
Abstract
Background:
Neuromyelitis optica spectrum disorder (NMOSD) is a devastating autoimmune disorder with cycles of escalating relapse. Rates of diagnosis in the elderly are increasing. Therapeutic decision-making is more challenging in elderly patients due to multiple comorbidities and high risk of drug-induced side effects.
Objective:
This retrospective study assessed the efficacy and safety of standard plasma exchange (PLEX) treatment in an elderly population with NMOSD.
Design:
Seventy-six patients with NMOSD who received PLEX were apportioned to two groups as either elderly (⩾60 years, n = 26) or young (<60 years) at the time of the first procedure.
Methods:
Therapeutic response was judged according to functional recovery at 6 months, as reflected by Expanded Disability Status Scale (EDSS) and visual outcome scale (VOS) scores.
Results:
The mean age of the 26 elderly patients was 67.7 ± 7.9 years (range 60–87 years); the population was predominantly female (88.5%). PLEX sessions were generally well tolerated among the elderly. Compared with the young patients, the elderly had significantly more comorbidities and concomitant medications. Twenty-four (96.0%) elderly patients showed functional improvement at 6 months after PLEX, of which 15 (60.0%) experienced moderate-to-marked improvement. Six months after the initial PLEX treatment, the patients overall experienced a significant improvement in EDSS and VOS scores. Logistic regression showed that severe optic neuritis attack was a significant independent prognostic factor associated with poor PLEX response. The groups were comparable regarding overall or serious adverse events. The rate of transient hypotension was significantly higher in the elderly compared with the young.
Conclusion:
PLEX is an effective and safe therapy for elderly patients with NMOSD and should be considered a treatment option during NMOSD attacks. In the elderly, preventive measures against hypotension are recommended before PLEX.
Introduction
Neuromyelitis optica spectrum disorder (NMOSD) is a rare B-cell autoimmune disorder of the central nervous system, mainly characterized by area postrema syndrome, severe optic neuritis, and longitudinally extensive transverse myelitis (LETM). NMOSD may be confused with multiple sclerosis. A chronic cycle of recovery and relapse is typical. In NMOSD, the body produces a defined autoantibody that attacks aquaporin 4 (AQP4), a protein on the surface of astrocytes that is vital to the central nervous system.1,2
NMOSD is most common in young adult women, aged 30 to 50 years. 3 However, with development of the AQP4-immunoglobulin G (IgG) test, the prevalence of elderly-onset NMOSD has been recognized as increasing worldwide.4–6 Elderly patients are beset by the same relapse frequency as the young, but attacks are more severe.6–8 Regardless of age, aggressive treatment of attacks should be initiated as early as possible.
Plasmapheresis, also known as plasma exchange (PLEX), is a well-established modality to treat various neuroimmunological disorders. PLEX involves replacing the patient’s plasma with a colloid fluid, thereby removing pathognomonic inflammatory mediators such as AQP4-IgG, other antibodies, and pro-inflammatory cytokines. 9 Patients with NMOSD have benefited from PLEX, as first-line or rescue therapy during attacks.10–13
Patients of any age are eligible for PLEX therapy. However, choosing among options for the elderly is complicated by multiple comorbidities, concomitant medications, vulnerable hemodynamic systems, and declined immune function. The invasiveness and operational methods of PLEX especially put the elderly at greater risk of adverse events.14–16 Furthermore, there is limited data on the indications and outcomes of PLEX for elderly patients with NMOSD.
This retrospective study assessed the efficacy and safety of PLEX used to treat consecutive Chinese elderly patients with NMOSD in a tertiary hospital.
Methods
The Institutional Review Board of China–Japan Friendship Hospital approved this retrospective study (Approval No. 2016-26-3). The patients, or their guardians when the patient had motor dysfunction or suffered unconsciousness, provided written informed consent before PLEX initiation.
