
Abstract
Background
Neuromyelitis optica spectrum disorders (NMOSDs) are rare antibody-mediated disorders of the central nervous system, with a predilection for the spinal cord and optic nerves. The clinical utility of evoked potential recordings (EPs) has already been established for multiple sclerosis, in particular, that of the abnormal visual evoked potentials (VEP), a key criterion in the McDonald diagnostic criteria for MS. However, there have been few reports on EPs in patients with NMOSD.
AIM
The aim of our study was to assess the possible involvement of the optical pathway through VEP responses in patients with NMOSD.
Methods
VEPs were prospectively performed in 13 patients with NMOSD. All the patients were recruited from the outpatient clinic of a demyelinating diseases center. The recording was done as recommended by the International Federation of Clinical Neurophysiology.
Results
We evaluated the eyes of 12 women with a mean age of 42 years and of one man who was 25 years old. In 6 of the examined eye samples, a response was not obtained, while in the remaining 20 eye samples, we found a significant increase in P100 latency without amplitude change.
Conclusion
VEPs showed a significant increase in P100 latency. VEP assessment is a non-invasive, painless, fast, and low-cost exam that provides neurophysiological data for diagnosis of NMOSD.
Highlights
The recording of visual evoked potentials provides us with evidence of the optic nerve involvement in optic neuromyelitis; in this study, we evaluated 26 eyes of patients diagnosed with NMOSD, registering the absence of response or delayed P100 latency significantly.
Introduction
Neuromyelitis optica (NMO) and neuromyelitis optica spectrum disorders (NMOSD) are rare antibody-mediated astrocytopathy disorders of the central nervous system, with a predilection for the spinal cord and optic nerves. Initially known as Devic’(tm)s disease, its first clinical descriptions date back to the 19th century, when it was a challenge to differentiate this from multiple sclerosis (MS), as an autoimmune inflammatory, demyelinating disease of the central nervous system.1-3 The hallmark manifestations are mainly recurrent extensive longitudinal involvements of the spinal cord and optic nerves. Identification of the aquaporin antibody (AQP4-Ab) has extended the clinical concept of NMO to the concept of NMO spectrum disorders (NMOSD), which includes brainstem syndromes, such as intractable hiccups and nausea, hypothalamic syndrome, and brain injuries. 4
While the first diagnostic criteria separated NMO and NMOSD based on clinical data, the criteria developed in 2015 defined a single diagnosis under the term NMOSD. 5
We have no evidence till date regarding whether ethnic or genetic origins play an important role in the development of NMO/NMOSD. Their similar global prevalence, and the lack of a clear latitude gradient of NMO/NMOSD prevalence, argues against an important role for sun exposure and vitamin D levels in conferring individual disease risk for NMO/NMOSD. 6
Since 1980, cerebrospinal fluid examination and magnetic resonance imaging have provided a powerful means to examine a large series of NMO cases, giving us the opportunity of revising and possibly clarifying the clinical criteria. The occurrence of optic neuritis and myelitis could be coincidental or separated by an interval that could range from months to years. The disease could follow a monophasic or a relapsing course.4,5
The term NMOSD first proposed in 2006 has not been clearly defined and is not used properly at all times. 4 These new criteria stratify patients by AQP4-IgG serological status. The presence of AQP4-IgG is now sufficient for the diagnosis of NMOSD when associated with 6 different central clinical presentations: optic neuritis, transverse myelitis, post-extreme area syndrome, other brainstem syndrome, acute diencephalic syndrome, and symptomatic brain syndrome, that is, any type of episode involving the central nervous system. In the absence of AQP4-IgG, neuroimaging findings and rigorous clinical features need to be added to the criteria accordingly.7,8
The clinical utility of evoked potential records (EPs) has already been established for MS, in which EPs can detect clinically silent lesions in the visual, auditory, and sensory pathways, even suggesting a prognosis for EPs in MS and an association between EP abnormality and the level of clinical disability. Recent studies are beginning to reveal the role of EPs and their possible value as a diagnostic tool for NMO, which is also the aim of this study.
Methods
The visual evoked potentials (VEP) were prospectively measured in 13 patients with NMOSD according to International Panel for NMO Diagnosis criteria of 2015. 5 All the patients were recruited from the outpatient clinic of a demyelinating diseases center at the Hospital of Clinics at Federal University of Paraná, Curitiba, Brazil.
