
Abstract
Background:
VEST was a multi-centre study of real-world use of vedolizumab in inflammatory bowel disease (IBD) in routine practice in the United Kingdom.
Objectives:
To describe real-world indications, effectiveness, patient-reported outcomes and safety.
Design:
Prospective observational cohort study at 22 centres.
Methods:
Patients receiving vedolizumab as part of standard care were included. Data were collected at infusion visits for activity indices (Harvey–Bradshaw Index (HBI) or partial Mayo Score (PMS)), physician global assessment (PGA), patient-reported quality-of-life and treatment perception (IBD-Control Questionnaire) and adverse events. Clinical response (Wk14) was defined as a reduction in HBI ⩾3 or PMS ⩾2, clinical remission as HBI ⩽4 or PMS ⩽1 and analysed using non-responder imputation. One-year persistence was defined as continuing on vedolizumab after an infusion at ⩾48 weeks. Biomarker and endoscopic data were not available.
Results:
364 patients, mean age: 48 years; 132 (36%) with Crohn’s disease (CD), 224 (62%) with UC and 8 (2%) with IBD-U; 174 (48%) male; 142 (39%) receiving steroids at baseline (Wk0); 141 (39%) bio-naïve. At baseline, 279 (77%) had “active” disease. One-year persistence: 58% overall (54% for active disease). Among persistent cases (n = 212), median (IQR) IBD-Control-8 scores improved from 6 (3–10) at baseline to 14 (10–16) at post-induction (Wk14) and 1 year (p < 0.001 vs baseline). Corresponding scores for IBD-Control-VAS were: 50 (30–70), 80 (65–90) and 85 (70–95), respectively (p < 0.001 vs baseline). Each domain of IBD-Control-8 showed improvement. Baseline and post-induction health status (activity index, PGA or IBD-Control) were associated with 1-year persistence, but no significant associations were observed for disease type, duration, bio-naïve status or baseline steroids. Of those with active disease at Wk0, clinical remission rates were 29%, 30% and 38% for CD, UC and IBD-U, respectively, and steroid-free remission rates were 26%, 27% and 38%. Similar remission rates were observed at 1 year. Possible adverse events leading to treatment cessation were rare (3%).
Conclusion:
In routine clinical practice in the UK, vedolizumab demonstrated high levels of persistence. Similar rates of clinical response, remission and 1-year persistence were seen in UC and CD patients, and in bio-experienced versus naïve cases. Persistent cases experienced significant and sustained improvements in quality of life and treatment perception. Persistence does not imply anti-inflammatory efficacy, as biomarker data were not available.
Plain language summary
This study (VEST) looked at how vedolizumab (a gut-selective biological treatment for inflammatory bowel disease (IBD)) works in everyday NHS practice across 22 UK hospitals. Unlike clinical trials, which have strict entry criteria, this study included all adults who started vedolizumab as part of routine care, including older patients, those usually excluded from trials and people with less severe disease.
A total of 364 people took part: 224 with ulcerative colitis, 132 with Crohn’s disease, and 8 with IBD unclassified. Most had active symptoms when treatment began, and many had already tried other biological drugs. The main measure was “persistence,” meaning whether patients were still receiving vedolizumab one year later. Overall, 58% continued treatment (54% of those with active symptoms). Persistence rates were similar for Crohn’s disease and ulcerative colitis, and for people who were new to biologics versus those who had used them before.
Among patients who remained on vedolizumab, symptoms and quality-of-life improved. By week 14, more patients were in clinical remission, using fewer steroids, and reporting better control of their condition. These findings were maintained at one year. Patient-reported outcomes “covering pain, sleep disturbance, fatigue, mood, and impact on daily activities” showed improvement across all areas. People with more severe symptoms at the start were less likely to stay on the drug, while better patient-reported control scores early in treatment predicted continuation. Vedolizumab was well tolerated. Possible drug-related side effects were uncommon (only 3% of patients stopped because of adverse events).
In summary, this real-world UK study shows that vedolizumab was safe and is used across diverse patient groups with meaningful, lasting improvements observed in those remaining on treatment
Keywords
Introduction
The two main forms of inflammatory bowel disease (IBD) are Crohn’s disease (CD) and ulcerative colitis (UC), with a minority having an unspecified form of colitis (IBD-U). These chronic conditions share many common features and treatments. The development of anti–tumour necrosis factor (TNF)-α agents provided a revolution in the management of IBD. Nevertheless, this drug class is not without potential for serious adverse effects (e.g. infection, malignancy risk) and a significant proportion of patients fail to respond, lose response or develop intolerable side effects. 1 This stimulated the development of biological agents with alternative modes of action. Vedolizumab is a selective humanized immunoglobulin G1 monoclonal antibody to α4β7 integrin that modulates gut lymphocyte trafficking. It was shown to be effective and safe in placebo-controlled trials2–4 and was approved in the UK for use in moderate-to-severe CD and UC during 2015.5,6
Subsequent observational studies have shown comparable effectiveness and safety in clinical practice. 7 However, by design, such cohort studies have typically focused on patients with baseline inclusion criteria comparable to the pivotal trials and reported comparable clinical, laboratory and/or endoscopic end-points. In routine practice, prescribing often extends to patient groups that would have been ineligible for trials or actively excluded. Moreover, traditional objective clinical endpoints may not fully capture the impact of a treatment on patients’ daily lives. As a result, observational data are sparse for patient-centred outcomes such as quality of life, patient-perceived disease control and treatment perception among unselected cohorts who receive vedolizumab in routine settings.
We report a prospective, multi-centre study of real-world experience of vedolizumab in the UK, which focused on these knowledge gaps. Our aim was to describe the baseline profile and subsequent outcomes of unselected patients treated with vedolizumab. In particular, we sought to quantify the benefits realized in UK practice among patients who continued treatment.
Materials and methods
Study design and setting
The VEST study was a prospective, multi-centre observational cohort study of adult patients (age 18 years or older) who commenced vedolizumab for treatment of IBD. Consent was obtained from patients initiating vedolizumab between February 2017 and December 2019, with a confirmed clinical, endoscopic, or histological diagnosis of CD, UC or IBD-U. Baseline characteristics were recorded and outcomes collected prospectively using a standardized IBD-specific electronic database (UK IBD Registry WebTool). Data were recorded at each infusion visit (weeks 0, 2, 6, 14, 22, 30, 38, 46 and 54) and at any ad hoc review visits. All patients who received at least one dose of vedolizumab were included in the cohort and were followed up until cessation of treatment or reaching 1 year of drug persistence. Lack of study persistence (i.e. missing follow-up) was assumed to indicate treatment failure (i.e. non-responder imputation, NRI).