Patients and inclusion criteria
The medical records were reviewed of 76 consecutive Chinese patients suffering from clinically and/or radiologically confirmed NMOSD, who had been hospitalized at China–Japan Friendship Hospital (Beijing, China) between October 2010 and July 2022. All the patients fulfilled the following criteria: with NMOSD (with or without AQP4-IgG);17,18 in the acute phase of the disease; received at least one session of PLEX treatment; and underwent evaluation at least 6 months after the last PLEX administration. Any prospective subject with a history of serious infection or other underlying acute medical condition (such as new bleeding, serious circulatory failure, or malignant arrhythmias) was excluded.
For analysis, the patients were divided into two groups by age (at the time of the PLEX procedure) as young or elderly (<60 years and ⩾60 years, respectively). The definition of elderly (aged ⩾ 60 years) referenced the ‘Law of the People’s Republic of China on the Protection of the Rights and Interests of Elderly People’ amended 29 December 2018.
PLEX procedure
The criteria for PLEX candidacy were contraindications to intravenous methylprednisolone (IVMP) and intravenous immunoglobin (IVIg), or a limited response to an initial standard dose of either of these. In addition, a patient was considered a candidate for PLEX if experiencing a severe disabling attack, as observed by at least two physicians on admission. A severe disabling attack was defined as, in nadir, an Expanded Disability Status Scale (EDSS) score ⩾ 6, or a visual outcome scale (VOS) score ⩾ 5.
All candidates received one session of PLEX every other day in the Neurology ward, for up to seven sessions, depending on therapeutic efficacy and tolerance. One-to-1.5 volumes of plasma were exchanged at each session. The exchanged plasma volume was calculated based on patient gender, body mass, and hematocrit level. 19 Fresh frozen plasma and 5% human albumin solution were used as replacement fluid. Promethazine (25 mg, intramuscular injection) was given as an anti-allergen before each session. Heparin was the first choice of anticoagulant, and dosage was based on body weight (per 100 IU/kg). When heparin was contraindicated, regional citrate was used. Patients were maintained on long-term immunosuppressive therapies during or after PLEX, as appropriate.
Clinical evaluations
The clinical data were retrospectively retrieved from the hospital electronic medical system. The EDSS and VOS scores were evaluated in parallel according to the attack type. The EDSS score was adjudged during attacks that included myelitis or symptomatic brain involvement. Visual acuity was graded 1 to 7 for each eye respectively according to the following VOS scores: 0—20/20; 1—scotoma, but better than 20/30; 2—20/30–20/59; 3—20/60–20/199; 4—20/200–20/800; 5—able to count fingers only; 6—light perception; and 7—no light perception.
Neurological functions of the elderly group were evaluated relative to that of the younger group and the total population at the following timepoints: baseline (before attack), attack (in nadir), after IVMP/IVIg (pre-PLEX), and at 1- and 6-months after the last session of PLEX (short- and long-term outcomes, respectively). The baseline neurological functional scores (EDSS or VOS score) were calculated based on the self-reports of each patient. The primary outcome was the percentages of patients in the elderly and young groups whose neurological functions had returned to baseline by the 6-month follow-up, according to the EDSS and VOS scores.
Secondarily, the factors associated with therapeutic response to PLEX in the elderly group were identified, where response was defined in terms of neurological symptoms and functional improvement; the latter suggested by lowered EDSS or VOS score. A PLEX responder showed marked-to-moderate improvement (MMI), that is, a complete-to-moderate resolution of attack symptoms and a reduction in EDSS or VOS scores by at least 30%, respectively. Patients who did not respond to treatment showed mild-to-no improvement (MNI) in neurological symptoms, and a reduction of less than 30% in EDSS or VOS scores. Logistic regression analyses were used to determine factors that were associated with MMI.
Magnetic resonance imaging evaluations
Evaluations of the spinal cord involvement in these patients were based on magnetic resonance imaging (MRI) scans, because the brain and optic nerve imaging data were incomplete. The spinal cord MRI scans were performed during the acute phase of the disease using a nuclear magnetic resonance scanner (SignaHDX-3.0 T, General Electric, Fairfield, CT, USA; or GYROSCAN-1.5 T, Philips, Amsterdam, Holland). The MRI scanning data were obtained before PLEX, and included the cervical, thoracic, and lumbar spine. All images were sagittal. The radiographical features of interest were the LETM (⩾3 vertebral segments), and the involved spinal cord segments and their location. The area postrema lesion on the cervical MRI was counted as one spinal cord segment when the cervical lesion extended to the area postrema.
