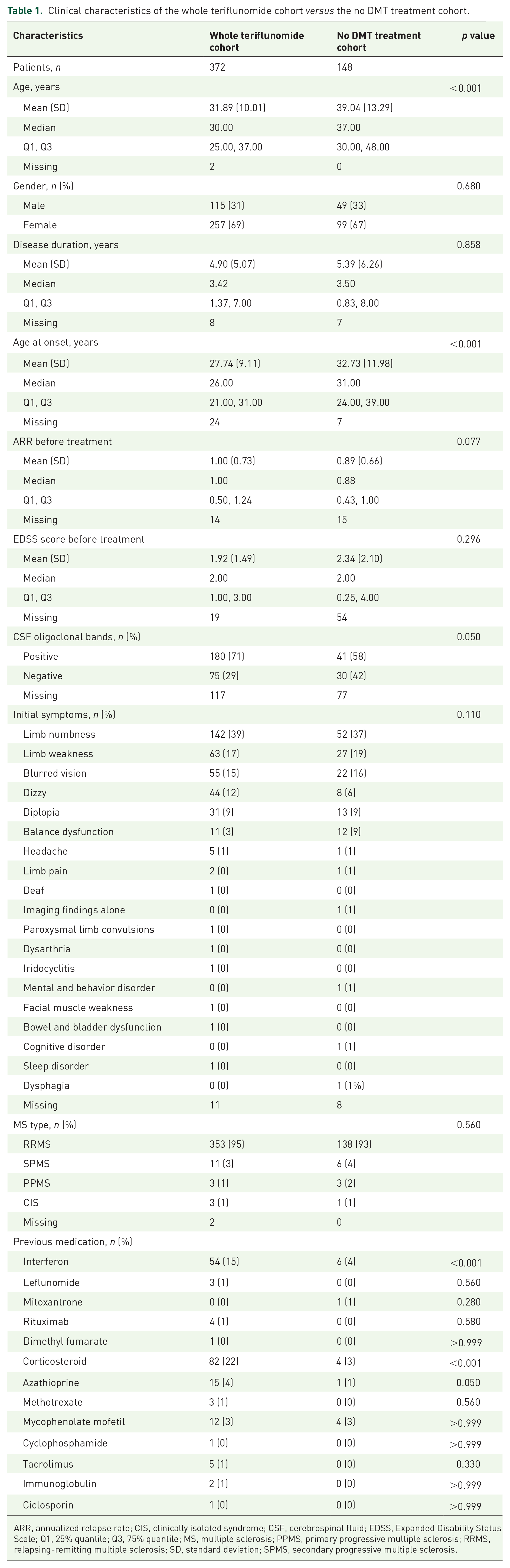
ARR, annualized relapse rate; CIS, clinically isolated syndrome; CSF, cerebrospinal fluid; EDSS, Expanded Disability Status Scale; Q1, 25% quantile; Q3, 75% quantile; MS, multiple sclerosis; PPMS, primary progressive multiple sclerosis; RRMS, relapsing-remitting multiple sclerosis; SD, standard deviation; SPMS, secondary progressive multiple sclerosis.
Teriflunomide treatment duration
The median treatment duration of teriflunomide was 12(6, 18) months (Table 2). In the whole teriflunomide cohort, 292 (78.92%) patients were treated with teriflunomide for at least 6 months.
Treatment duration of the whole teriflunomide cohort.

Q1, 25% quantile; Q3, 75% quantile; SD, standard deviation.
Effectiveness analysis
Among the patients who were treated with teriflunomide for at least 6 months, described as the stable teriflunomide cohort, the ARR was significantly lower (0.22 ± 0.44) at the last follow-up visit compared to pre-treatment (1.01 ± 0.74), with a 78.2% reduction (Table 3). The EDSS score showed a reduction, with a pre-treatment average of 1.92 ± 1.54 and a post-treatment average of 1.79 ± 1.66.
Effectiveness outcomes of the stable teriflunomide cohort (pre-treatment versus post-treatment).

