
Abstract
Objectives:
Therapeutic options in progressive forms of multiple sclerosis (MS) are still limited. Dimethyl fumarate (DMF) has immunomodulatory properties but may also exert antioxidative cytoprotective effects. Hence, it may be a therapeutic option for progressive MS. The aim of this observational study was to evaluate safety, adherence and efficacy of fumarates in patients with primary progressive MS (PPMS) or secondary progressive MS.
Methods:
Patients with progressive MS whose condition had failed to respond to standard therapies and had worsened received the fumarate mixture Fumaderm, licensed for psoriasis therapy in Germany, or DMF by pharmaceutical preparation (Bochum ethics approval no. 4797-13). At regular follow-up visits, tolerability and disease course were assessed.
Results:
Twenty-six patients [age 54 ± 7.8 years; female = 13 (50%); PPMS = 12 (46.2%); Expanded Disability Status Scale (EDSS) = 6.0 ± 0.4 (range 3.5–8.0); disease duration = 14.1 ± 8.7 years] were initiated on treatment with Fumaderm (n = 18) or pharmacy-prepared DMF (n=8). During a mean follow-up period of 13.2 ± 7.5 months (range 6–30) only five patients (19.2%) reported minor complaints. In 15 patients (57.7%) EDSS remained stable. In five cases (19.2%) there was even a decrease in EDSS while in six patients (23.1%) there was an increase in EDSS of more than 0.5 points, reflecting deterioration. Laboratory values were controlled for lymphopenia, renal and hepatic values, without any safety problems. We observed no significant differences between the two pharmaceutical forms.
Conclusion:
Our pilot data indicate that fumarate therapy appears to be safe and well tolerated by patients with progressive MS. In more than 75% of cases no further disease progression was evident. However, controlled studies are warranted to evaluate the detailed therapeutic potential of fumarates and their long-term effects in progressive MS.
Introduction
Multiple sclerosis (MS) is one of the most common autoimmune diseases among young adults [Koch-Henriksen and Sørensen, 2010]. Disease activity and progression of disability is determined by combination of inflammation and oxidative stress [Gold et al. 2012; Linker et al. 2011]. Thereby, it is assumed that the progressive course of the disease is dominated by neurodegenerative phenomena [Gilgun-Sherki et al. 2004]. However, therapeutic options for these progressive forms of MS are still very limited [Comi, 2013].
Dimethyl fumarate (DMF) is an oral compound that has recently been approved in Europe (brand name Tecfidera, Biogen Idec Ltd, Berkshire, UK) and is now available to treat relapsing-remitting MS (RRMS). Originally, a mixture of compounds consisting of DMF and three salts of ethylhydrogenfumarate was licensed in Germany in 1994 as oral therapy for severe psoriasis under the brand name Fumaderm (Biogen Idec GmbH, Ismaning, Germany). Positive effects of Fumaderm on course of RRMS were first seen in a small exploratory, open-label study in 2006 [Schimrigk et al. 2006].
Recently, two phase III studies demonstrated efficacy of DMF in patients with RRMS across a range of clinical analyses and magnetic resonance imaging endpoints [Gold et al. 2012; Fox et al. 2012]. Besides their immunomodulatory properties, DMF also exerts antioxidative cytoprotective effects. As oxidative stress and inflammation are supposed to play a key role in neurodegeneration [Lassmann, 2013], DMF might be a therapeutic option to treat progressive forms of MS [Gold et al. 2012; Linker et al. 2011; Johnson et al. 2010]. Although its mode of action is not fully understood, it is known that DMF reduces oxidative stress via activation of the nuclear 1 factor (erythroid-derived 2)-like 2 (Nrf2) antioxidant response pathway. Activation of this pathway induces neuroprotective effects in an animal model of chronic MS [Linker et al. 2011]. These neuroprotective features of DMF could also be demonstrated in animal models of neurodegenerative diseases like Huntington’s disease [Ellrichmann et al. 2011].
Here we report the first data on patients with a progressive course of MS treated with DMF in an observational study to evaluate safety, adherence and efficacy of fumarates in primary progressive MS (PPMS) or secondary progressive MS (SPMS).