Intervention
Patients received vedolizumab according to the standard UK dosing regimen for IBD. Under this protocol, 300 mg of vedolizumab is administered via intravenous infusion over 30 min. Induction doses were administered at 0, 2 and 6 weeks, with standard maintenance intravenous dosing at 8-week intervals thereafter. Concomitant medications, prior treatment exposure and changes to the vedolizumab maintenance schedule (i.e. dose escalation) were recorded. Dose escalation of vedolizumab was at the discretion of the treating physician teams.
Outcomes
Baseline patient and disease characteristics were recorded, and the main study outcomes were analysed statistically at week 14 and 1 year. To allow for variation in the timing of infusion visits and changes to the regimen, the 1-year outcomes were based on the last recorded measure at least 48 weeks from drug start.
Drug persistence
The primary outcome was treatment persistence at 1 year, defined as the continuation of scheduled maintenance treatment beyond any recorded infusion visit ⩾48 weeks from baseline. Data were collected for clinician- and patient-reported outcomes at each infusion visit.
Clinician-reported outcomes
Traditional clinical disease activity was assessed using the Harvey–Bradshaw Index (HBI) for CD 8 or the partial Mayo score (PMS) for UC. 9 Active CD was defined as HBI score ⩾5 (based on symptoms for the previous day), and active UC or IBD-U as PMS⩾2 (based on symptoms over the last 3 days). Relevant binary outcomes were clinical response (among those with active disease at baseline), remission and steroid-free remission. Response was defined as a reduction in HBI of ⩾3 points, or a reduction in PMS ⩾2 points (plus an absolute rectal bleeding score ⩽1). Steroid-free refers to patients who were not taking oral glucocorticoids at the time of assessment (prednisolone or budesonide). Activity scores were further categorized by severity based on published cut-offs (PMS: Remission ⩽1; Mild 2–4; Moderate 5–6; Severe 7–9; HBI: Remission < 5; Mild 5–7; Moderate 8–16; Severe > 16). Clinical teams were also asked to record their overall (global) rating of IBD activity at each visit, categorized as remission, mild, moderate or severe (Physician’s Global Assessment, PGA).
Patient-reported outcomes
Patient-reported outcomes were collected using the IBD-Control Questionnaire, which measures patient-perceived disease control over the last 2 weeks. 10 The instrument includes an eight-item scale (IBD-Control-8), covering health-related QoL (physical, social and psychological) and treatment satisfaction.10–12 Each question has three response options (Yes, No and Not sure), with zero points assigned to the most negative response (i.e. the relevant concern or impairment is present), one point to the neutral response (i.e. not sure) and two points for the most positive response (i.e. the impairment is absent). The IBD-Control-8 score ranges from zero to 16, with higher scores indicating better control. The questionnaire also includes a visual analogue scale for overall control, the IBD-Control-VAS, with scores ranging from zero (worst) to 100 (best).
Laboratory values
Data on stool biomarkers, endoscopic or radiological assessments were not available.
Adverse events
At each visit, clinicians were asked to enquire about possible side effects or adverse events (AEs) and to categorize as: Infusion reactions, infections (grouped as Upper Respiratory Tract (URTI), Lower Respiratory Tract (LRTI) or any other (Infections, Other)), headaches, skin rashes, arthralgia, breathlessness or other potential AEs related to vedolizumab. AEs were graded as serious if they resulted in discontinuation of vedolizumab.
Statistical methods
Descriptive statistics are provided to summarize demographic and clinical characteristics. Cessation of vedolizumab or loss of study follow-up prior to the 1-year assessment was considered a treatment failure (non-responder imputation, NRI), with time-to-event for drug persistence based on last-recorded visit or verified drug stop date. After completing the study, sites were asked to verify any missing stop dates, thereby validating drug persistence. Patients were censored following their last-recorded visit ⩾48 weeks from drug start. Analyses of clinical response and remission were based on a denominator of all cases with active disease at baseline (NRI analysis). Pre-treatment and post-treatment continuous variables are compared using parametric or non-parametric statistics as appropriate (t-test or Mann–Whitney U, ANOVA or Kruskal–Wallis Test). A two-sided p value of 0.05 was considered statistically significant. Drug persistence was compared between relevant strata using Kaplan–Meier survival analysis and log-rank test. Outcomes were analysed against clinical characteristics to identify prognostic factors, focusing on IBD subtype, disease duration, bio-naïve status, steroid intake and measures of health status. Associations with binary outcomes were explored using logistic regression in exploratory analyses (i.e. not formally pre-specified). Sensitivity analyses restricted these models to the cohort with clinically “active” disease at baseline. All analyses were performed using R. The study is reported in accordance with STROBE guidelines. 13
Results
Baseline patient characteristics
Baseline characteristics of 364 patients from 22 UK centres, which form the overall cohort, are shown in Table 1, which included 132 with CD, 224 with UC and eight with IBD-U. The overall mean age was 48 years (range: 18–98 years) with those aged ⩾65 years accounting for one in four cases (24%, n = 87). Fifty-two percent were female. Of those patients with UC, 8% (n = 17) had proctitis only. Of those with CD, 27% (n = 36) had no colonic involvement. Twenty-two percent of patients with CD (n = 29) had perianal disease. There were 16 patients with a history of prior surgery resulting in the presence of a stoma at the time of vedolizumab initiation. Mean disease duration was 10 years (range: 0–58 years), with 28% being less than 3 years from their original IBD diagnosis.
Baseline demographic and clinical characteristics of 364 patients treated with vedolizumab.