Safety evaluations
A bedside nurse remained with the patient throughout the procedure and monitored the safety of PLEX. The following blood analyses after PLEX were repeatedly performed: blood cell count, coagulation function, electrolyte level, cardiac function, and albumin/globulin concentration. Other safety data included vital signs, gastrointestinal reaction, allergic reaction, bleeding, and catheter-related events were recorded as previously described. 12 Serious adverse events were those that prolonged hospitalization or threatened life, by which the PLEX treatments were prematurely interrupted.
Statistical analysis
All statistical analyses were conducted using SPSS 22.0 software (IBM, Armonk, NY, USA). Statistical significance was set at p < 0.05. The continuous variables were analyzed by Mann–Whitney U tests. Differences in the gender ratio and other clinical and imaging parameters between the groups were analyzed using Fisher’s exact tests. Baseline variables that showed a univariate association (p < 0.1) were included in the multivariate logistic regression analysis to determine whether these predictors were independently associated with the clinical outcome. To reduce bias, three patients (one elderly and two young) who received fewer than three sessions of PLEX were excluded from the therapeutic response analyses. Considering that three patients prematurely and completely withdrew (i.e. fewer than three sessions) from the PLEX sessions due to severe adverse events, all the selected subjects underwent a safety evaluation.
Results
Clinical and imaging characteristics of the two groups
The elderly group comprised 26 patients, who were predominantly women (88.5%; Table 1). The mean age at PLEX was 67.7 ± 7.9 years (range 60–87 years). Specifically, at the time of receiving PLEX, there were 18/26 (69.2%), 5/26 (19.2%), and 3/26 (11.5%) patients who were aged, respectively, 60 to 69, 70 to 79, and older than 80 years.
Demographic and clinical features of 26 elderly patients with NMOSD.

BON, bilateral optic neuritis; CID, chronic infectious disease; CLD, chronic lung disease; CS, symptomatic cerebral syndrome; CVO, circumventricular organ; DM, diabetes mellitus; HTN, hypertension; ID, patient identification; LON, left optic neuritis; RON, right optic neuritis.
Age at PLEX, y/gender.
Pre-PLEX.
PLEX sessions.
Withdrew from PLEX prematurely due to heparin-related thrombocytopenia, deep venous thrombosis, and sepsis associated with chemotherapy, respectively.
For example, coronary heart disease, ischemic stroke and symptomatic cerebrovascular stenosis that require long-term secondary prevention medication.
The number of patients with comorbidities in the elderly group [18/26 (69.2%)] was significantly higher than that of the young group [6/50 (12.0%); Table 2], p < 0.05. Specifically, 9/26 (34.6%) and 7/26 (26.9%) patients in the elderly group suffered from, respectively, hypertension or atherosclerotic cardiovascular disease (ASCVD), while neither of these were observed in the young group. In addition, significantly more patients in the elderly group were found with diabetes mellitus (DM) compared with the young [5/26 (19.2%) cf. 2/50 (4.0%), p < 0.05]. Prior to PLEX, none of the patients in the elderly group had experienced cardiac failure or renal dysfunction.
Clinical characteristics and response rate of patients with NMOSD at two age groups. a

AP, area postrema; AQP4-IgG, aquaporin 4 antibodies; ASCVD, atherosclerotic cardiovascular diseases; CVO, circumventricular organ; DM, diabetes mellitus; EDSS, Expanded Disability Status Scale; HT, Hashimoto thyroiditis; IQR, interquartile range; IST, immunosuppressive therapies; LETM, longitudinally extensive transverse myelitis; NMOSD, neuromyelitis optica spectrum disorders; ON, optic neuritis; PLEX, plasma exchange; RA, rheumatoid arthritis; SS, Sjogren’s syndrome; TM, transverse myelitis; VOS, visual outcome scale.
Reported as n (%), unless indicated otherwise;
ASCVD including coronary heart disease, ischemic stroke and symptomatic cerebrovascular stenosis that require long-term secondary prevention medications;
Only patients with spinal cord attack were involved in these analyses.