95% CI, 95% confidence interval; ARR, annualized relapse rate; EDSS, Expanded Disability Status Scale; SD, standard deviation.
We then evaluated the ARR and EDSS in the stable teriflunomide cohort versus the no DMT treatment cohort. After adjustment for the clinical characteristics by PSM analysis, the clinical characteristics of the no DMT treatment and stable teriflunomide cohorts were found to be comparable (Table 4). There were no significant differences in age of onset, gender, disease duration, initial symptoms, and MS type between the no DMT treatment cohort and the stable teriflunomide cohort.
Clinical characteristics of the no DMT treatment and stable teriflunomide cohorts via propensity score matching analysis.

CIS, clinically isolated syndrome; MS, multiple sclerosis; PPMS, primary progressive multiple sclerosis; PSM, propensity score matching; RRMS, relapsing-remitting multiple sclerosis; SD, standard deviation; SMD, standardized mean difference; SPMS, secondary progressive multiple sclerosis.
The ARR of the stable teriflunomide cohort (0.23 ± 0.47) was significantly lower than that of the no DMT treatment cohort (0.87 ± 0.67; Table 5). The average EDSS score of the stable teriflunomide cohort (1.77 ± 1.62) was also lower than that of the no DMT treatment cohort (2.09 ± 2.00).
Effectiveness outcomes of the no DMT treatment cohort versus the stable teriflunomide cohort.

95% CI, 95% confidence interval; ARR, annualized relapse rate; EDSS, Expanded Disability Status Scale; SD, standard deviation.
Factors influencing the effectiveness of teriflunomide
In the relapse evaluation (Table 6), after adjusting for the other characteristics, patients with an ARR before treatment of ⩾1 were more likely to have a 0–70% reduction (odds ratio [OR] = 6.71; 95% confidence interval [CI] = 1.92–23.5, p = 0.003) and >70% ARR reduction (OR = 2.73; 95% CI = 1.15–6.44, p = 0.022) than patients with an ARR before treatment of <1. Patients with a disease duration of ⩾5 years were more likely to have a 0–70% ARR reduction (OR = 3.95; 95% CI = 1.08–14.4, p = 0.038) than patients with a disease duration of <5 years. In addition, patients with a teriflunomide treatment duration of >24 months were more likely to have a 0–70% ARR reduction (OR = 13.6; 95% CI = 2.47–75.2, p = 0.003) than patients with a teriflunomide treatment duration of 6–12 months.
Multinomial logistic regression analysis of factors influencing teriflunomide effectiveness (ARR).

95% CI, 95% confidence interval; ARR, annualized relapse rate; DMT, disease-modifying therapy; EDSS, Expanded Disability Status Scale; OR, odds ratio.
Bold values denote statistical significance at the p < 0.05 level.
In the disability evaluation model (Table 7), patients with before treatment EDSS score of ⩾2 were more likely to have disability improvement (OR = 3.32; 95% CI = 1.49–7.40, p = 0.003) than those with before treatment EDSS score of <2, and patients with previous DMT use were less likely to have disability improvement (OR = 0.22; 95% CI = 0.07–0.67, p = 0.008).
Multinomial logistic regression analysis of factors influencing teriflunomide effectiveness (EDSS).

95% CI, 95% confidence interval; ARR, annualized relapse rate; DMT, disease-modifying therapy; EDSS, Expanded Disability Status Scale; OR, odds ratio.
Bold values denote statistical significance at the p < 0.05 level.
Safety analysis
A total of 219 AEs were reported among the whole teriflunomide cohort (Table 8). The most common adverse effect of teriflunomide was alopecia, which was described in 28.49% of the whole teriflunomide cohort. Other common adverse effects included abnormal liver function test results (7.80%), leukopenia (5.91%), and skin rash (2.96%). Other adverse reactions, such as digestive symptoms, headache, amenorrhea, weight loss, and hypertension, occurred in less than 2% of the whole teriflunomide cohort.
