
Abstract
Background:
Although the pathogenesis of myasthenia gravis (MG) is well known, prognostic markers are not yet available. We assessed the utility of anti-acetylcholine receptor (AChR) antibody (AChR-ab) titer and concentration of C3, C4, and C5a as potential severity biomarkers in MG.
Methods:
Levels of C3, C4, C5a, and AChR-ab were measured in 60 AChR-ab-positive patients with MG. Their relationship with clinical severity was analyzed using the activities of daily living (ADL) and MG composite (MGC) scales.
Results:
AChR-ab titer correlated with severity of MG according to ADL (p = 0.002) and MGC scales (p = 0.001). When patients were classified according to disease duration, a statistically significant correlation between AChR-ab titer and clinical severity was only found in the subgroup of patients with fewer than 5 years from symptoms onset. C5a levels showed a positive correlation with MG severity according to the ADL scale (p = 0.041; τb = 0.18), although C5a levels were not different from the control group.
Discussion:
AChR-ab titers and C5a levels could potentially be considered markers of severity in patients with MG.
Keywords
Introduction
Myasthenia gravis (MG) is an organ-specific autoimmune disease mediated by autoantibodies directed against proteins of the neuromuscular junction. 1 It is reported that 85% of patients with MG develop autoantibodies against the nicotinic acetylcholine receptor (AChR-abs), and these antibodies destroy the postsynaptic membrane and decrease the number of receptors and ion channels in this membrane.2–4 The mechanisms by which AChR-abs affect neuromuscular transmission involve complement activation, 5 acceleration of the degradation and internalization of AChRs, and functional blockade of receptors. 6 In addition to AChR-abs, pathogenic antibodies against other postsynaptic membrane proteins, including muscle-specific tyrosine kinase and low-density lipoprotein 4, have been identified.7,8
Antibodies against AChRs, particularly isotypes IgG1, IgG2, and IgG3, activate the classical complement pathway in MG, 9 beginning with the recognition of the antigen/antibody immunocomplex. Complement proteins are cleaved sequentially by convertases, thereby producing two factors (a and b). After the hydrolysis of C5, C5a is released into the circulation, and C5b binds to the next protein to continue the activation cascade. The membrane attack complex is formed as an end product of the activation cascade and is inserted into the postsynaptic membrane of the neuromuscular junction causing altered neurotransmission.10–12
Kusner et al. demonstrated that components of the complement system were present in the neuromuscular junctions of patients with MG. 13 Also, IgG and C3 were colocalized in the neuromuscular junctions of an experimental MG model by passive transfer. 14 Recently, a study demonstrated the therapeutic efficacy of eculizumab, an anti-C5 monoclonal antibody, in patients with AChR-ab-positive MG, indicating the active role of complement activation in the physiopathogenesis of MG. 15
Nonetheless, no markers of clinical severity in MG or pharmacodynamic parameters that may support therapeutic decisions in patient management are available to date. 16 Although the analysis of AChR-ab is useful for the diagnosis and serological classification of patients with MG, the efficacy of AChR-abs titer as a marker of severity has been widely questioned.17–24
The objective of this study was to identify biomarkers of clinical severity in patients with generalized AChR-ab-positive MG at different clinical stages. For this purpose, the utility of AChR-abs titer and concentration of complement system factors (C3, C4, and C5a) as potential prognostic markers to identify the severity of MG were evaluated.
Materials and methods
Patients and clinical data
This cross-sectional study was approved by the Bioethics Committee of the José María Ramos Mejía Hospital in Buenos Aires, Argentina. Patients aged >18 years who were diagnosed with generalized AChR-ab-positive MG and referred to the Section of Neuroimmunology and Electrophysiology of this hospital from April 2016 to June 2018 were included in this study. Patients with other associated active autoimmune diseases, infectious disease, pregnant women, patients with cognitive or psychiatric comorbidities that prevented measuring the evaluated parameters, and patients who received treatment with intravenous immunoglobulin or plasma exchange in the 4 weeks prior to consultation were excluded from the study. The study was approved by local ethical committee (Resolution number 97 485/MSG/2011). All study participants signed an informed consent form.