Seventeen of 26 (65.4%) patients in the elderly group concomitantly used drugs other than immunosuppressive therapy (IST; mainly antithrombotic therapies, antihypertensives, and antidiabetic agents), which was significantly higher than that of the young group (5/50 [10.0%]), p < 0.05. One woman in the elderly group suffered from breast cancer and underwent chemotherapies during the period of the PLEX procedures.
Imaging revealed significantly fewer cervical spinal lesions in the elderly patients [1/21 (4.8%)] compared with the young [10/38 (26.3%)], p < 0.05.
The elderly and young groups were comparable regarding the following: sex ratio; onset symptoms; serum AQP4-IgG; coexisting autoimmunity; prior disease duration; disability at PLEX; presence of LETM; and IST.
Therapeutic efficacy of PLEX
One woman was prematurely withdrawn from the study due to severe sepsis. She received only one session of PLEX and was excluded from the therapeutic response analyses.
Functional improvement was defined as any reduction in EDSS or VOS score. One month after the last session of PLEX, in the elderly group 22/25 (88.0%) patients showed functional improvement, which increased to 24/25 (96.0%) patients at the 6-month follow-up. One 67-year-old male patient with optic neuritis-relapse was unresponsive to PLEX.
In the elderly cohort, 21 patients received IVMP as a first therapy (nine of these were also given IVIg). None of them exhibited significant improvements in either of the scores for function (EDSS or VOS) before PLEX (Figure 1). In patients who received IVMP/IVIg as the first treatment, the percent reduction in EDSS score after PLEX was significantly higher than after IVMP/IVIg therapies at 1 and 6 months (25.2% cf. 2.4% and 48.3% cf. 2.4%, respectively, p < 0.001). The percent reduction in VOS score after PLEX (30.1%) was significantly higher than after IVMP/IVIg (6.3%) therapies at 6 months, but the VOS scores were similar at 1 month (20.0% cf. 6.3%, p = 0.08).
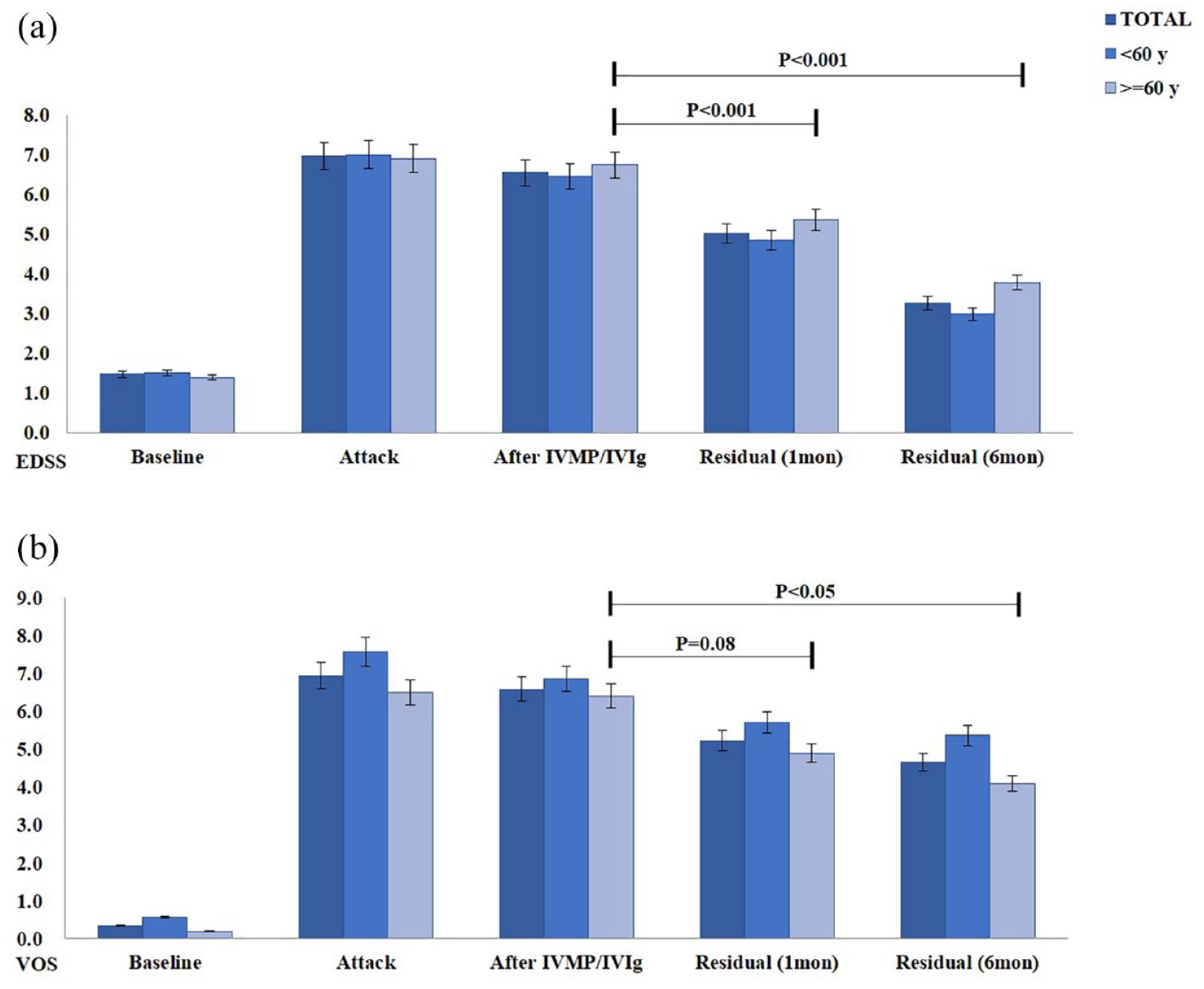
EDSS and VOS scores at various timepoints in patients given IVMP/IVIg as a first therapy (elderly, n = 21). Bar charts showing the (a) EDSS and (b) VOS scores at baseline, attack, after IVMP/IVIg, residual at 1 month and 6 months after the last session of PLEX.
Prognostic factors for PLEX