Methods
Study population
We recruited patients from the Department of Neurology of the St Josef-Hospital, Ruhr University, Bochum. Key inclusion criteria were patients aged 18–80 years with a progressive form of MS according to the revised McDonald criteria [Polman et al. 2005; Lublin and Reingold, 1996]. Consecutive patients with MS were treated with the fumarate mixture Fumaderm (215 mg total fumarates), approved for psoriasis therapy in Germany, or DMF (240 mg capsules) by pharmaceutical preparation. Principally, treatment was initiated with Fumaderm and it was switched to the pharmaceutical preparation when there were incompatibilities, or if this was requested by the patient at the beginning. Fumarate mixture or DMF treatment was initiated and dosage slowly tapered in within 4–6 weeks. Indication was made in accordance with the treating physician’s recommendation based on progression of disability of the patient and antecedent failure of standard immune therapies. Patients with RRMS were excluded [Lublin and Reingold, 1996]. Other exclusion criteria were pregnancy, abnormal results on prespecified laboratory tests or recent exposure to long-term active immune medications. Costs for off-label treatment were negotiated on an individualized basis with the respective healthcare provider.
All patients were included in a computerized data bank, and their demographic characteristics, sum scores of standardized disease evaluating scores and relevant laboratory tests were documented. Patients with MS were prospectively followed up and clinically reevaluated at regular elective hospital stays or at adapted intervals at the outpatient clinics of our institution by consultants in neurology.
The study was approved by the local university ethics committee (Bochum ethics approval no. 4797-13) and was conducted in accordance with the International Conference on Harmonization Guidelines for Good Clinical Practice and the Declaration of Helsinki.
Clinical and paraclinical assessment
Disease course was evaluated clinically by standardized neurological assessments, including the Expanded Disability Status Scale (EDSS) [Krutzke, 1983]. The EDSS was performed by specialized neurologists who were certified either by in-person training or through an online program (www.neurostatus.net) by experienced investigators (KSK, GE and RG).
Common side effects of fumarates like flushing, gastrointestinal events like diarrhea, nausea, abdominal pain and vomiting, as well as pruritus and rhinorrhea were explicitly assessed.
Laboratory tests included blood count analysis with white cell count and lymphocyte count, renal retention parameters and transaminases. Great care was taken to avoid critical values of lymphopenia (<500/μl) or leucopenia (<3000/μl).
