
Abstract
Background:
Multiple sclerosis (MS) is an autoimmune demyelinating disorder of the central nervous system (CNS). Despite improvements of immunomodulatory therapies in relapsing–remitting MS, the pathomechanisms of progressive disease are poorly understood and therapeutically addressed to date. A pathophysiological role for proteins encoded by human endogenous retroviruses (HERVs) has been proposed. GNbAC1 is a monoclonal antibody directed against the envelope protein of a HERV with postulated involvement in MS.
Methods:
This review addresses the treatment concept of GNbAC1, the design, preclinical and clinical development of the antibody, as published by November 2018. All four in-human trials (of which two addressed MS) are discussed.
Conclusion:
The treatment concept of GNbAC1 is appealing but remains controversial due to conflicting results regarding the hypothesized underlying pathomechanism. Anticipated immunomodulatory effects were not observed in clinical or pharmacodynamic analyses of the currently available data. However, a magnetic resonance imaging sign compatible with the remyelinating potential of GNbAC1 encouraged further development of this antibody in progressive MS. No relevant issues with tolerability or safety have been described to date.
Keywords
Introduction
Multiple sclerosis (MS) is a demyelinating disorder of the central nervous system (CNS) and the most common nontraumatic cause of disability in young adults in the western hemisphere. 1 The relapsing–remitting form of MS (RRMS) frequently transforms into a chronic secondary-progressive phase (SPMS) with constant worsening affecting motor, autonomic and neurocognitive functions among others.2,3
To date, the treatment of MS with disease-modifying agents generally aims to influence the underlying immune mechanisms and is efficacious in RRMS.4,5 Despite persistent attempts, no neuroregenerative treatment for MS has been approved for clinical routine use. GNbAC1, a monoclonal antibody directed against a human endogenous retrovirus (HERV) envelope protein, was considered a candidate compound in this context. 6
HERVs
HERV biology and functionality
HERVs represent the footprints of ancient retroviral infections in the genome of human germ-line cells. The incorporated genetic retroviral information or its fragments prevail through generations in a Mendelian manner and constitute about 8% of the human genome.7,8 HERV-derived genomic regions include sequences resembling the coding regions of four major proteins forming the envelope (env), the core (gag), the reverse transcriptase (pol) and integrase (pro) of ancestral viruses, and are grouped into 10 families by their primer binding sites (e.g. HERV-K or HERV-W). 9 The ability to produce functional proteins or even a virion is typically lost through accumulated mutations. While being truncated and losing their open reading frame fossilizes most genes, very few retroviral sequences retain a coding function. 9 These expressed fragments can account for evolutionary acquired biological functions like syncytin-1, a primarily placental cell–cell fusion protein, but could potentially also be involved in the pathophysiology of cancer (e.g. breast cancer), neurodegeneration (e.g. amyotrophic lateral sclerosis) or autoimmunity.7,10,11 Such biologically relevant events seem to be very rare or may, in fact, be limited to env proteins of the HERV-W (and hypothetically HERV-K) family8,12 [Figure 1(a)].

HERV biology and treatment concept of GNbAC1.