Data regarding sex, age, age at disease onset, duration of MG, presence of thymic abnormalities, history of thymectomy, and type of pharmacological treatment received were collected. A detailed neurological examination was performed using the activities of daily living (ADL) scale and MG composite (MGC) scale. According to the clinical status at the time of examination, the patients were considered to exhibit disease exacerbation in cases where the status deteriorated along with an increase of ⩾3 points in ADL and/or MGC scores with regard to previous consultation. Patients not meeting these criteria were considered to have stable disease.
The effect of immunosuppressive treatment on the prognostic value of complement system components was determined after classifying the patients with either stable or exacerbated disease status into subgroups according to the treatment received at the time of consultation.
Serological tests
AChR-abs were quantified in serum samples at a clinical analysis laboratory by radio-immunoprecipitation single analysis. Values <0.1 nmol/L were considered negative or normal.
Fresh blood samples were centrifuged to obtain serum and plasma. C3, C4, and AChR were measured in the serum, whereas C5a was measured in the plasma, which was obtained using Futhan (BD FUT-175®, BD Biosciences, San Jose, CA, USA) as an inhibitor of the activity of proteases and components of the classical complement pathway in vitro. The samples were frozen at –20°C, and sent to the Department of Immunology of the School of Pharmacy and Biochemistry, where they were stored at –80°C. The sera and plasma of a healthy control group, treated and stored in the same way, were used as negative controls or indicators of the ranges of normal concentrations in each test. This control group consisted of 49 healthy volunteers with a mean age at sample collection of 38 years; 63.6% were women.
Radial immunodiffusion plates (Diffu-Plate, Biocientífica, Buenos Aires, Argentina) were used to measure the concentration of C3 and C4. Briefly, 5 µl of each serum sample was seeded on to the wells of agar plates and, after 48 h, the diameter of the precipitin rings was measured using a magnifying glass. The concentration of each sample (mg/ml) was determined by comparing the obtained diameters with a standard curve provided by the manufacturer. C5a was quantified using an enzyme-linked immunosorbent assay (ELISA) with commercial reagents (LEGEND MAX™ Human C5a ELISA Kit, BioLegend, San Diego, CA, USA). Briefly, ELISA microplates (Nunc) were coated with anti-C5a (desArg) antibodies (1 µg/ml), blocked with 1% phosphate-buffered saline-bovine serum albumin, and incubated with plasma samples in the presence of the inhibitor (1/100) or a standard solution with known concentrations of C5a. The plates were incubated with anti-C5a (desArg) antibodies conjugated with biotin (0.250 µg/ml) and antibodies were detected using streptavidin peroxidase (1/2500). Subsequently, the color reaction was developed with tetramethylbenzidine and stopped with 4N H2SO4. Absorbance was read at an optical density of 450 nm, and C5a levels (ng/ml) were determined using a standard calibration curve.
Statistical analysis
All continuous variables were tested for normality, and the results were expressed as mean ± standard deviation (SD) when the variables followed a normal distribution, median [interquartile range (IQR)] when the variables did not follow a normal distribution, or percentages, as appropriate. Unpaired t-test was used to compare means of variables which followed a normal distribution, nonparametric Mann–Whitney test was used to compare medians of independent variables which did not follow a normal distribution, and tau-b (τb) correlation coefficient test was used for the correlation analyses.
SPSS software (version 25) was used for the statistical analysis.
Results
Clinical records of 205 patients with diagnosis of MG were reviewed. A total of 69 samples from 60 patients (65% women) diagnosed with AChR-ab-positive MG were examined. The median age of onset of MG was 28 years (range: 3–82 years) and the median age at the time of consultation was 39 years (range: 20–88 years). The mean duration of MG was 9 years (range: 0–36 years); 23% of the patients had been thymectomized. At the time of examination, 19 patients presented with exacerbated MG and 50 patients had stable MG. The clinical characteristics of the disease and treatments are detailed in Table 1.
Clinical characteristics of patients with acetylcholine receptor-antibody-positive myasthenia gravis.

The complement factors, C3 and C4, and AChR-ab were measured in all samples. C5a was measured in 64 of 69 samples. The mean concentration of C3 was 1.22 mg/ml (SD 0.3 mg/ml), and the mean concentration of C4 was 0.24 mg/ml (SD 0.08 mg/ml); the means of both markers were within the reference range (C3: 0.84–1.93 mg/ml; C4: 0.2–0.4 mg/ml), and were not significantly different from the mean levels in healthy controls (C3: 1.18 mg/ml; C4: 0.22 mg/ml).