Visual evoked potentials were obtained using full-field monocular stimulation with black-and-white checkerboards (12 mm/41 min), reversed at a rate of 1.5–2/s. Nihon Kohden MEB-9400 was used, following the same technical parameters established by the American Society for Clinical Evoked Potentials and International Society for Clinical Electrophysiology of Vision,9,10 including constant contrast and luminance. VEPs were recorded in 2 trials for each eye, averaging 200 responses, with electrodes positioned at Oz (active) and Fz (reference) for channel 1 and Oc (contralateral occipital) and Fz for channel 2 sites, respectively. We measured peak latencies of N75, P100, and N145. Cutoffs for normal values were < 115 ms for P100-peak latencies and ≥ 3 μV for P100-N140 peak-to-peak-amplitudes.
For each latency variable (P100 Oc, P100 Oz), patients were categorized as “Normal” or “Abnormal.” If one of the patient’(tm)s eyes was considered “Abnormal,” the patient was categorized as “Abnormal.” Otherwise, the patient was categorized as “Normal.”
The VEP variables were also created similarly; for example, the patient was considered abnormal in relation to the VEP if he had at least one “abnormal” eye in relation to the variables P100 Oc and P100 Oz.
Subsequently, the variables of age, gender, AQP4-Ab, and latencies were compared between the 2 groups (Abnormal vs Normal). The P value in the table refers to the two-tailed test.
Regarding demographic data (ages) and the proportion of positive/negative antibody, there was no statistical difference between the “Normal” and “Abnormal” groups, regardless of the latency variable used to perform the categorization.
Statistical analysis
In the descriptive analysis, continuous variables were expressed in terms of summary measures (mean, median, standard deviation, and quartiles), while categorical variables were expressed in terms of percentages.
For the comparison of the 2 groups in terms of the continuous variables, the t test was used for variables that followed a normal distribution (Anderson–Darling test). The non-parametric Mann–Whitney and Brunner–Munzel tests were used for homogeneous and heterogeneous variables (Bartlett test), respectively. Fisher’(tm)s exact test was used for categorical variables. The level of significance adopted in the tests was .05. Software R version 3.6.0 was used to perform all the analyses.
The study was prospective approved by the Local Ethics Committee for Human Research of the Hospital de Cliínicas da Universidade Federal do Paraná, with the approval number 4.340.521. All studies were conducted in accordance with ethical principles of the Helsinki Declaration after obtaining written informed patient consent.