Potential association with MS
Perron and colleagues first described retroviral particles in the leptomeningeal tissue of MS patients and reported the genome of an endogenous retrofragment they found associated with MS; this retrofragment was hence termed MSRV.13,14 The MSRV sequence suggests that it is a member of the HERV-W family. Its gag, pol and pro regions were soon recognized as noncoding. 13 Intensive research on a putative MSRV-env protein with different techniques and sample types in the era of evolving genome analysis led to often conflicting or incomparable results. 15 Like syncytin-1, MSRV-env and other putative env proteins of similar retrofragments would classify as HERV-W-env. In an analysis of the 26 known HERV-W-env sequences of relevant lengths (>400 nucleotides) most loci were altered by substitutions, frameshifts (compared with syncytin-1) and stop codons. Only syncytin-1 and seven frame-shifted sequences did not contain a stop codon, none of which is concordant with any reported MSRV sequences. 8
A post-mortem study identified a higher expression of HERV-W-env in the brain lesions of MS patients and especially in the microglia and invading lymphocytes. 16 A recent meta-analysis (analyzing the results of DNA, RNA or protein expression) concluded that HERV-W-env is more frequently found in the serum/plasma, cerebrospinal fluid (CSF) and peripheral blood mononuclear cells (PBMCs) from MS patients compared with control populations [with odds ratios ranging from 6.0 (CSF) to 22.7 (serum/plasma)]. 15 The potentially translatable HERV-W-env proteins have similar predicted structures and in early studies could not easily be discriminated (until the introduction of a specialized polymerase chain reaction protocol 17 ), although syncytin-1 differs in several biologically relevant domains from a putative MSRV-env protein. 8 Retrospectively, the interpretation of the observed associations is therefore hampered by the confusion of HERV-W-env proteins due to their gradual discovery and inconsistent measurement. In a human genome-wide association study (GWAS) a HERV-associated locus of the HERV-15 family was associated with MS, but there was no association found for HERV-W-env.8,18
GNbAC1 development
Treatment concept
With respect to reports of the epidemiological associations of MS and HERV-W-env, it was hypothesized that the putative env protein encoded by the MSRV retrofragment is triggering or amplifying pathological processes in MS patients.
In vitro and animal experiments with a reconstructed MSRV-env (after artificial elimination of stop codons) suggested a strong agonist function of this recombinant MSRV-env surface domain on Toll-like receptor 4 (TLR4) and subsequent effects. In vitro MSRV-env could mediate immune activation pathways, hypothetically leading to acute and chronic inflammation in the CNS,19,20 and inhibit oligodendroglial precursor cell differentiation, hypothetically leading to impaired remyelination. 21 These properties potentially account for a pathomechanism in relapsing as well as progressive stages of MS [Figure 1(b)].
GNbAC1 is a monoclonal antibody designed to antagonize the surface domain of the reconstructed MSRV-env protein to inhibit these effects.22,23 The treatment concept anticipates that GNbAC1 will exert anti-inflammatory properties and promote remyelination in treated individuals.