The adverse effects of whole teriflunomide cohort.

Analysis of treatment discontinuation
During the study period, a total number of 136 patients in the whole teriflunomide cohort discontinued the treatment (Table 9). Disease relapse was the main reason for treatment discontinuation (55.15%). Other reasons included financial reasons (8.82%), self-intention (6.62%), pregnancy or an intention to get pregnant (5.88%), adverse drug reaction (5.88%), and going off-test (5.15%). Among those who discontinued treatment, 26 patients (19.12%) had a treatment duration of <3 months, and 13 patients (9.56%) were treated with teriflunomide for >25 months.
Analysis of teriflunomide treatment discontinuation.

Subgroup analysis
We further evaluated the effectiveness of teriflunomide in different MS types in the stable teriflunomide cohorts (Table 10). In RRMS patients, the ARR post-treatment was significantly lower (0.21 ± 0.44) than the ARR pre-treatment (1.01 ± 0.75). The EDSS scores also showed a decreasing trend. The same decreasing ARR trend was also observed in other types of patients, while the change in EDSS scores showed an unstable trend.
Effectiveness outcomes of different MS types (pre-treatment versus post-treatment).
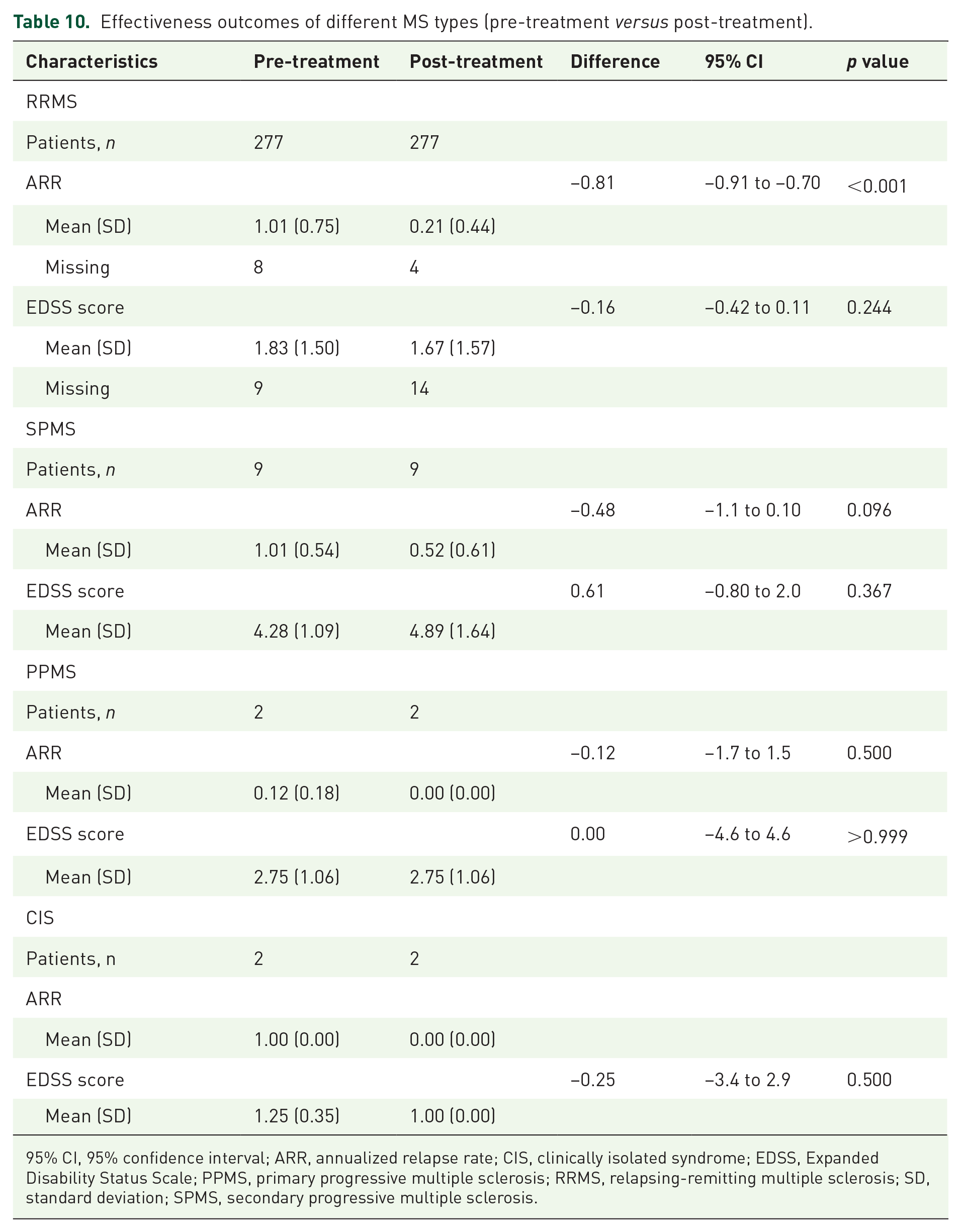
95% CI, 95% confidence interval; ARR, annualized relapse rate; CIS, clinically isolated syndrome; EDSS, Expanded Disability Status Scale; PPMS, primary progressive multiple sclerosis; RRMS, relapsing-remitting multiple sclerosis; SD, standard deviation; SPMS, secondary progressive multiple sclerosis.
Discussion
Here, we present a retrospective multi-center real-world study on MS patients following teriflunomide treatment from five tertiary hospitals and regional MS centers in different geographical areas of China. To the best of our knowledge, this study is the first to evaluate real-world treatment outcomes of teriflunomide in Chinese patients with MS in multiple regions. The regional MS centers included in this study were located in eastern, central, and western China. Therefore, the patients included in this study were representative of a broad MS population in China.
Some large-scale studies focusing on the prevalence and clinical features of MS in Asian or Chinese population have been reported.12,13 It is recognized that MS in Asia is associated with different clinical and epidemiological features compared with those in North America and Europe, such as a lower prevalence, rare familial occurrence, high female to male ratio, more severe optic nerve and spinal cord attacks, fewer brain and cerebellar lesions, lower proportion of progressive disease, and a lower incidence of positive oligoclonal bands. 14 In this study, females accounted for a high ratio of participants in both the teriflunomide and no DMT treatment cohorts. RRMS accounted for 95% and 93% of the teriflunomide and no DMT treatment cohorts, respectively. Optic nerve and spinal cord symptoms, such as limb numbness, limb weakness, and blurred vision, were the most common initial symptoms, consistent with the previous findings [with limbs numbness (33%), blurred vision (16%), limbs weakness (14%), and diplopia (7%)]. 12