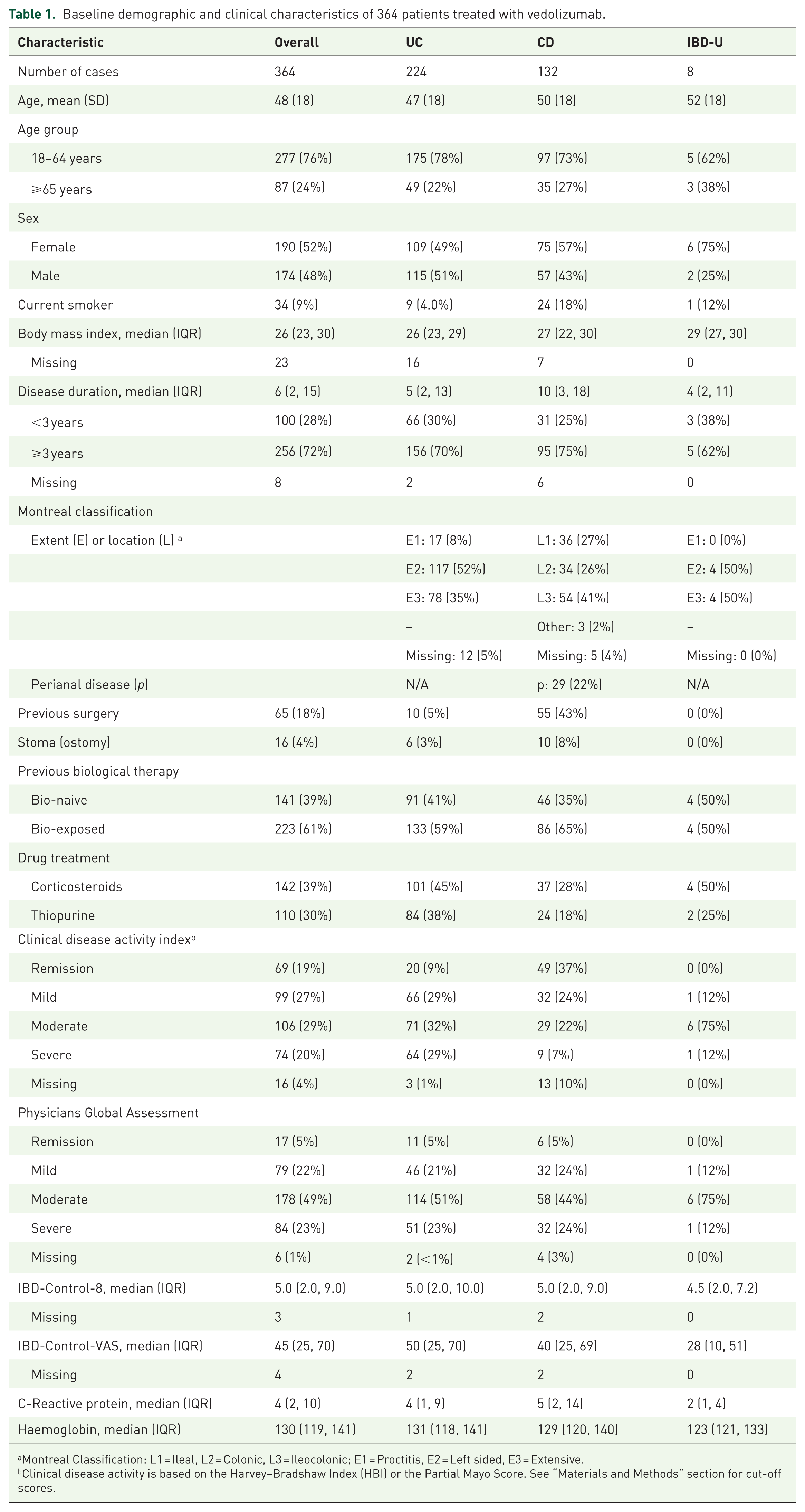
Montreal Classification: L1 = Ileal, L2 = Colonic, L3 = Ileocolonic; E1 = Proctitis, E2 = Left sided, E3 = Extensive.
Clinical disease activity is based on the Harvey–Bradshaw Index (HBI) or the Partial Mayo Score. See “Materials and Methods” section for cut-off scores.
Overall, 39% were receiving corticosteroids at baseline, 30% a thiopurine and 5% another type of immunosuppressant (methotrexate, tacrolimus or ciclosporin). Baseline steroid intake was more prevalent in UC than CD in this cohort (45% vs 28%, p < 0.05). Of the total, 61% had a record of previous biologic exposure (CD: 65%; UC: 59%; IBD-U: 50%) and 39% were bio-naïve. Of the bio-naïve cases, 41% were ⩾65 years of age compared with just 13% of those with a history of prior biologic treatment (p < 0.001). Recorded indications for choosing vedolizumab as first-line biologic were a history of prior malignancy (16%), perceived risk of opportunistic infections (11%), future malignancy (9.2%) or being at high risk for systemic immunomodulation (9.2%), patient preference (9.2%), primary sclerosing cholangitis (1.4%) with no specified reason recorded in the remainder (44%).
Clinician and patient-reported outcomes at baseline
Of the 364 cases treated with vedolizumab, 77% (n = 279) were classified at their first infusion visit as having active disease based on traditional disease activity indices (53% of CD; 90% of UC; 100% of IBD-U; Table 1). The PMS or HBI scores were in the moderate or severe range in 50% (n = 180) of the total cohort (29% of CD; 60% of UC; 87% of IBD-U; p < 0.05). However, based on the treating clinician’s overall global rating (PGA), 94% (n = 341) were judged to have active disease (92% of CD; 94% of UC cases; 100% of IBD-U; p > 0.05 (NS)) with 72% (n = 262) being classified as moderate or severe (68% of CD; 74% of UC cases; 100% of IBD-U; p > 0.05 (NS)).
The median baseline score for IBD-Control-8 for the whole cohort was 5 points (IQR: 2–9), with only 43 cases (12%) reporting a score in the “quiescent” range (⩾13 points). 10 The corresponding median baseline score for IBD-Control-VAS was 45 (IQR: 25–70), with only 38 cases (10%) in the quiescent range (⩾85 points). There were no significant differences in median baseline IBD-Control scores between those with CD, UC or IBD-U, nor in the proportions of patients having scores in quiescent ranges, indicating comparable levels of patient-perceived disease control across the IBD subtypes among this cohort.
Comparison of cohort characteristics against eligibility criteria for original GEMINI RCTs
Within the limits of available baseline patient-level data, we determined whether there was evidence of ineligibility for the original GEMINI trials programme.2,3 Thirteen patients (3.6%) were over the age of 80 years, 17 (4.7%) had proctitis only, 16 (4.4%) had a stoma and 69 (19%) had inactive disease at first infusion visit based on activity index at that point. Based on these four criteria alone, a total of 108 (30%) of those treated with vedolizumab would have been ineligible due to one or more trial exclusions.
Treatment persistence at 1 year
Of the 364 patients started on vedolizumab, 88% (n = 319) persisted with treatment beyond week 14 (i.e. received at least one maintenance infusion) and 58% (n = 212) remained on treatment at 1 year. Drug discontinuation accounted for study non-persistence (i.e. none of the cohort left the study but remained on vedolizumab). There was no significant difference in 1-year drug persistence by diagnosis (CD: 56% (n = 74): UC: 59% (n = 133); IBD-U: 62% (n = 5); p = 0.8).
Among the subgroup of 279 cases with baseline disease activity index in the active range, 54% (n = 152) persisted on treatment at 1 year (CD: 46% (n = 32): UC: 57% (n = 128); IBD-U: 62% (n = 5); p = 0.2), of whom 12% had treatment escalation. Of the 69 cases who had an HBI or PMS score in the remission range at induction, 71% (n = 49) remained on vedolizumab at 1 year (CD: 67% (n = 33); UC: 80% (n = 16); p = 0.3) – significantly more than those with active disease.