Criticism of treatment concept
This treatment approach of GNbAC1 and the concept of a HERV-associated pathophysiology in MS remain controversial.
Cohorts establishing an association between HERV-W-env and MS were largely analyzed one to two decades ago and used different techniques, while a relevant signal from GWAS data is missing to date.15,18 Various candidate sequences of MSRV genes have been published. None of the previously published sequences potentially coding an MSRV-env protein fully accords with a translatable HERV-W locus. 10 Specifically, the reconstructed MSRV-env protein used to design GNbAC1 (GenBank entry: AF331500.122,23) is not encoded by any known gene in the human genome. The only sequence showing less than 5% discordance (Xq22.3b, 98% concordance) contains a stop codon at position 39 preventing a meaningful translation. 24
It was hypothesized that discrepancies between the identified MSRV-env and the human genome were created by unintended in vitro recombinations between individual HERV transcripts created during reverse transcription (e.g. through template switches of reverse transcriptases) or point mutations. 24 While putative HERV-env proteins could be encoded by eight identified loci, the biological significance of HERV-W-env proteins other than syncytin-1 remains a matter of debate. 8 A low expression of syncytin-1 in the CNS could explain some observations of HERV-W-env-transcripts in MS brains and even correlate with effects on glial cells. 25
Antibody design
Candidate immunoglobulin (Ig)G1 murine antibodies were isolated from mice immunized with one suggested recombinant MSRV-env protein (GenBank entry: AF331500.1). Among these candidates, a prototype antibody was selected by its anti-inflammatory properties in PBMC cell cultures and its capacity to bind to both the ectodomain on the cell surface and the full-length recombinant protein. 23 It might therefore bind to the similar structure of syncytin-1 as well, but not cover the ectodomain of syncytin-1. 8 From this prototype an intermediate chimeric IgG1 and IgG4 immunoglobulin and finally a fully humanized IgG4 version of the antibody, called GNbAC1, was created. 23
Interchain disulfide linkage of the antibody was enhanced by mutations in the core region to tighten interchain binding. It was designed as a full-length antibody of the IgG4/kappa subclass with a molecular weight of 147 kDa. GNbAC1 affinity to recombinant MSRV-env is 2.2 nM 23 and its preserved specificity during the humanization process was determined by both in vitro and in vivo methods. 19
Toxicology
Toxicity of GNbAC1 was studied in a 2-week observation of mice following a single intravenous administration of the antibody at the equivalent dose and the five-fold dose planned for the phase I trial. A thorough analysis of clinical features including ophthalmologic findings, haematological and biochemical blood values and macroscopic post-mortem as well as microscopy did not show any signs of toxicity and only a marginal elevation of leukocyte counts in animals treated with high-dose regimens. 23 Moreover evaluation of antibody-dependent immune cell-mediated cytotoxicity and complement-dependent cytotoxicity in MSRV-env transfected human cells in vitro revealed no cytotoxicity of the IgG4 antibody. 23