Previous phase III trials, such as TOWER 6 and TEMSO, 5 demonstrated that teriflunomide was associated with a lower relapse rate and less disability accumulation than placebo. A subgroup analysis of the TOWER study also confirmed that teriflunomide was as effective and safe in the Chinese subpopulation as it was in the overall population of patients in the TOWER trial. 15 Teriflunomide entered the Chinese market in 2018; thus far, real-world data on the effectiveness of teriflunomide in Chinese patients have been relatively limited. In our study, we observed a decreasing trend in EDSS scores and ARR using multi-center real-world data from MS patients in different areas of China. Compared with the ARR pre-treatment, ARR post-treatment decreased from 1.01 to 0.22, a 78.22% reduction. The ARR of the teriflunomide cohort was much lower than that of the no DMT treatment cohort after PSM (0.23 versus 0.87). These results were similar to those of our previous single-center real-world study. 10 The decreasing trend of relapse rate observed in our study was similar to that of the TOWER Chinese subpopulation 15 and much higher than that of European and American Caucasian populations. 4 According to previous studies, the difference in the effectiveness of teriflunomide between the Chinese population and European and American Caucasian populations may be due to differences in plasma teriflunomide concentrations. Population pharmacokinetic analysis showed that the median value for the area under the plasma teriflunomide concentration versus time curve (0–24 h) in Chinese patients was 51.5% higher than that in non-Asian patients. Furthermore, according to previous studies and our data, few Chinese patients had received other DMTs compared with the European and American Caucasian populations. Therefore, we suggest that teriflunomide is more suitable for Chinese patients. We noticed that the age of the stable teriflunomide cohort before PSM was younger than that of the stable teriflunomide cohort after PSM and the ARR post-treatment was slightly higher in the group after PSM (0.23 ± 0.47) compared with the group before PSM (0.22 ± 0.44), which suggested that age may affect the DMT treatment response of MS. Since patients who did not receive DMTs still accounted for a considerable proportion of all patients with MS in China, it is recommended that patients who do not receive DMTs at present should start DMTs as soon as possible.