Overall, there were 44 patients (9% of total cohort) with escalated vedolizumab dosing during the 1-year observation period (CD, n = 7; UC, n = 34; IBDU, n = 3), of which 22 (50%) remained persistent at 1 year (CD, n = 4; UC, n = 17; IBDU, n = 1). These 22 cases represented 10% of the 212 patients continuing on treatment. Of the 33 cases with active disease at baseline who underwent escalation of treatment (CD, n = 1; UC, n = 30; IBDU, n = 3), 15 (46%) remained persistent at 1 year (CD, n = 1; UC, n = 13; IBDU, n = 1) (Figure 1).
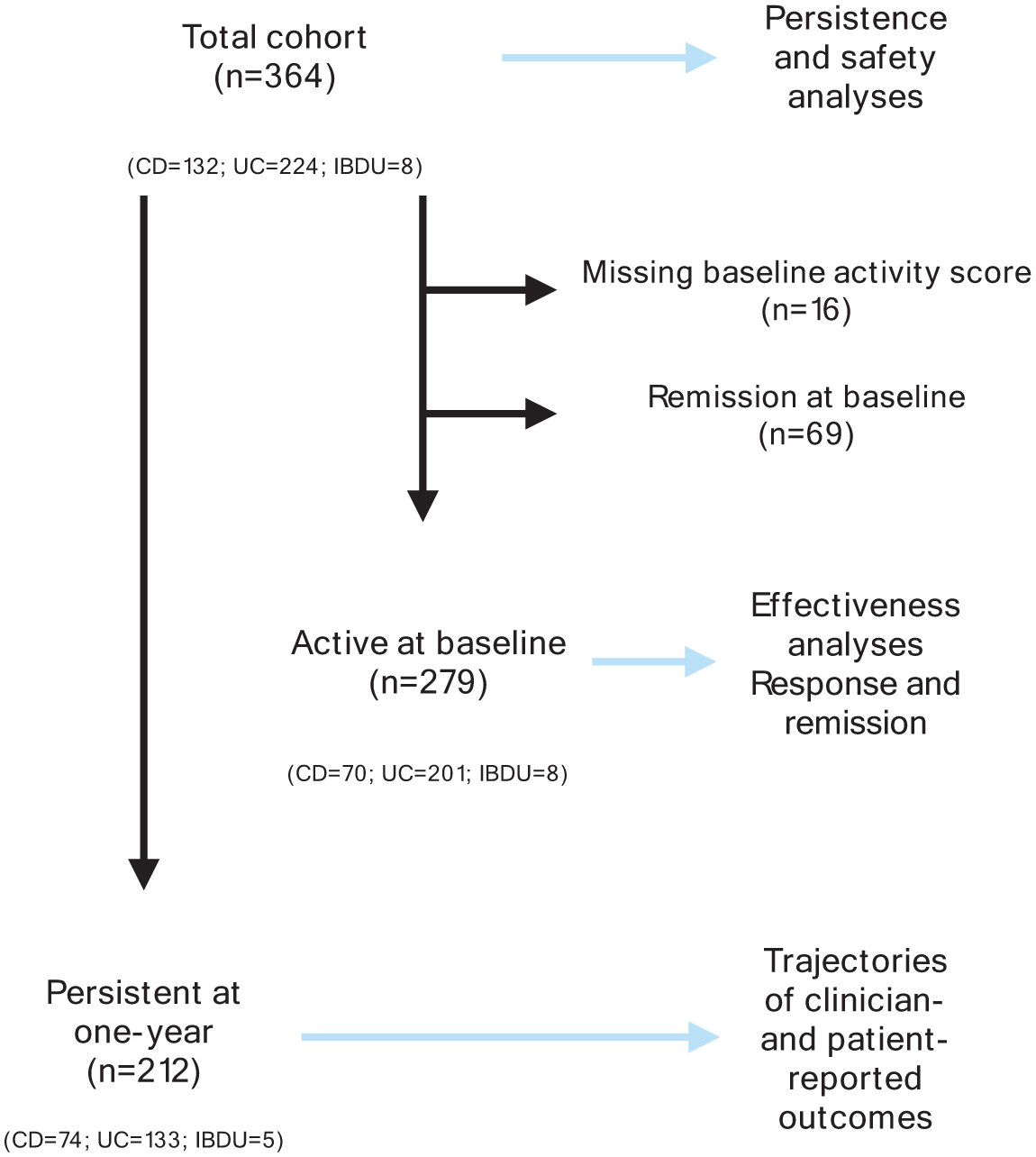
Flow diagram for the VEST study.
We examined persistence among sub-groups of patients typically excluded from clinical trials. Thirteen patients in the cohort were older than 80 years (CD, n = 5; UC, n = 7), of whom 8 (62%) remained persistent at 1-year overall. This included six of seven (86%) of older patients with active disease at the time of the first dose of vedolizumab. There were 17 patients with ulcerative proctitis included in the study, of whom 16 (94%) had clinically active disease at baseline. 1-year persistence was observed in 13 proctitis cases overall (77%), and 12 (75%) of those with active disease at baseline. The cohort also included 16 patients with a stoma (CD, n = 10; UC, n = 6), with 11 (69%) of cases remaining on treatment at 1 year.
We also examined persistence among CD cases stratified according to the presence (n = 29) or absence (n = 103) of perianal disease, finding significantly lower 1-year persistence in the former group (11 (38%) vs 63 (61%), p < 0.01). Fistula-specific outcomes were not reported.
Trajectories of health status measures among persistent patients
The changing profiles of clinician-reported outcomes among the 212 patients who remained on vedolizumab throughout the year of observation are shown in Figure 2.