Finally, cross-reactivity of GNbAC1 was examined in 42 different human tissues. An antibody-specific signal was detected in a few samples but only at high concentrations. Interestingly, a signal on syncytiotrophoblasts and trophoblasts of the placenta suggests that GNbAC1 binds to syncytin-1. 23 Potential toxic effects in the placenta therefore necessitate a restrictive regimen in fertile women.
Pharmacokinetics
GNbAC1 is administered as an intravenous infusion. The two dose-finding studies in healthy volunteers have been completed. At the examined doses from 0.15 to 36 mg per kg body weight near-linear pharmacokinetics were documented.26,27 Dose-dependent maximal concentrations of 3 to 1018 µg/ml (dose-normalized median Cmax = 18.1 to 30.1 µg/ml) were reached after a few hours (median tmax = 1.50 to 4.06 h). Uptake into the CNS is complicated by the blood–brain barrier (BBB). Thus, effective concentrations are significantly lower in the target tissue. In healthy volunteers the CSF/serum ratio did not exceed 0.5% within 1 month after administration. 27 As an IgG antibody, GNbAC1 is mostly eliminated via intracellular catabolism 28 with a half-life of approximately 1 month in the terminal phase (median t½ = 452 to 620 h). Detailed pharmacokinetics are listed in Table 1.
Pharmacokinetic parameters by dose group after a single GNbAC1 administration in two phase I trials: values are geometric means (% coefficient of variation).
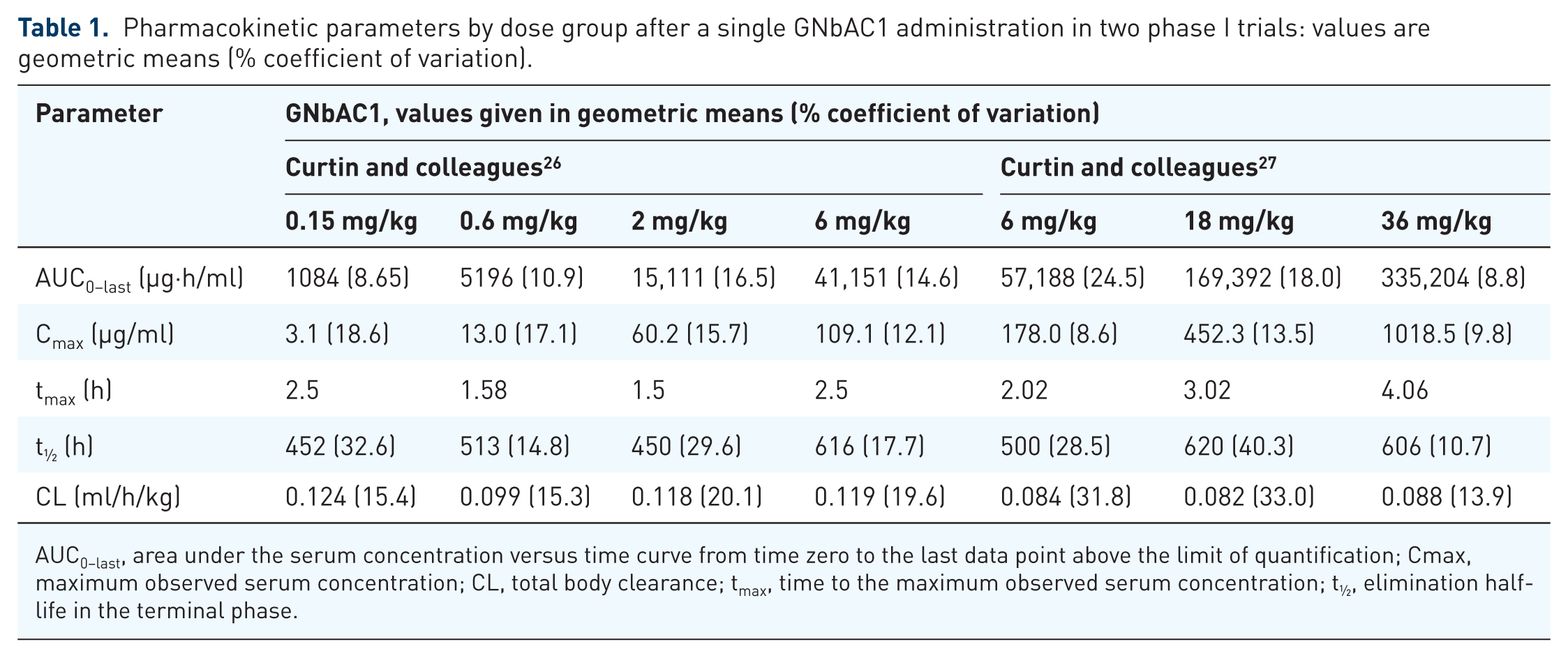
AUC0–last, area under the serum concentration versus time curve from time zero to the last data point above the limit of quantification; Cmax, maximum observed serum concentration; CL, total body clearance; tmax, time to the maximum observed serum concentration; t½, elimination half-life in the terminal phase.
Pharmacodynamics
Considering the limited number of patients treated in the published phase IIa trial, pharmacodynamic data are limited. There were two publications that analyzed the parameters of the 10 patients treated with GNbAC1 in this trial. Compared with the baseline, no statistically significant treatment effects were observed for the proportions of various immune cell populations, for proinflammatory cytokines, for in vitro interferon-γ production in response to antigens, nor for p38 mitogen-activated protein kinase phosphorylation in monocytes as a marker of TLR4-stimulation.29,30 All of these findings suggest no significant impact on TLR4 signalling by GNbAC1.
RNA transcript numbers of both the putative MSRV-env and MSRV-pol were found to decrease in PBMCs with recurrent GNbAC1 administrations in this small cohort. A conclusive mechanistic explanation for this effect is lacking as well as an affirmation from greater patient numbers. 29
Clinical efficacy
Two studies in MS patients have been conducted to date29,31,32 (see Table 2). Due to small patient numbers, conclusions regarding the clinical response from the first trial (classified phase IIa) are limited. In this study, only one treated patient presented with disease activity, as identified by a new MS-specific lesion on magnetic resonance imaging (MRI) after 12 weeks. 29 No other clinical markers of efficacy were specifically analyzed.
Summary of in-human trials of GNbAC1.