In the elderly group 6 months after PLEX, 15/25 (60.0%) patients showed overall MMI. Seven of these patients experienced only one attack with transverse myelitis before PLEX and showed MMI. The frequency of attack symptoms and MMI rate after PLEX by each attack type between elderly patients and the total population were similar (Figure 2). In the 7, 21, and 2 elderly patients who experienced attacks with optic neuritis, transverse myelitis, and symptomatic cerebral syndrome, respectively, 2 (28.6%), 14 (66.7%), and 2 (100%) showed MMI at 6 months after PLEX.

Bar chart respectively showing the number and percentage of MMI to PLEX by attack types in the elderly (left) and total population (right).
According to the univariate analyses, the following were not significantly associated with improvement after PLEX: sex; age at onset; age at PLEX; clinical course; pre-PLEX EDSS score; comorbidity; and pre-IST therapies. However, the univariate analyses showed that the following were significant intermediate predictors for MMI (p < 0.1): lower baseline/pre-PLEX VOS score; seropositive AQP4-IgG; short-delayed time from last attack to PLEX; and nonoptic neuritis attacks (Supplementary Table and Figure 2). These were entered into the multivariable logistic regression analysis. In the elderly group, five of six (83.3%) patients who experienced severe optic neuritis attack showed MNI at 6 months after PLEX [p < 0.05, odds ratio: 11.667, 95% confidence interval (CI): 1.112–122.381]. It was shown that severe optic neuritis was a significant prognostic factor independently associated with poor response to PLEX.
In spinal attacks, the lesion locations and median number of involved spinal segments did not differ between patients with MMI and MNI.
Adverse events
Overall, most of the patients tolerated the PLEX sessions (Table 3). The incidence number and percentage of total and specifically serious adverse events of the two age groups were similar. In the elderly group, nine of the 26 (34.6%) patients experienced 12 adverse events. Eight (72.7%) of these adverse events were minor and transient and spontaneously resolved or could be relieved by withholding the PLEX procedure for several days. In the elderly group, 5/26 (19.2%) patients suffered transient hypotension at the first session of PLEX, which was a significantly higher rate than that of the young group [2/50 (4.0%)], p < 0.05.