The median serum level of C5a was 16.5 ng/ml (IQR = 25.9 ng/ml; range = 6.9–127.0 ng/ml). The median concentration of C5a in healthy controls was 21.1 ng/ml (IQR = 36 ng/ml; range = 3–79 ng/ml). There was no significant difference in the levels of C5a between the groups. The mean AChR-ab titer was 4.7 nmol/L (SD 2.8 nmol/L).
The levels of C3, C4, and C5a were related to the clinical severity of MG. There was no difference between stable and exacerbated MG, or MGC score. Nonetheless, there was a correlation toward higher levels of C5a in patients with higher scores on the ADL scale (p = 0.041; τb = 0.18) (Figure 1).
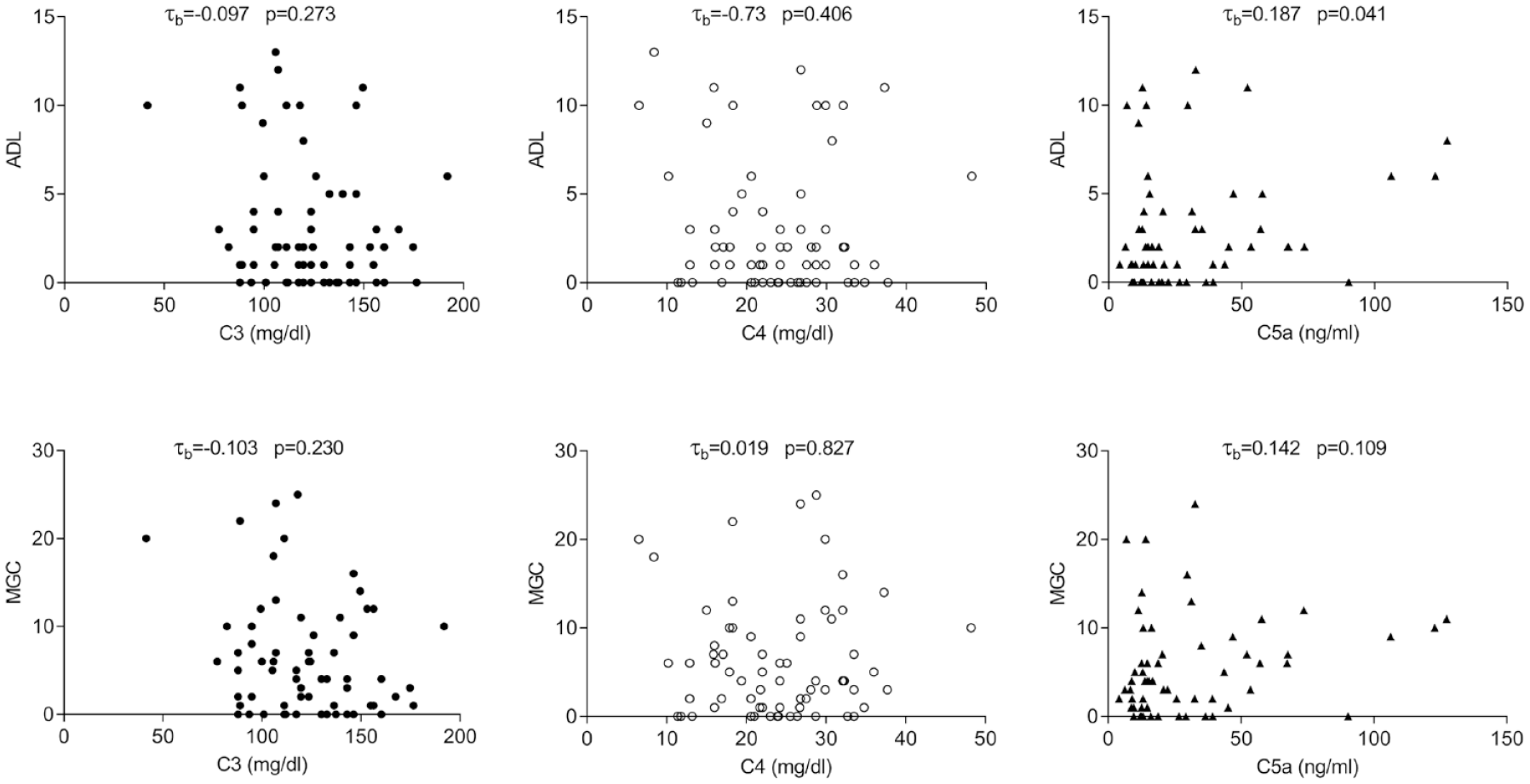
Correlation of C3, C4, and C5a with clinical severity of MG. p > 0.05, not statistically significant.