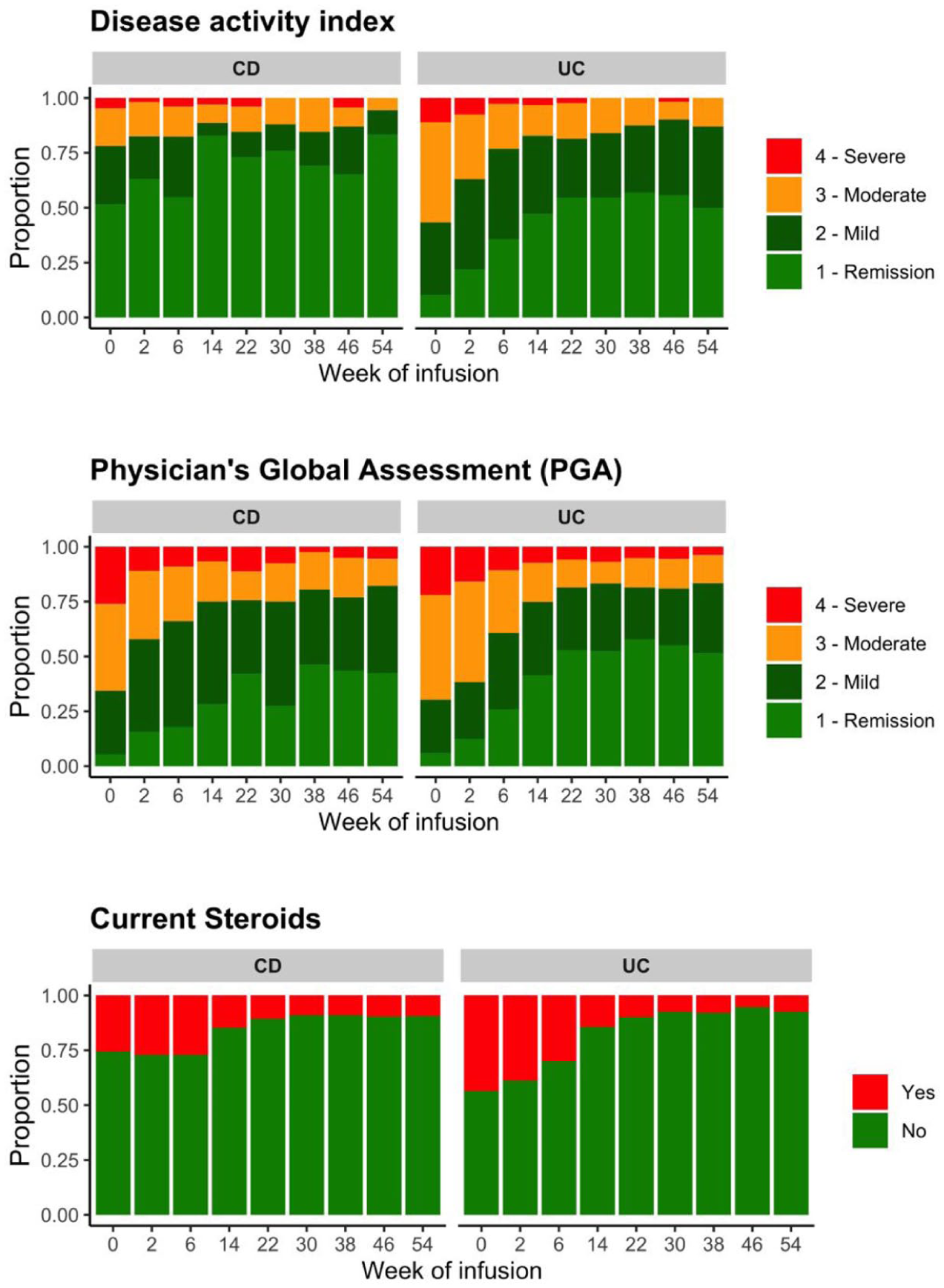
Trajectories of clinician-reported health status measures in 212 patients who remained on vedolizumab at 1 year. (Upper Panel) Clinical disease activity based on the Harvey–Bradshaw Index for Crohn’s disease (CD) or the Partial Mayo Score for ulcerative colitis (UC). Compared to baseline (Week 0), there was a significant increase in proportions of patients categorized as “remission” by Week 14 and at 1 year (p < 0.05 in all cases). (Middle Panel) Distribution of Physician’s Global Assessment (PGA) rating. By Week 14, the proportion of patients classified as “remission” was significantly increased and remained so throughout the 1-year period (p < 0.001). (Lower Panel) Current steroid therapy. Rates of concomitant steroids declined significantly by Week 14 and remained below 10% throughout the remaining observation period.
For those with CD, the proportion of persistent cases in clinical remission (HBI ⩽ 4) increased from 52% at baseline to 83% at post-induction (Week 14) (p < 0.01 vs baseline) and 83% at 1 year (p < 0.01 vs baseline). Corresponding proportions for PGA-based remission for CD were 6% at baseline, 28% at post-induction (p < 0.001 vs baseline) and 42% at 1-year (p < 0.001 vs baseline). Rates of steroid use declined from 26% to 15% (p = NS) and 10% (p = 0.02), respectively.
For those with UC who continued to receive vedolizumab, respective remission rates (PMS⩽1) increased from 10% at baseline to 47% at post-induction (p < 0.001 vs baseline) and 50% at 1 year (p < 0.001 vs baseline). Based on PGA-remission, corresponding rates increased from 6% at baseline, 41% at post-induction (p < 0.001 vs baseline) and 52% at 1-year (p < 0.001 vs baseline). Steroid use declined significantly over the year from 44% to 14% (p < 0.001) and 8% (p < 0.001), respectively.
Patient-reported outcomes demonstrated significant and sustained improvement among those who remained on treatment (Figures 3 and 4). Median IBD-Control-8 scores increased from 6 (IQR: 3–10) at baseline to 14 (10–16) at post-induction (p < 0.001) and 14 (10–16) at 1 year (p < 0.001), (Figure 3). Similarly, median IBD-Control-VAS scores improved significantly in persistent cases from 50 (30–70) at baseline to 80 (65–90) and 80 (70–95), respectively (Figure 3).