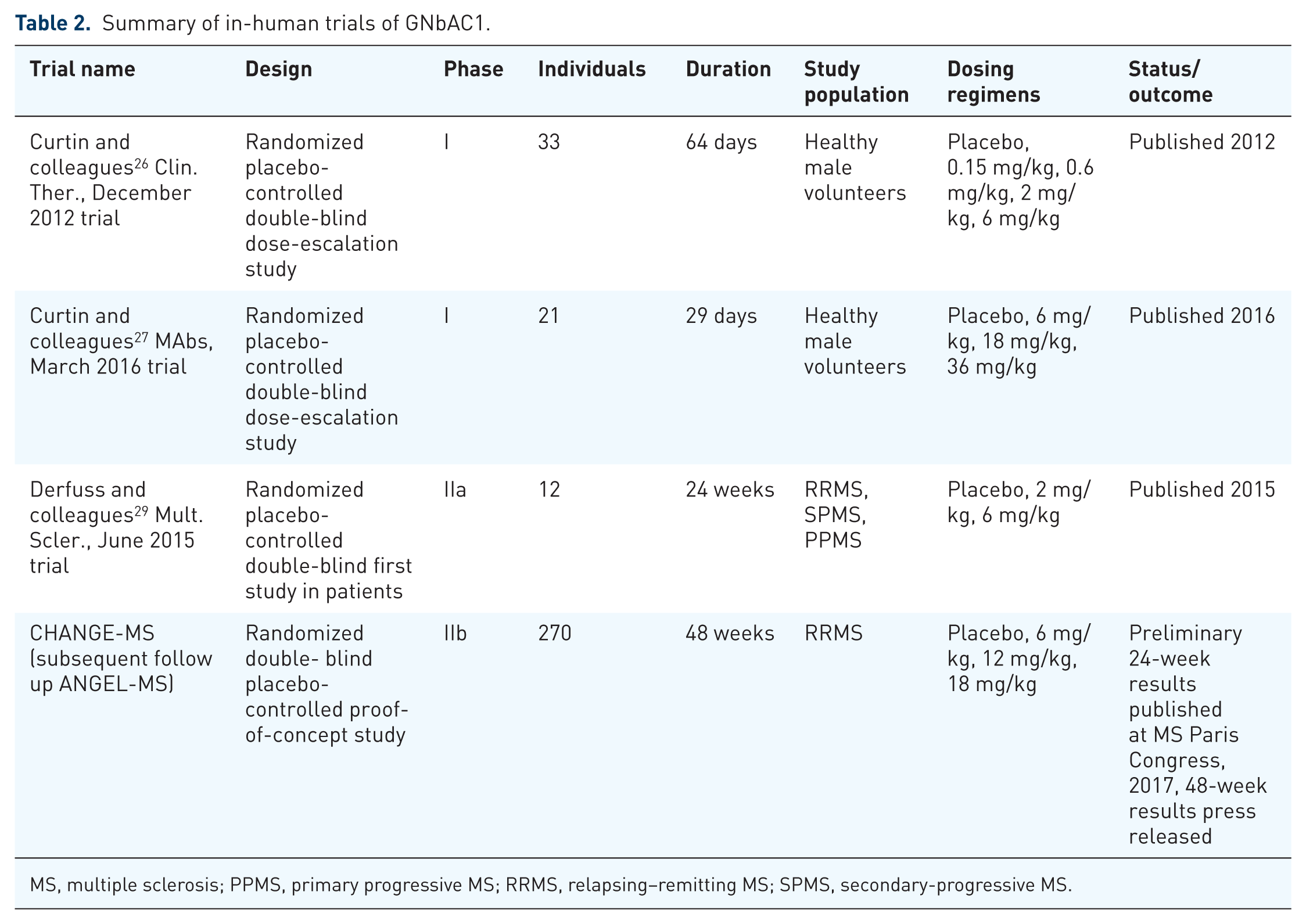
MS, multiple sclerosis; PPMS, primary progressive MS; RRMS, relapsing–remitting MS; SPMS, secondary-progressive MS.