On the other hand, there were stronger correlations with AChR-ab levels. There was a positive correlation between AChR-ab titers and MGC and ADL severity scores (Figure 2), and a strong trend towards higher titers in patients with exacerbated MG than in those with stable MG (5.9 nmol/L and 4.7 nmol/L, respectively), (p = 0.06) (Figure 2).

Correlation of AChR-ab titers with clinical severity of myasthenia gravis. p > 0.05, not statistically significant.
When we stratified patients according to disease duration, the subgroup with fewer than 5 years from symptoms onset showed a trend toward higher levels of C5 (p = 0.057) and lower levels of C3 (p = 0.06) in patients with higher clinical severity on the ADL scale. Also, a statistically significant positive correlation between AChR-ab titer and clinical severity was only found in this subgroup of patients (ADL: τb = 0.36. p = 0.004; MGC: τb = 0.34, p = 0.006). The associations between complement and antibody titers with disease severity were not different between genders.
The relationships between C3, C4, and C5a levels with AChR-ab titers were also analyzed. The levels of C3 (mean 1.25 mg/ml), C4 (mean 0.25 mg/ml), and C5a (median 18.8 ng/ml; IQR = 33.8 ng/ml) in patients with AChR-ab titers above the median (4.7 nmol/L) were not significantly different from the levels in patients with AChR-ab titers below the median (C3: 1.19 mg/ml; C4: 0.22 mg/ml; C5a: 16 ng/ml: IQR = 21.6 ng/ml).
The concentration of C3, C4, C5a, and AChR-abs in the subgroups of patients according to gender, presence of thymic abnormalities, and history of thymectomy were not different. However, there was a positive correlation between the age of onset of MG and C3 and C4 levels, with lower titers observed in patients with early onset disease (C3: r = 0.31, p = 0.009; C4: r = 0.25, p = 0.041).
Finally, comparing patients with or without immunosuppression, both AChR-abs (mean 5.16 nmol/L and 3.14 nmol/L, respectively; p = 0.01) and C5a levels (median 20 ng/ml and 13.9 ng/ml, respectively; p = 0.03) were higher in immunosuppressed patients than those receiving pyridostigmine only, with no changes in C3 or C4 concentration (Figure 3).