Adverse events in patients with NMOSD treated by PLEX, n (%).

AE, adverse event; SAE, serious adverse event.
Three patients in the elderly group experienced serious adverse events. One 60-year-old woman who concomitantly underwent chemotherapies developed severe sepsis during the PLEX procedure, and withdrew from the treatment. In addition, in two elderly patients PLEX sessions were prematurely interrupted due to life-threatening heparin-related thrombocytopenia and deep venous thrombosis. None of the elderly patients in our cohort died during the PLEX procedure. The incidence of adverse events was similar among the stratified age groups of the elderly.
Discussion
To our best knowledge, this is the first study to assess the value of PLEX for the treatment of NMOSD in an elderly population. The therapeutic response of 26 elderly patients (>60 years, range 60–87 years) was evaluated relative to that of a younger group of 50 patients in terms of functional recovery from baseline 6 months after PLEX treatment. It was found that the response rates after PLEX of the two groups were statistically similar. The groups were comparable regarding adverse events, but the rate of transient hypotension was significantly higher in the elderly. For the elderly group, logistic regression analyses identified severe optic neuritis as a significant prognostic factor independently associated with MNI (failure of treatment) after PLEX.
In this study, functional improvement occurred in 88.0% of the elderly patients by 1 month after PLEX, and increased to 96.0% after 6 months. This is consistent with another study on NMOSD 20 and supports the long-term benefit of PLEX treatment. In addition, in this study, after failing to respond to initial IVMP/IVIg, lower EDSS and VOS scores showed that the elderly experienced improvement of neurological functions by 6 months after PLEX regardless of attack type (optic neuritis, transverse myelitis, or symptomatic cerebral syndrome).
More than half of the patients showed MMI at 6 months. This is consistent with other studies that concluded that PLEX is an effective therapy for NMOSD attacks, with an overall response rate between 35% and 65% in both Western and Asian populations.10–13,20–22 However, the MMI rate of the elderly patients in the present study (57.7%) was slightly higher than we previously reported for a Chinese overall population with NMOSD (31.0%). 11 This may be because the follow-up of the previous study was only 1 month. 12
In this study, PLEX was the first treatment option applied for five elderly patients who suffered from severe transverse myelitis relapses. After IVMP/IVIg-free PLEX, all these patients achieved clinical MMI. This is in accord with other studies in overall populations.10,12,23 Therefore, PLEX may be considered a first choice for elderly patients, especially in cases of severe NMOSD relapse with or without disabling transverse myelitis.
In contrast to two recent studies in overall populations with NMOSD-associated optic neuritis,24,25 the elderly patients in the present study who suffered optic neuritis as an attack symptom were more likely to experience MNI. Indeed, one patient with optic neuritis failed to respond to PLEX entirely. Elderly patients with optic neuritis attacks were also more likely to fail to achieve a significant functional score reduction until 6 months. It was found that severe optic neuritis attack in elderly patients was a significant prognostic factor independently associated with poorer response to PLEX. This agrees with another study. 25 Of note, in our elderly group, 85.7% of optic neuritis attacks were defined as severe, which may explain the poor outcome in our study. Moreover, the comorbidities of hypertension and DM in the elderly may have worsened the rate of visual function improvement. Because NMOSD-related optic neuritis appears refractory to PLEX, or response is delayed especially in the elderly, PLEX should begin earlier or combined sequentially with other initial treatment.26,27
PLEX is a technically demanding and invasive extracorporeal blood purification modality with a risk of treatment-related complications. Any plasmapheresis may physiologically stress the heart and kidneys, but physicians are especially concerned when performing PLEX in the elderly because these patients are more highly prone to comorbidities, vulnerable hemodynamic systems, declined protective immunity, and concomitant medications. Two previous studies evaluated elderly patients with different PLEX indications relative to a younger group and reported that the former experienced a significantly higher rate of adverse events, especially blood clotting in the extracorporeal circuit.15,16 This may have been due to preexisting narrow vascular structures in these elderly patients, and insufficient use of preventive anticoagulant treatment.15,16
Another study noted that among patients undergoing PLEX for neurological indications, the elderly (⩾65 years) had suffered significantly higher mortality 1 year after admission compared with the younger. 14 The authors believed that the increased risk of death was multifactorial (e.g. due to underlying pathology) and not due to the PLEX procedure alone. However, in the present cohort with NMOSD, the two age groups were comparable regarding rates of total and serious adverse events despite the greater prevalence of comorbidities in the elderly. The rate of adverse events in the elderly is consistent with other studies in which patients with NMOSD overall generally tolerated PLEX well.12,20 Furthermore, none of the elderly patients in the present cohort died during the PLEX procedure. These seemingly contradictory findings may be because this study involved only a single indication, the rates of congestive heart failure or renal dysfunction were low, or sufficient anticoagulation therapies were administered.