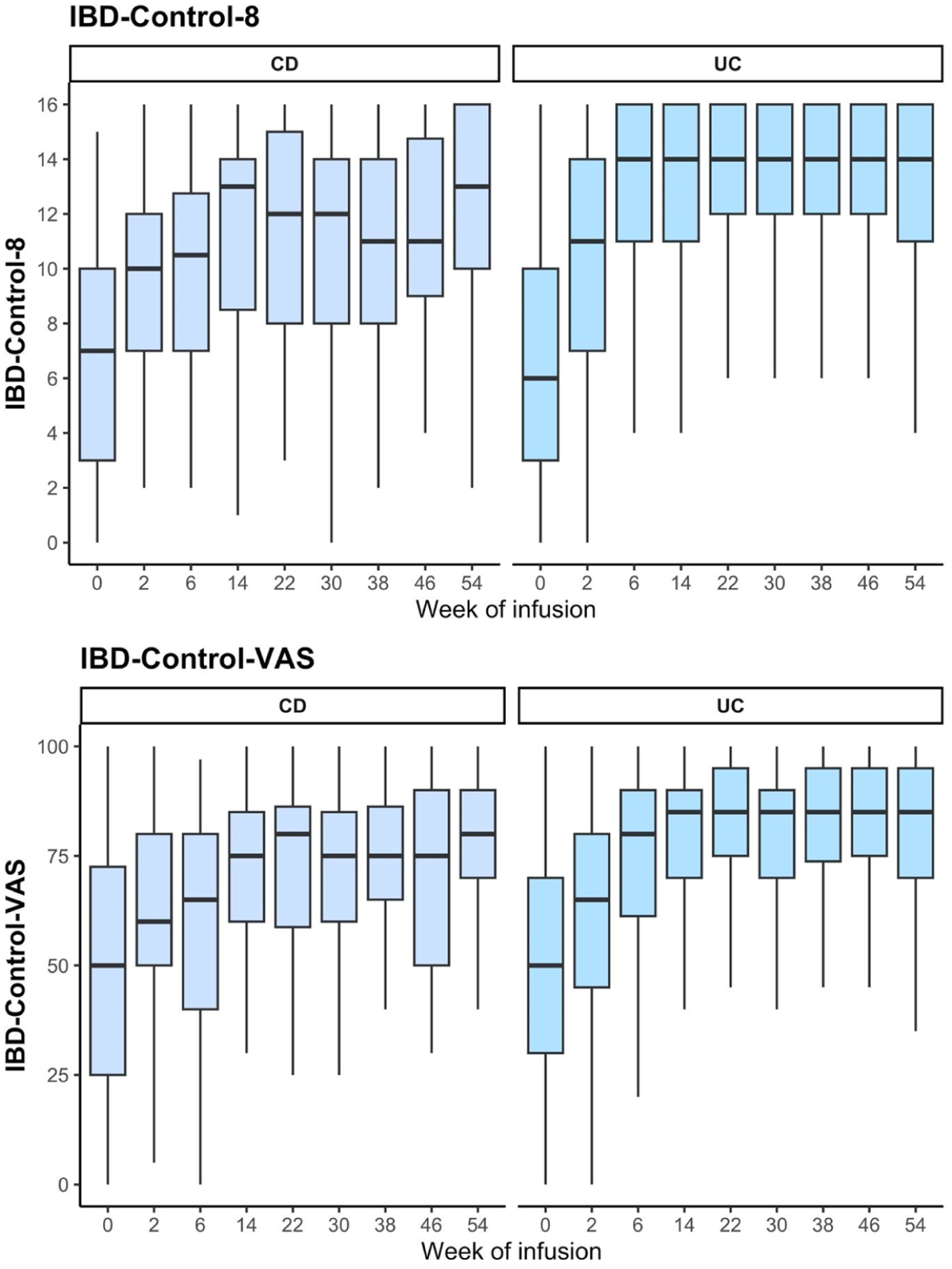
Trajectories of patient-reported disease control in patients who remained on vedolizumab at 1 year. Boxplots show the median and interquartile range of scores derived from the IBD-Control Questionnaire. Compared to baseline (Week 0), median scores for treatment-persistent cases were significantly higher at the post-induction visit (Week 14) and at all subsequent visits (p < 0.001).
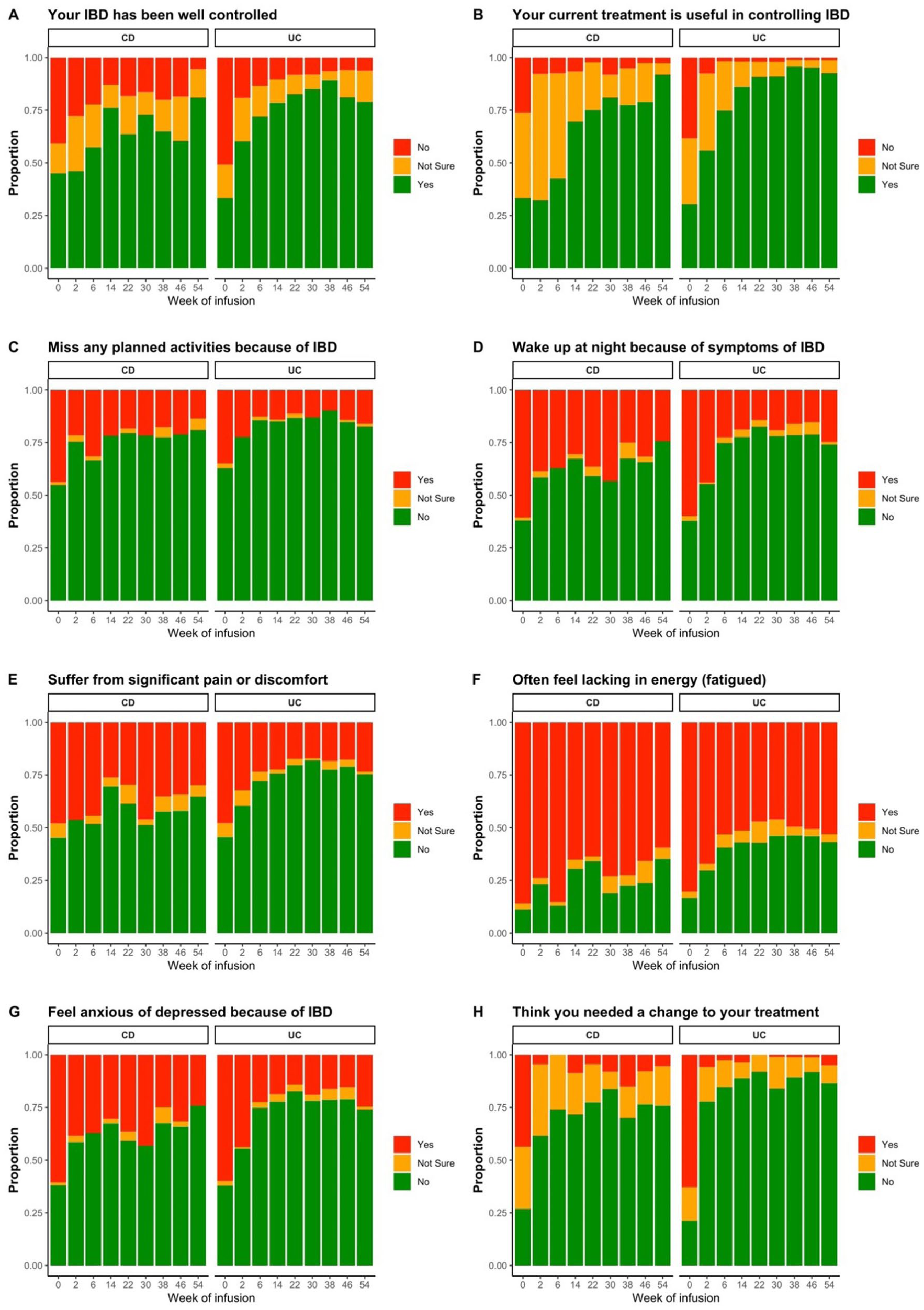
Trajectories of patient-reported health-related quality of life and treatment perception in 212 patients who remained on vedolizumab at 1 year. Responses to each of the component questions (a-h) of the IBD-Control-8 score, derived from the IBD-Control Questionnaire. The proportion of treatment-persistent patients reporting negative impacts (red bars) had reduced significantly across all eight questions by Week 14, and these improvements were sustained at all subsequent visits (p < 0.05).