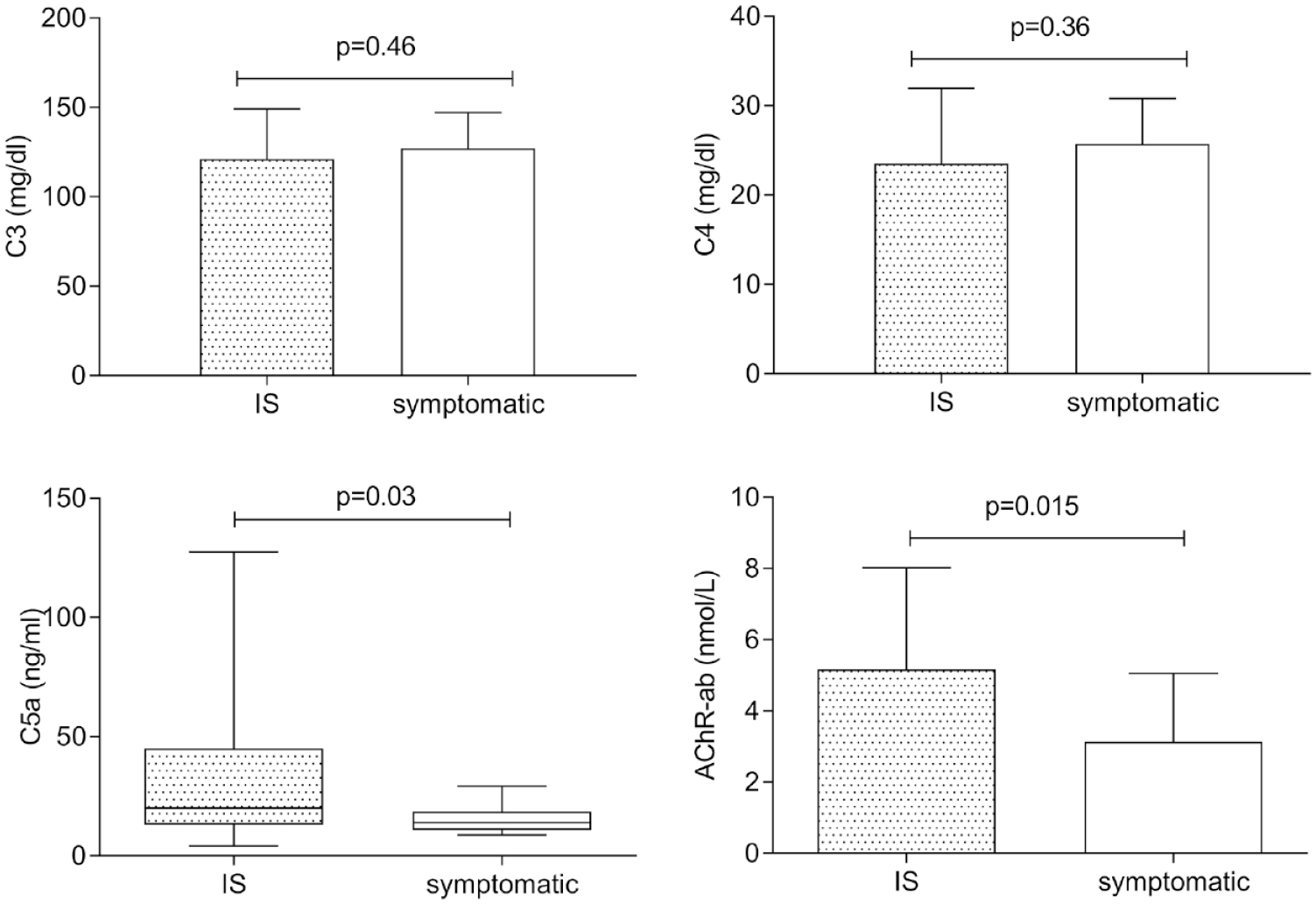
Mean levels of C3, C4, and AChR-ab and median levels of C5a in patients receiving either immunosuppressive (n = 55) or symptomatic treatment (n = 14). p > 0.05, not statistically significant.
The patients were then classified into five groups according to the pharmacological treatment they had received: group 1, symptomatic treatment with pyridostigmine (14 patients); group 2, corticosteroid therapy with or without symptomatic treatment (19 patients); group 3, azathioprine treatment with or without symptomatic treatment (7 patients); group 4, azathioprine and corticosteroid treatment with or without symptomatic treatment (25 patients); group 5, treatment with other immunosuppressive drugs such as rituximab and mycophenolate mofetil (4 patients). The cutoff values for C3, C4, and C5a were determined using the median value in each treatment group. The clinical severity of MG based on the mean values of the MGC and ADL scales was compared between the treatment groups. Only in group 4 (azathioprine + corticosteroids) was there a trend to higher levels of C5a in patients with higher clinical severity on both the MGC and ADL scales.
Discussion
The search for biological markers capable of determining the severity or clinical progression of MG and supporting therapeutic decisions to avoid exacerbations in patients with MG is underway. However, a biomarker that meets these criteria has not yet been identified. The complex pathogenesis of MG, i.e. its high variability in biological responses due to disease dynamics, which is characterized by constant changes in the synthesis and degradation of molecules, and the variable immune response to different immunosuppressive therapies used to control disease progression, have hindered the identification of a useful biomarker.