The development of circulatory problems during PLEX is a major complication, particularly hypotension. Hypotension can be due to vasovagal episodes, inadequate blood volume, allergic reaction, cardiac arrhythmia, or cardiovascular collapse.19,28 In an overall population with NMOSD, the rate of hypotension during PLEX varied from 0.9% to 16.7%.12,13,23,24 However, in this study, the rate in the elderly was 19.2%, possibly due to greater concomitant use of diuretic and antihypertensive drugs. A reduction in dose, or discontinuation, might eliminate subsequent episodes of hypotension in affected patients. Of note is that none of these circulatory complications were serious or prematurely interrupted the PLEX procedure. In addition, one elderly patient complained of transient tachycardia during the PLEX procedure. Altogether, PLEX was well-tolerated by the elderly, even in the presence of preexisting ASCVD. Nevertheless, elderly patients should be given more attention during the PLEX procedure. Preventive measures are necessary to decrease the risk of circulatory problems. These measures include balancing plasma removal, modifying antihypertensive medication, and colloid solution supplementation.
This study is limited by the inherent biases of a retrospective design, a single hospital, a small population, and lack of placebo controls. Moreover, in those patients who received IVMP/IVIg shortly before PLEX, measurement of the short-term efficacy of PLEX may have been confounded by the prior treatment. Hence, the results warrant confirmation by prospective, multi-center, and controlled studies with a larger sample of elderly patients.
Conclusion
In this study of patients with NMOSD, the improvements in neurological and functional outcomes 6 months after PLEX were significant relative to baseline for both the elderly and young cohorts. Despite comorbidities, the response of the elderly was similar to that of the young. The procedure was well-tolerated, with minimal and transitory adverse events, although elderly patients were more prone to transient hypotension when under hypotensive medication. In the elderly, severe optic neuritis was prognostic of poor response to PLEX treatment at the 6-month follow-up. Altogether, PLEX appears safe and effective for elderly patients with NMOSD and should be considered an option during attacks when initial therapies fail or during severe relapse. For elderly patients experiencing optic neuritis, or any patient showing refractory or delayed response to PLEX, earlier initiation of escalating or sequential therapies is highly recommended.
Supplemental Material
sj-docx-1-tan-10.1177_17562864231162420 – Supplemental material for Therapeutic efficacy and safety of plasmapheresis in elderly patients with neuromyelitis optica spectrum disorder: a single-center observational study
Supplemental material, sj-docx-1-tan-10.1177_17562864231162420 for Therapeutic efficacy and safety of plasmapheresis in elderly patients with neuromyelitis optica spectrum disorder: a single-center observational study by Weihe Zhang, Yujuan Jiao, Lei Cui, Yeqiong Zhang, Jinsong Jiao, Ming Jin, Wei Yuan, Yang You, Renbin Wang and Dantao Peng in Therapeutic Advances in Neurological Disorders
Footnotes
References
Supplementary Material
Please find the following supplemental material available below.
For Open Access articles published under a Creative Commons License, all supplemental material carries the same license as the article it is associated with.
For non-Open Access articles published, all supplemental material carries a non-exclusive license, and permission requests for re-use of supplemental material or any part of supplemental material shall be sent directly to the copyright owner as specified in the copyright notice associated with the article.