Improvements were observed across each of the question items comprising the IBD-Control-8 scale, indicating positive impacts of vedolizumab on physical, social, psychological and treatment domains among those remaining on treatment, Figure 4. The trajectories of these health status measures were remarkably similar for UC and CD over the course of the first year of treatment.
At baseline, among the 1-year persistent cohort, the proportion of cases who believed their current treatment was useful in controlling their IBD was just 33% for CD and 31% for UC, respectively, Figure 4(b). By week 14, this had increased to 70% and 86%, respectively (p < 0.001 vs baseline). At 1 year, over 90% of persistent patients reported that treatment was useful (p < 0.001 vs baseline). Conversely, the proportion of cases thinking they needed a change to their IBD treatment at baseline was 44% for CD and 63% for UC, respectively. This reduced rapidly to less than 5% at post-induction and remained at this low level at 1 year for both sub-types of IBD (p < 0.001 vs baseline), Figure 4(h).
The proportion of patients reporting missed activities because of IBD had halved by week 14 (CD: 44% to 22%; UC: 35% to 13%; p < 0.001), and this improvement was sustained over the first year of treatment, Figure 4(c). The prevalence of waking up at night because of symptoms of IBD was reduced by at least half following induction (CD: 61% to 30%; UC: 60% to 19%; p < 0.001), and this benefit was maintained at 1 year, Figure 4(d). Significant pain or discomfort was reported by 48% of patients at week 0, reducing significantly by week 14 (CD: 26%; UC: 22%; p < 0.01) and remaining at similar levels at 1 year (CD: 30%; UC: 24%; p < 0.01 vs baseline), Figure 4(e).
Fatigue was highly prevalent at baseline, but the proportions who reported feeling lacking in energy (at least half the time) had reduced significantly by week 14 (CD: 86% to 65%; UC: 80% to 51%; p < 0.01). This reduction in fatigue rates from baseline was persistent at 1 year (CD: 60%; UC: 53%; p < 0.01), Figure 4(f). Mood disturbance attributed to IBD was reported by over half at baseline, with significant reductions in prevalence at week 14 (CD: 61% to 30%; UC: 60% to 16%; p < 0.001). At 1 year, the proportions who reported feeling anxious or depressed because of IBD remained at less than half their baseline values (CD: 24%; UC: 25%; p < 0.001), Figure 4(g).
Baseline predictors of 1-year persistence
Supplemental Table S1 compares baseline characteristics of patients who did (n = 212) or did not (n = 152) remain on scheduled treatment at 1 year. There were no significant differences with respect to age group, IBD subtype, disease duration, bio-naïve status or baseline steroid use. The non-persistent group had a significantly higher proportion classified as having moderate-to-severe clinical activity (61% vs 45%, p = 0.005) or moderate-to-severe PGA rating (80% vs 69%, p = 0.019), and significantly lower median PROM scores (IBD-Control-8: 3 vs 6, p < 0.001; IBD-Control-VAS: 35 vs 50, p < 0.001). Supplemental Table S2 summarizes the corresponding univariate odds ratios for these univariate associations. Stratified Kaplan–Meier survival analysis showed no significant difference in persistence between CD and UC among the total cohort (Figure 5(a)), but confirmed a significantly lower cumulative probability of drug survival for those with moderate or severe clinical disease activity at baseline (PMS⩾5 or HBI⩾8) (Figure 5(b)). We observed no differences in drug survival when the cohort was stratified by disease duration (Figure 5(c)) or prior biologic exposure (Figure 5(d)).
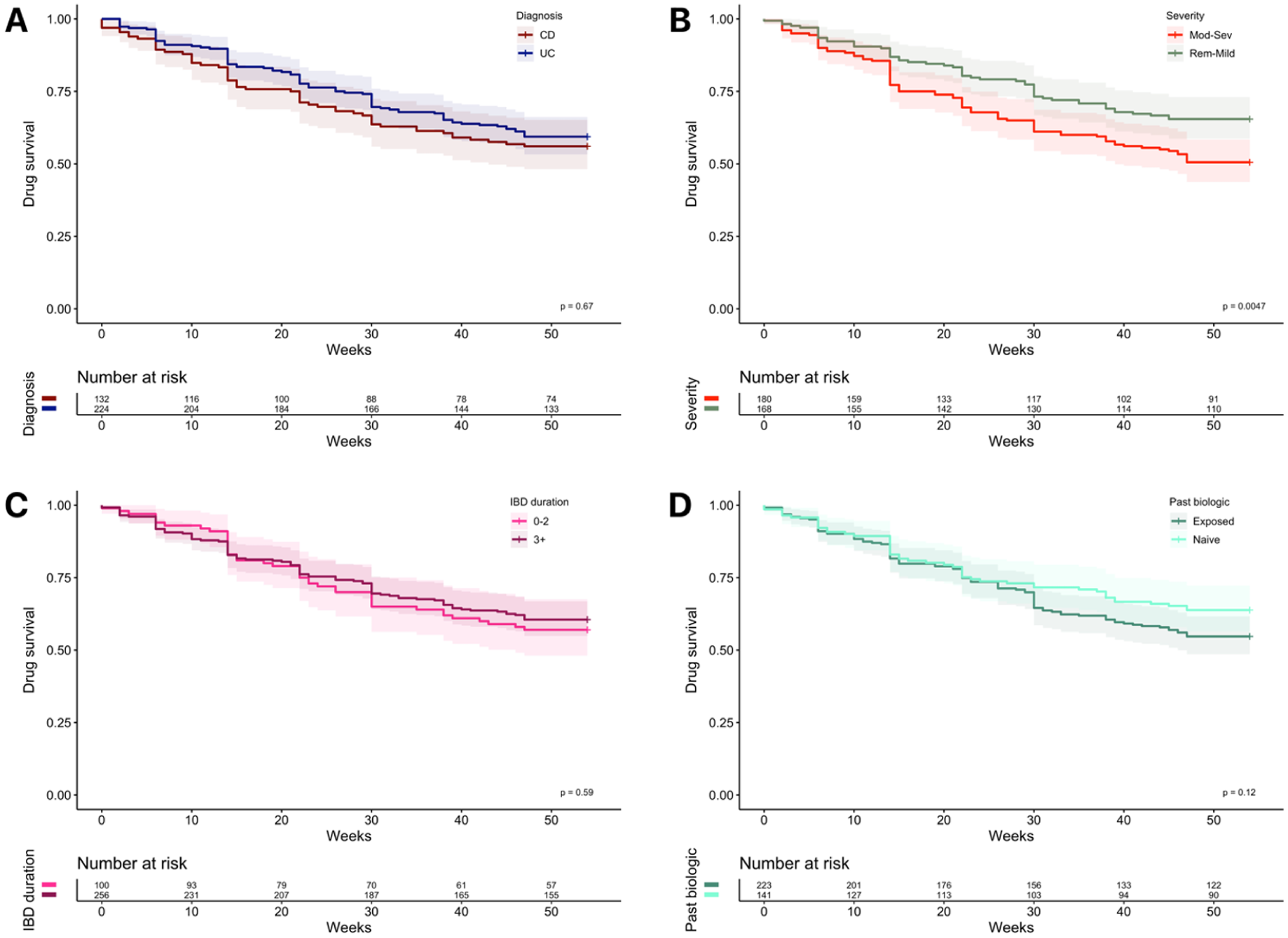
Drug survival in patients treated with vedolizumab. Kaplan–Meier survival analyses stratified by baseline patient characteristics. (a) By diagnosis (excluding eight cases with IBD unspecified). At 1 year, persistence rate was comparable (Crohn’s disease: 56% (74/132) vs ulcerative colitis: 59.4% (133/234)); (b) By severity of disease activity. Drug survival was significantly lower for patients with baseline scores in the moderate or severe range (Partial Mayo Score ⩾5 or Harvey–Bradshaw Index ⩾8). (c) By duration of inflammatory bowel disease (in years). (d) By past exposure to a biological agent (TNF-alpha inhibitor). p Values represent the log-rank test.