Considering current knowledge regarding the activation/participation of the complement system as a primary pathogenic mechanism in AChR-ab-positive MG, 25 the relationship between complement system factors, C3, C4, and C5a, and the clinical status of patients with MG at the time of consultation was analyzed. Also, this study focused on AChR-ab titer and the correlation with severity of MG.
The relationship between AChR-abs titers and clinical severity of MG has been previously investigated, but the results were inconsistent. Some studies found that antibody titers were higher in patients with more severe MG,17–22 whereas others showed that this correlation with severity could only be proven within the same patient, performing serial measurements of AChR-abs. 26 On the contrary, other studies found no significant correlation between a decrease in antibody titers and clinical improvement or vice versa.23,24
Our results demonstrated that there was a positive association between AChR-abs titers and the clinical severity of MG according to ADL and MGC scores. When we stratified patients according to disease duration, the association between ADL and MGC scores and AChR-ab concentration was only found in patients with a more recent diagnosis of MG, and was no longer significant after 5 years from symptoms onset. This association between AChR-abs titers and MG severity in patients with short disease duration has been previously reported by Heldal et al. in a retrospective analysis of patients with MG who had repetitive determinations of AChR-ab concentration in the follow up. 22 Our results suggest that AChR-ab titers may be a useful marker of disease severity in patients with MG with generalized AChR-ab-positive MG, particularly in patients with shorter disease duration. However, our transversal study design did not allow a statistical comparison at an intra-individual level, which could be relevant, as has been described previously.
Experimental studies have provided evidence that variations in serum concentration of different complement system components might affect the clinical course of MG; 27 complement depletion protects animals against the induction of experimental autoimmune MG (EAMG), 14 antibodies that block the soluble C1q receptor protect animals against EAMG, 28 and animals with reduced complement function secondary to genetic defects are not affected by EAMG. 29 On the other hand, Romi et al. 30 reported that the serum levels of C3 and C4 were decreased in patients with high AChR-ab titers regardless of clinical severity, and only serum complement consumption was associated with antibody titers and not the clinical status of patients with MG. In contrast, a previous study found a relationship between C3 levels, clinical status, and response to treatment in patients with AChR-ab-positive MG. 31 To the best of our knowledge, no studies to date have evaluated C5a levels in patients with AChR-ab-positive MG.
In the global analysis of 69 samples from 60 patients with AChR-ab-positive MG, we found a significant correlation between the levels of C5a and disease severity on the ADL scale. There was no significant correlation between the levels of C3 and C4 and severity scores on the ADL or MGC scales, and there were no significant differences in the concentrations of these factors between patients with stable and exacerbated MG.
In contrast to the results of the study by Romi et al. 30 our results could not demonstrate a relationship between higher AChR-ab titers and a decrease in the levels of complement factors. This discrepancy may be due to different pharmacological profiles in these populations, with a higher percentage of patients treated with immunosuppressive drugs in our study.
Overall, the complexity of the disease added to the intricacy of the complement system, which makes it difficult to arrive at relevant conclusive findings evaluating a limited set of complement factors. There are still many more unexplored aspects of MG to look at in relation to complement.
One limitation of this study was the great heterogeneity regarding the treatment received in our patient population. The differences in pharmacological profile and, therefore, in clinical severity make it difficult to compare groups of patients. Also, the method used to assess AChR-ab titers was a single analysis radio-immunoprecipitation and not a serial titration assay making sera dilutions.
In conclusion, the present study demonstrates that AChR-ab titers may be a useful marker of disease severity regardless of the adopted treatment and serum complement levels. C5a concentration was higher in patients with more severe MG, however, there were no differences in levels between patients and healthy controls. So C5a is a nonspecific marker in patients with MG. Further studies are necessary in order to confirm the usefulness of complement factors as a biomarker of MG.
Footnotes
Acknowledgements
The authors would like to thank Professor Angela Vincent (Neurosciences Group, Department of Clinical Neurology, MRC Weatherall Institute of Molecular Medicine, University of Oxford, UK) for her helpful insights.
Conflict of interest statement
The authors declare that there is no conflict of interest.
Funding
This work was supported by grants UBACyT20020150200007BA 2016-2018 from the University of Buenos Aires and Research Grant 2016-2018 from the Roemmers Foundation. Funding sources were not involved or had any role in this study.