Statistical analyses
Continuous parametric and nonparametric data are presented as mean ± standard deviation (SD) or as median (range), respectively. Noncontinuous variables are presented as percentages. No formal sample size estimation was performed since this was an observational study and as such approved by the local ethics committee. The Statistical Package for Social Science (SPSS Inc., version 13.0 for Windows) was used for statistical analyses.
Results
Patients and baseline characteristics
Between July 2011 and April 2013, a total of 26 study patients (13 women) with progressive forms of MS (12 PPMS, 14 SPMS) were initiated on Fumaderm (n = 18) or pharmacy-prepared DMF (n = 8). Patients were 36–74 years old (mean age 56.6 ± 10.0 years) and were diagnosed with MS between 1 and 32 years before study entry (mean disease duration 14.1 ± 8.7 years). EDSS changes were confirmed at a 12-week follow up.
At baseline, EDSS scores ranged between 3.5 and 8.0 (median 6.2 ± 1.3). Patients were initiated on a treatment with Fumaderm (n = 18, 69.2%) or DMF (n = 8, 30.8%). Baseline demographic and clinical data are summarized in Table 1.
Baseline characteristics of the study population.
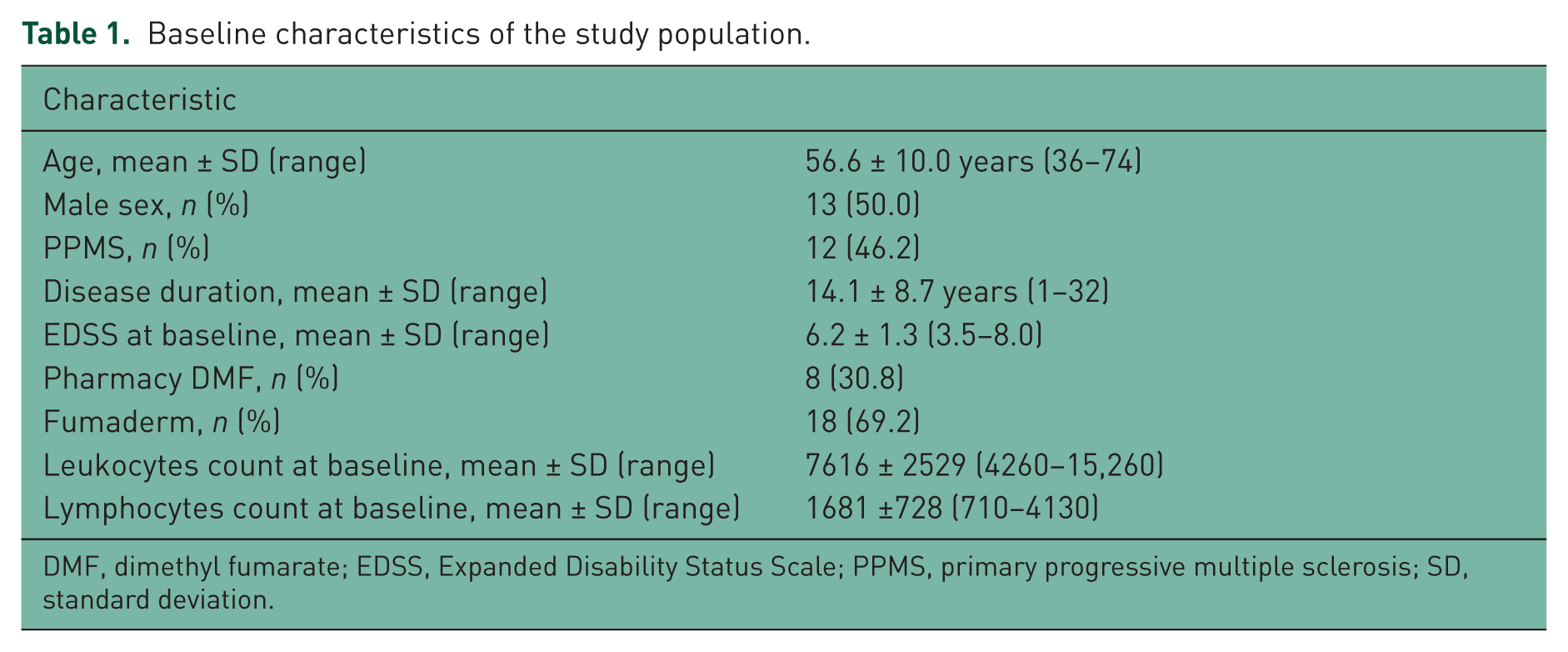
DMF, dimethyl fumarate; EDSS, Expanded Disability Status Scale; PPMS, primary progressive multiple sclerosis; SD, standard deviation.
Median daily dosage of fumarates using Fumaderm was 645 mg (range 215–860 mg) and DMF was 600 mg (range 120–600 mg). In all patients we attempted to titrate the individual dosage to achieve relative lymphopenia following the long-term experience of Peter Altmeyer (personal communication) in dermatological disease.
Patients kept on taking symptomatic therapies prescribed for treatment of spasticity or bladder problems as well as therapy for coexisting diseases.
Safety parameters and adherence
The mean evaluation period was 13.2 ± 7.5 months (range 6–30 months). In this period, five patients (19.2%) reported the following adverse events (Table 2): gastrointestinal events like upper abdominal pain, vomiting or diarrhea (n = 4, 15.4%); flushing and rhinorrhea (n = 2, 7.7%). Of these, one patient (3.8%) had both of these adverse events, resulting in six reported complaints in five patients. The incidence of rhinorrhea and gastrointestinal events was highest in the first 3 weeks after initiation and decreased afterwards. Overall, the extent of the side effects was rather mild, so that no discontinuation of the treatment due to side effects occurred. One patient stopped treatment (3.8%) as the health insurance company finally rejected coverage of the costs.
Safety outcomes of fumarates.