Results
We evaluated 12 women with a mean age of 42 years and one man who was 25 years old. Total 77% of the patients tested positive for AQP4-IgG, with assay indirect immunofluorescence. Only 3 patients were negative, and no anti–MOG-Ab was performed in these patients. The mean age at disease onset was 29 years and only 3 patients had comorbidities (anemia, diabetes mellitus, and Sjogren’(tm)s syndrome).
All patients had a history of optic neuritis (ON); however, none of them had acute ON during VEP.
Demographic characteristics, P100 latency and AcAQP4.
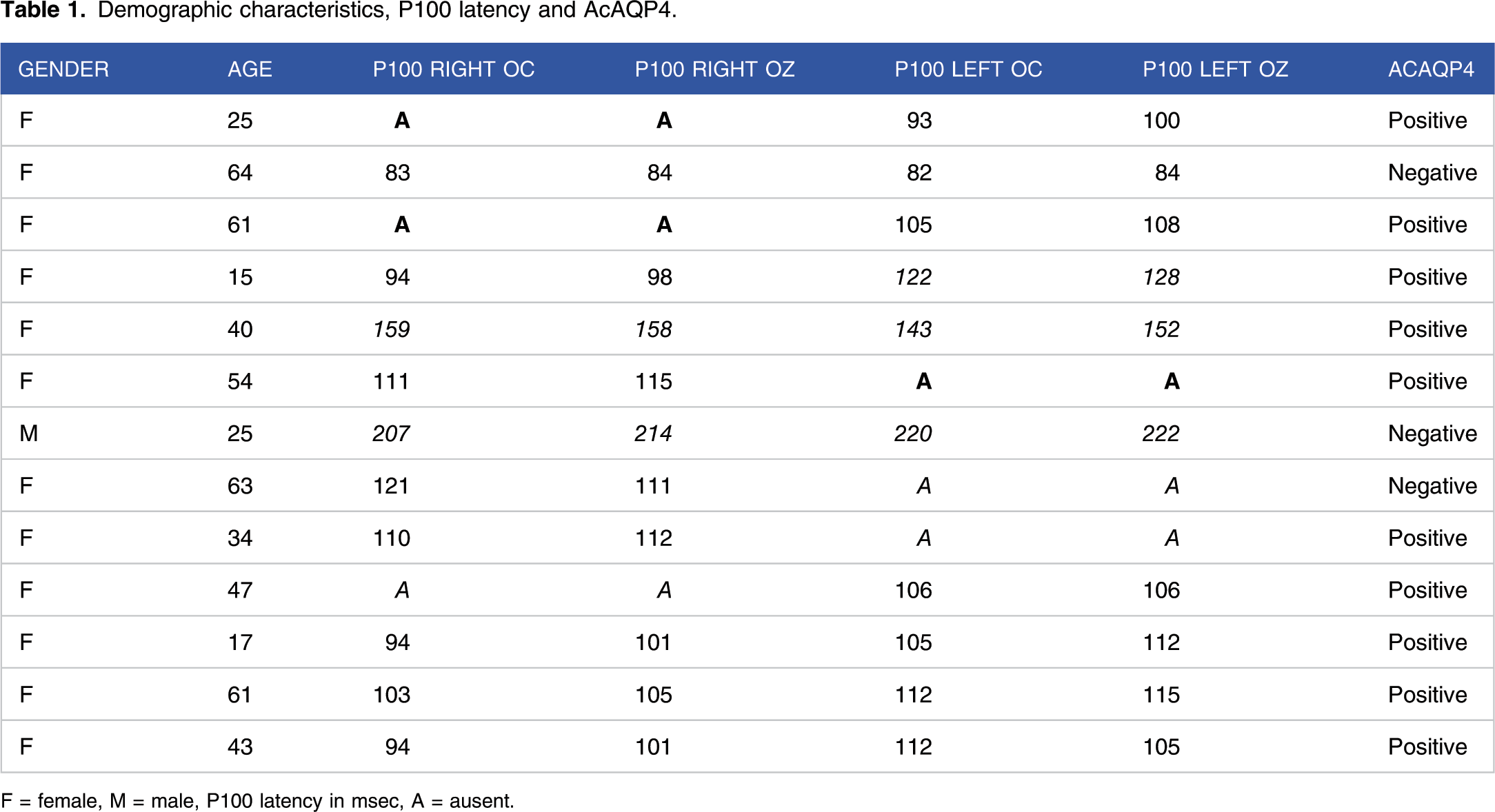
F = female, M = male, P100 latency in msec, A = ausent.
Age, disease time, visual evoked potentials, and positivity for AQP4-Ab.

*Age in years; **msec P: people; E: eyes.
When categorized in relation to the variable P100 Oc (Normal x Abnormal), there was a statistical difference in relation to P100 Oz latencies. There was also a statistical difference in relation to the P100 Oc latency itself, in which Normal patients had an average P100 Oc latency of 98.12 ± 11.83 and the Abnormal patients had an average of 132.58 ± 42.35 (P = .034 two-tailed hypothesis).
In relation to the variable P100 Oz (Normal x Abnormal), the same result was observed as when patients were categorized in relation to the variable P100 Oc, since the categorization between Normal and Abnormal was exactly the same.
Comparison of groups with VEP Normal vs Abnormal.

SD: standard deviation; F: female; ms: miliseconds; in green P value significant.
Discussion
VEP is a well-known non-invasive tool for investigating the function of the visual system. 11 Decreased amplitude and prolonged latency of VEP recording is believed to reflect axonal damage and demyelination in the optic nerve. 12
There are only a few studies reporting electrophysiological examinations in NMO. An Australian study revealed abnormal VEP more frequently in opticospinal demyelinating disease than in conventional MS (85% and 71.4%, respectively). 13 In a multi-ethnic Cuban NMO study, reported VEPs were abnormal in 83% (44/53) of the sample. 14 VEP and somatosensory evoked potentials examination in patients with NMO frequently reveal abnormalities, whilst peripheral nerve conduction studies are expected to be normal. 15
VEP is widely available and has a relatively low cost. If validated, it may help raise the suspicion of NMOSD, particularly in AQP4-antibody–negative subjects, and also help elucidate the prevailing pathophysiology mechanisms.