The previous single-center real-world study had provided guidance regarding that female treatment-naïve patients with mild disease activity (⩽1 attack in 1 year or ⩽2 attacks in 2 year before treatment) and EDSS score <4 at treatment initiation were more likely to benefit from teriflunomide. 11 Considering that the ARR and before treatment EDSS scores varied among patients treated with teriflunomide, we included both variables as confounders in the models. Finally, our study identified that a previous ARR of ⩾1, longer disease duration (⩾5 years), and longer teriflunomide treatment duration (⩾24 months) were associated with high ARR reduction. A previous EDSS score of ⩾2 and a history of no previous DMT use were associated with disability improvement. Although post-marketing studies have shown a propensity to prescribe teriflunomide to men rather than women, driven by safety concerns about pregnancy 16 and risk of hair thinning and alopecia, and the previous single-center real-world study has shown that female patients were more likely to benefit from teriflunomide treatment, 11 in this study gender was not a significant factor influencing the effectiveness of teriflunomide. The age of onset also showed no significant impact on the effectiveness of teriflunomide in both relapse reduction and disability improvement. Patients with more than 5 years of disease duration showed a significant association with ARR reduction, which is consistent with the findings of a previous study. 17 We suggested this may be due to the high proportion of MS patients who have not undergone prior DMT treatment. Despite their long disease duration, patients with a naïve DMT treatment history may still benefit from the initial DMT treatment. We also noticed that a teriflunomide treatment of >24 months had a significant impact on ARR reduction, indicating that the persistence of teriflunomide treatment is important. A decreasing effect on the probability of disability improvement was observed in patients who had undergone previous treatment with DMTs. Therefore, this analysis suggested MS patients with a previous ARR of ⩾1, a previous EDSS score of ⩾2, and a long disease duration of ⩾5 years can also benefit from teriflunomide treatment, who had not been considered as the major target population before. Nevertheless, more evidence is required to support this finding.
In this study, the most common adverse effects were alopecia (28.49%), abnormal liver function test results (7.80%), leukopenia (5.91%), and skin rash (5.91%), which were consistent with the safety results from the TOWER Chinese subgroup. 15 Most adverse events were mild, suggesting that teriflunomide was generally well tolerated in Chinese patients.
Our study has some limitations. First, the sites in this study did not include MS centers in northern China, and limited numbers of regional MS centers may lead to incomplete assessment and bias; more large-scale, multi-center, multi-regional real-world studies are needed to increase the representativeness of the sample in the future. Second, due to the retrospective design and inconsistent medical imaging standards, this study did not include any magnetic resonance imaging (MRI) endpoints. Third, the duration of follow-up should be extended to observe the long-term effectiveness and safety of teriflunomide. Furthermore, future large-scale research is needed to determine the factors influencing the effectiveness of teriflunomide.
Taken together, these results suggest that teriflunomide is associated with a significantly lower relapse rate and less disability accumulation, which is consistent with previous clinical trials. We noticed MS patients with a previous ARR of ⩾1, a previous EDSS score of ⩾2, and a long disease duration of ⩾5 years might also benefit from teriflunomide treatment. In addition, teriflunomide was well tolerated in this study.