A phase IIb study in patients with RRMS (CHANGE-MS (ClinicalTrials.gov Identifier: NCT02782858)) was conducted for a 24-week period in a placebo-controlled design. After this period placebo-treated patients were re-randomized to three verum dose groups and treated for another 24 weeks. 32 270 patients, randomized equally to four treatment arms, were treated with placebo or GNbAC1 (at doses of 6 mg/kg, 12 mg/kg or 18 mg/kg) every 4 weeks. The primary endpoint and secondary endpoints were predefined and focussed on established MRI markers of inflammatory activity and brain atrophy. Neither a significant change in contrast medium-enhancing lesions in MRI (primary endpoint), clinically apparent relapses, nor brain volume loss was observed in the GNbAC1-treated cohorts (secondary endpoints). 32 A series of predefined analyses of this trial were performed in addition. In patients with active lesions, a significant reduction in new contrast medium-enhancing lesions was reported for the highest dose of GNbAC1 (18 mg/kg) versus placebo at one time point in the 24-week follow up. 33 Furthermore, the magnetization transfer ratio (MTR) was analyzed as a marker of remyelination in cerebral normal-appearing white matter and cortical regions. MTR is a specially developed MRI technique depicting the density of macromolecules in the brain parenchyma by comparing off-resonance pulsed and unpulsed images. It has been proposed as an indicator of myelination in cerebral tissue not directly affected by inflammatory lesions.34,35 While patients receiving placebo experienced median decreases in MTR of 0.5–0.7% units over the course of 24 weeks, a median increase of 0.2–0.3 was described in the patient group receiving high doses of GNbAC1 treatment. 32 No significant results were obtained for treatment with 6 mg/kg or 12 mg/kg.
After 12 months of treatment, reductions in cortical and thalamic atrophy of 31% and 72% respectively were seen in the highest dose of 18 mg/kg compared with the control group, defined as patients originally randomized to placebo before being re-randomized to active therapy for the second period of 6 months (p = 0.045 and p = 0.014 respectively; Spearman’s rank correlation coefficient). Whole brain atrophy showed a nonsignificant 29% relative reduction in brain volume loss over 12 months for the highest dose versus the control group (p = 0.079). The number of T1 hypointense lesions was reduced by 63% (p = 0.014) at the end of the study in the 18 mg/kg versus control group. T1 hypointense lesions, also known as black holes, are considered as a marker of permanent tissue destruction in the brain. 36 The benefit in the MTR signal of 18 mg/kg relative to the placebo that was seen at 6 months remained stable over the second period of the trial. For MRI measures of neuroinflammation there was no significant separation between treatment groups over the 12-month treatment period. The trend seen in post hoc analyses at 6 months on neuroinflammatory markers (see above) did not translate into a relevant clinical or imaging result at 12 months. Currently, a long-term extension to CHANGE-MS evaluating the long-term safety and efficacy of GNbAC1 for 96 weeks is ongoing (ANGEL-MS). 36
Publication of data from the extended trial is awaited.
Safety and tolerability
The administration of GNbAC1 was generally well tolerated in patients and healthy volunteers. Studies in healthy individuals and MS patients revealed no serious or severe adverse effects and no changes in vital signs, laboratory findings or electrocardiogram data.26,27,29,32 Of note, no specific infusion-related adverse events or signs of immunogenicity were reported in these studies.
Development for different indications
In addition to MS, GNbAC1 is also being tested in a phase IIa trial in 60 patients with type1 diabetes 37 . Results from this trial are pending. GNbAC1 has received an orphan drug designation from the United States Food and Drug Administration in chronic inflammatory demyelinating polyneuropathy (CIDP). Currently there is no trial of GNbAC1 in CIDP listed on clinicaltrials.gov.
Conclusion
Despite tremendous efforts and unwaning attention, the pathophysiology and the treatment of the progressive aspect of MS still waits for a breakthrough. While it appears realistic that most currently investigated agents will not perform encouragingly in a clinical setting, a singular success can promote new understanding of the underlying pathophysiological processes. As a monoclonal humanized IgG4 antibody directed against a hypothetically pathogenic HERV-W-env protein, GNbAC1 represents a novel treatment approach for this unmet need.
The concept of MS being a HERV-triggered or HERV-mediated disorder remains controversial. Conflicting results in the era of evolving techniques in genetics created a confusing picture of possible associations based on relatively small epidemiological studies.
It is now established that HERVs do not form virions and that most of their genetic information is fossilized in retrofragments without the ability to be translated into proteins. While some HERV-W-env sequences are known or hypothesized to produce proteins (e.g. syncytin-1), the existence and origin of MSRV-env remains a matter of debate. It also remains controversial whether the apparent TLR4-mediated effects observed in vitro have a pathologically relevant counterpart in vivo. Since GNbAC1 was designed to bind not only the ectodomain of recombinant MSRV-env, but also full-length HERV-W-env, effects on other similar proteins are conceivable.