Frequent latency prolongations in >40% of NMO eyes, and a less frequent occurrence of amplitude reductions has been demonstrated, suggesting a mainly demyelinating affection of the visual pathway. 16 We also noticed delayed P100 responses, even in eyes without previous history of ON, suggesting subclinical involvement.
However, data on VEP latency in NMOSD are less established. In a Japanese cohort study, it was found that P100 was delayed over 121 ms (30′ check-size) in only 1/6 (17%) AQP4+ patients with a non-absent VEP response, compared to 28/64 (44%) MS patients with delayed latency. 17
Therefore, a specific VEP “NMO pattern” with normal latency and isolated amplitude reduction was suggested 18 based on the only previous study conducted among Brazilian subjects that reported latency delay over a threshold of 117.6 ms (43′ check-size) in 2/20 (10%) NMOSD eyes with recordable VEP. In relation to the study carried out in Rio de Janeiro, our study showed 2 important differences that might justify why we could not find a change in the amplitude, and only in the latency, of the P100. Our patients were Caucasian, while 73.7% of patients in the Rio de Janeiro study were African-Brazilian. Further, a greater majority of our patients were seropositive (76.9%) compared to patients in the Rio de Janeiro study (21%). 18 In a previous study, Kay et al analyzed the genetic susceptibility to NMO as well as the relationship between HLA genotypes and susceptibility to the disease in the southern Brazilian population. They found that the HLA genotype was different to that reported previously for other Brazilian populations. 19
As published in a study conducted on the European population, considering both ON+ and ON– eyes, 36/74 (49%) NMO eyes with non-absent VEP had P100 latencies equal or higher than 120 ms (41′ check-size). Among eyes with ON history, a higher rate of VEP delay was found, with average latency of 131.2 ± 20.7 ms. 16
Our data confirmed findings by Ringelstein et al, who provided evidence of VEP latency delay occurring independently of acute ON. 20
A study investigating the utility and limitations of optical coherence tomography and VEPs for detecting ON in NMOSD reported that VEPs appeared to be more sensitive for subclinical and first-ever ON. 21 Recently, a study comparing healthy controls and patients with MS and NMOSD, showed that foveal morphometry reveals a wider and flatter fovea in NMOSD patients, suggesting that this effect is, at least in part, independent of ON, thus proposing the existence of a primary retinopathy in AQP4-IgG seropositive NMOSD. 22
The fact that a high proportion of patients with anti-AQP4 antibody lacked VEP responses suggests critical roles for the antibody in severe optic nerve impairment. A delay in the initiation of immunological treatment for this condition may lead to a loss of visual function. 17 In addition, all of the NMOSD patients who tested positive for anti-AQP4 antibodies may be associated with high prevalence of loss of VEP on account of severe visual impairment. 23
A limitation of our study is the possible bias in the selection of patients in the sample, which was carried out in a single, specialized center.
Our results reinforce the concept of VEP evaluation, which is currently the standard method used to confirm the presence of clinical and subclinical ON. 24 Visual evoked potentials is a non-invasive, painless, fast, and low-cost exam that provides data which can be used as a neurophysiological biomarker of the disease in NMO. We think that is necessary to conduct more studies to understand the prognostic role of VEP and its relationship with concomitant therapy.
Footnotes
Author’(tm)s note
Otto Jesus Hernandez Fustes: Conceptualization, data curation, investigation, methodology, formal analysis, project administration; Roles/Writing—original draft. Cláudia Suemi Kamoi Kay: Conceptualization, data curation, formal analysis, investigation, methodology, validation, visualization, project administration; Roles/Writing. Paulo José(c) Lorenzoni: Conceptualization, data curation, formal analysis, investigation, methodology; Roles/Writing. Renata Dal-Pra Ducci: Conceptualization, data curation, formal analysis, investigation, methodology; Roles/Writing. Lineu Cesar Werneck: Conceptualization, validation, visualization, supervision; Writing—review and edit. Rosana Herminia Scola: Conceptualization, validation, visualization, formal analysis, project administration, supervision; Writing—review and edit.
Declaration of conflicting interests
The author(s) declared no potential conflicts of interest with respect to the research, authorship, and/or publication of this article.
Funding
The author(s) received no financial support for the research, authorship, and/or publication of this article.