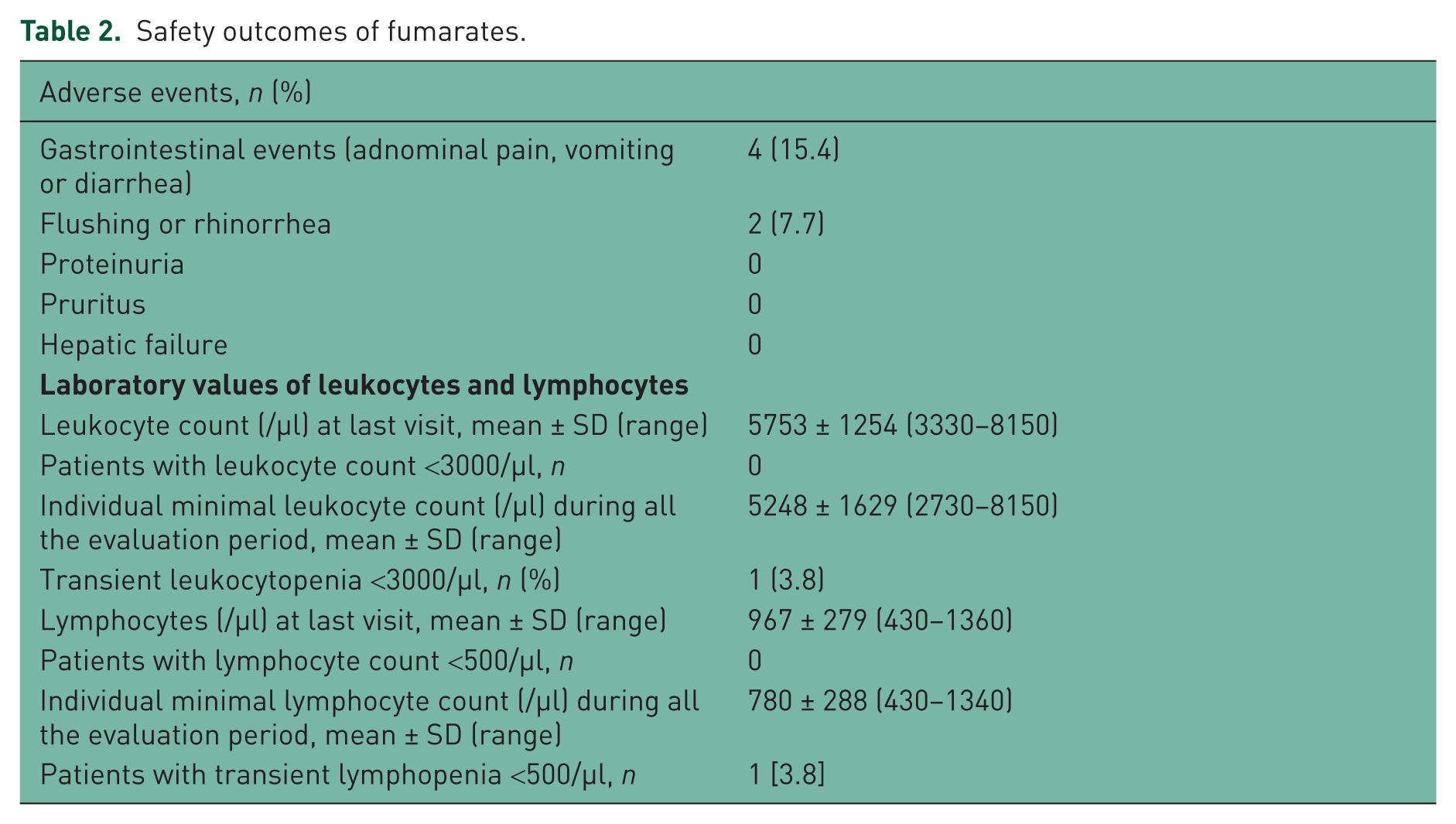
The mean white cell count and lymphocyte count decreased over the first months and then remained static, without any safety problems. There was no report of hepatic failure.
Four of 22 patients (18.2%) being initiated on Fumaderm reported complaints mostly due to gastrointestinal symptoms and were therefore switched to the pharmaceutical preparation, which was better tolerated in these cases. Nonetheless, there was no significant difference regarding the tolerability of these two preparations as one (12.5%) of the eight patients initiated on the pharmaceutical preparation also reported minor side effects (Fisher exact test, p = 0.387). Furthermore, the two treatments did not show any significant difference regarding safety issues (laboratory values of leukocytes and lymphocytes) or efficacy (confirmed clinical progression on the EDSS score).
Disease progression
During a total mean follow-up period of 13.2 ± 7.5 months (range 6–30 months), in 15 (57.7%) of the patients the EDSS scores remained unchanged. The mean follow-up period of this clinically stable subgroup was 12.9 ± 6.5 months (range 6–27 months).
In six cases (23.1%) an increase in EDSS score of more than 0.5 points was reported, reflecting deterioration (Figure 1). In four of these six patients, the increase was 0.5 points (mean follow up 27 ± 4.7 months, range 20–30 months). In one patient the increase was 1.0 point (increase from 5.5 to 6.5 within a follow-up period of 16 months) and in one patient the increase was even 2.0 points (increase from 3.5 to 5.5 within a follow-up period of 19 months).

Disease course according to the course of the EDSS scores, shown in relation to the individual evaluation period of fumarates treatment.
In five patients (19.2%) there was even a decrease in EDSS score during the evaluation period. In four of these patients the decrease was 0.5 points (mean follow-up period 16 ± 5.0 months, range 10–22 months). In one case a decrease of 1.5 points was documented (decrease from 6.0 to 4.5 points within a follow-up period of 18 months). Regarding the follow-up periods, there were no significant differences between these three subgroups.