The discussed studies revealed no clear immunomodulatory effects in imaging and clinical data nor effects on immune markers. These results do not support the use of this antibody as a prophylactic treatment for the inflammatory component of MS. Despite these frustrating results on classical parameters, the positive outcome on MTR as a marker of possible remyelination and brain atrophy raised awareness of possible neuroprotective effects. It is a widely discussed perception that the detection of an efficacious treatment for neuroregeneration and progressive aspects of MS may depend on different endpoints and longer timeframes compared with inflammatory aspects. Considering these premises, eventual future trials with progressive MS patients will have to show similar paraclinical effects, but more importantly also a reduced worsening of neurological symptoms.
Summary and outlook
In summary, the development of GNbAC1 represents an experiment to translate a novel pathophysiological concept into a clinical treatment. It is currently investigated as a potentially remyelinating agent, after no signal of immunomodulatory activity was detected. Its development involves substantial challenges, not least being a demonstration of clinical efficacy in a progressive MS population.
The interpretation of preclinical data is hampered by the difficulty of testing the pathogenicity of HERV-W-env in mice since it is a human endogenous retrovirus that is not present in the genome of rodents. It is therefore even more important to stringently test an association of HERV-W-env with MS in humans. So far, these association studies used different analytic tools, were unblinded and were carried out in rather small cohorts. To finally prove an association, a blinded analysis of a large multicentre cohort of paired serum/CSF samples with a validated assay has to be performed. Also, neuropathological and biological studies will need to robustly clarify the specific role and source of HERV proteins in the CNS.
For further clinical development, a progressive or a relapsing MS population with a concomitant anti-inflammatory treatment could be targeted. To see the possible neuroprotective/remyelinating effects of GNbAC1 several biomarker endpoints would have to be included in addition to the established clinical endpoints (e.g. the expanded disability status scale, MS functional composite, symbol digit modalities test). 38 Obviously, nonconventional MRI sequences could give an indication of the remyelination potential.34,35 This could be further corroborated by positron emission tomography imaging. 39 The analysis of neurofilament light chains in the serum could give an indication of axonal protection. 40 Finally, motor, sensory and visual evoked potentials could make the translation between pure biomarker and functional outcomes. 3 If HERV-W-env protein can be reliably detected in the serum or CSF this could also be used as a potential patient stratification marker for treatment responses. If GNbAC1 were to prove efficacious in MS, it would substantially strengthen the idea that endogenous retroviral sequences in our genome are involved in MS and maybe in other diseases as well. This could open a new area of treatment possibilities. However, to date, substantiated evidence for this treatment concept is lacking.
Highlights
Proteins encoded by HERVs are discussed as components in the pathophysiology of MS.
GNbAC1 is a monoclonal antibody directed against the envelope protein of the HERV-W family.
Pharmacodynamic and imaging data do not reveal any immunomodulatory effects of GNbAC1.
MRI changes during a phase IIb study with GNbAC1 are compatible with remyelination.
No issues of safety or tolerability of this antibody were identified in the studies published to date.
Footnotes
Funding
This research received no specific grant from any funding agency in the public, commercial, or not-for-profit sectors.
Conflict of interest statement
Martin Diebold received grants from the University of Basel and speaker honoraria from Biogen Switzerland, used exclusively for research purposes. Tobias Derfuss serves on scientific advisory boards for Novartis Pharma, Merck, Biogen, Genzyme, GeNeuro, Mitsubishi Pharma, and Celgene; has received funding for travel or speaker honoraria from Biogen, Genzyme, Novartis, and Merck, and receives research support from Biogen, Novartis Pharma, the European Union (ABIRISK project under grant agreement no. 115303), the Swiss National Foundation and the Swiss MS Society. He was the principal investigator of the phase IIa trial of GNbAC1 and is a member of the steering committee of the phase IIb trial of GNbAC1.