Discussion
To the best of our knowledge, this is the first study evaluating treatment with fumarates in progressive forms of MS. In progressive forms of the disease the most important therapeutic aim is a stable state and no further disease progression. Importantly, our patients had disease that failed to stabilize under previous standard treatment with mitoxantrone or repetitive steroid pulses and thus had been offered off-label therapy.
Our pilot data indicate that therapy with fumaric acid esters (FAE) appears to be safe and well tolerated in patients with progressive forms of MS. Side effects were mainly gastrointestinal events and rhinorrhea and occurred in about 15% of the patients with low intensity. These results are consistent with those reported in the placeb-controlled phase III studies of oral DMF for relapsing MS [Gold et al. 2012; Fox et al. 2012].
The effects of some pharmacological treatments on disease progression have been studied [Andersen et al. 2004; La Mantia et al. 2012; Montalban et al. 2009; Hartung et al. 2002]. Interferon β1a failed to show convincing effects on the disability progression in SPMS [Andersen et al. 2004]. A Cochrane review summarized a significant decrease of the risk of 3-month confirmed disability progression due to relapse-related disability changes [La Mantia et al. 2012]. Thus, the use of interferon β1b is restricted to patients with ongoing relapses [La Mantia et al. 2012]. In PPMS only a trend to reduce disability progression has been shown [Montalban et al. 2009].
Mitoxantrone has been analyzed in the Mitoxantrone in Multiple Sclerosis Study (MIMS) [Hartung et al. 2002]. Patients with RRMS and SPMS received mitoxantrone or placebo for 24 months. A benefit concerning disease progression could be shown, but the SPMS group was not analyzed separately.
Until today, almost all treatments which have attempted to stop disease progression in progressive MS have an anti-inflammatory effect on the immune system [Comi, 2013]. Thus, symptomatic therapies still represent the core component in the treatment of patients with progressive forms of MS [Thompson et al. 2010].
Taking into consideration that the pathophysiological mechanisms of progressive MS are mainly neurodegeneration rather than inflammation, fumarates might be a possible therapeutic option due to their antioxidative cytoprotective effects [Linker et al. 2011].
In the present study, less than 25% of the patients showed progression according to the EDSS score. In more than 55% of the patients, the EDSS score remained stable and in about 20% a decrease in the disability score was even documented. Regarding the follow-up periods, there were no significant differences between these three subgroups, so there is no indication that the difference in disease progression is due to different lengths of evaluation periods. Overall, the duration of follow up was relatively short. Nonetheless, in placebo-controlled trials, the proportion of patients with PPMS receiving placebo with confirmed disability progression ranged from 19.3% to 38.5% after 48 or 96 weeks, respectively [Hawker et al. 2009].
We observed no significant differences between the two pharmaceutical forms of FAE. There is a growing body of data on the pharmacodynamics and genomic level that ethylhydrogen fumarate, which is a major component of the ‘old Fumaderm’ licensed in 1994 and assembled according to the original positive Schweckendieck experience, exerts different effects from DMF. Obviously, ethylhydrogenfumarate tends to be enriched in the kidney compared with DMF, and gene induction of each monosubstance is different. More importantly, when both fumarates are given together a synergistic gene induction can be observed. So far, these differences have not been further elucidated on the functional protein level [Scannevin et al. 2014].
Limitations in our observational study are obviously the lack of a control group and blinded study design. Studies evaluating a therapeutic effect on progressive forms of the disease are so far mostly negative due to the fact that disease progression is hard to stop. We omitted magnetic resonance imaging measurements because in patients with progressive MS we would have needed baseline monitoring of brain atrophy, and also the impact of gadolinium uptake is limited in progressive MS.
In conclusion, our pilot data indicate that therapy with fumaric acid esters appears to be safe and well tolerated in patients with progressive MS. In more than 75% of our patients no further disease progression was evident. Further studies are urgently needed to evaluate the detailed therapeutic potential of fumarates and their long-term effects in progressive MS.
Footnotes
Funding
This research received no specific grant from any funding agency in the public, commercial, or not-for-profit sectors.
Conflict of interest statement
Katrin Strassburger-Krogias, Gisa Ellrichmann and Peter Altmeyer: no disclosures. Christos Krogias: received travel grants for scientific meetings from Bayer Vital and Bristol-Meyer Squidd. Andrew Chan: personal compensation as a speaker or consultant for Almiral, Bayer Schering, Biogen Idec, Merck Serono, Novartis, Sanofi-Aventis and TEVA. Ralf Gold: personal compensation and grant support from Biogen Idec, Bayer Schering, Novartis, Merck Serono, Sanofi-Genzyme, Roche and TEVA.