In multivariable models, baseline IBD-Control-8 score was the only observed variable that reached significance as an independent predictor of 1-year persistence (adjusted OR: 1.09 per unit increase; 95% CI: 1.01–1.18; p = 0.025). However, among patients with CD those with perianal disease had a significantly reduced adjusted odds of 1-year persistence relative to those without (OR: 0.20 (0.05–0.68), p = 0.014). Restricting the main model to patients with clinically active disease at baseline produced the same findings, with no association demonstrated for age group, IBD subtype, disease duration, bio-naïve status or baseline steroid use. Of the baseline health status measures, again, only IBD-Control-8 score reached significance (OR 1.10 per unit increase, 95% CI: 1.01–1.19, p = 0.026).
Post-induction predictors of 1-year persistence
Of the total cohort, 319 patients received at least one dose of maintenance treatment at week 14. Compared with persistent patients (n = 212), those subsequently stopping vedolizumab (n = 107) were more likely to have been taking steroids at week 14 (27% vs 14%, p = 0.007); have moderate-to-severe clinical activity (43% vs 16%, p < 0.001); moderate-to-severe PGA rating (43% vs 16%, p < 0.001) and had significantly lower median PROM scores at the time of first maintenance infusion (IBD-Control-8: 7 vs 14, p < 0.001; IBD-Control-VAS: 55 vs 80, p < 0.001). Corresponding univariate odds ratios for 1-year persistence are shown in Supplemental Table S2, with similar findings to baseline associations but with the addition of steroid use at week 14 being negatively associated with 1-year persistence. In multivariable analysis including all observed health status measures, the IBD-Control-8 score was the only variable reaching significance (adjusted OR: 1.19 (1.08 −1.32) per unit increase; p < 0.001). As with the baseline model, cohort restriction to clinically active cases did not alter these findings.
Characteristics of non-persistent patients at the time of treatment discontinuation
Supplemental Table S1 summarizes the profile of health status measures (including steroid status) at the last recorded visit for those patients who discontinued treatment before 1 year (n = 152; 42%). The majority of patients had active disease based on their SCCAI/HBI (77%), PGA (84%), with median PROM scores indicating sub-optimal patient-perceived control (IBD-Control-8, median (IQR): 6 (2–12); IBD-Control-VAS: 50 (25–75)). One in four (26%) were requiring ongoing or new steroid therapy at the time of stopping.
Clinical effectiveness among patients with active disease at baseline visit
We report traditional clinical activity endpoints for the subgroup of 279 patients who were categorized as having active disease at the first infusion visit based on HBI (⩾5 points) or PMS (⩾2 points). These are summarized in Supplemental Figure S1. Of 70 cases of active CD at baseline, 13% (n = 9) achieved clinical response; a further 29% (n = 20) achieved remission and 26% (n = 18) were in steroid-free remission by week 14. By 1 year, 31% (n = 22) were in remission and 29% (n = 20) in steroid-free remission.
Of the 201 cases with active UC at baseline, 20% (n = 41) achieved clinical response; a further 30% (n = 60) achieved remission and 27% (n = 54) were in steroid-free remission by week 14. By 1 year, 29% (n = 58) were in remission and 27% (n = 54) were in steroid-free remission. Of the eight cases with active IBD-U, 25% (n = 2) responded and a further 38% (n = 3) were in remission and steroid-free remission at week 14. At 1 year, the remission rates remained at 38% (n = 3). There were no statistically significant differences between subtypes of IBD for any of these traditional clinical endpoints.
Supplemental Figure S2 further illustrates the 1-year outcomes for the 279 patients with active disease, stratified by initial treatment response based on changes in baseline disease activity scores at week 14. This shows how treatment was continued beyond week 14 in 144 “primary non-responders,” with 56 such cases remaining on treatment at 1 year of which 21 (37.%) had achieved remission.
Side effects or AEs
There were 2331 visit records available belonging to the 364 patients, of which 1618 visits (69.4%) contained no record of any side effects or AEs, 353 visits (15.1%) contained a single category of adverse event, and the remaining 360 visits (15.4%) contained two or more categories within the same review record. In total, there were 1037 categorized events within 713 visit records (Supplemental Figure S3). The most common recorded individual category was headache. Only 11 patients with a record of an adverse event had their vedolizumab treatment stopped at the same visit (Supplemental Table S4). This suggests that the vast majority of recorded events were considered mild, self-limiting or unrelated to drug treatment. Of those continuing treatment at 1 year (n = 212), 48 (23%) had a record of an adverse event noted at the time of their last recorded infusion visit but nevertheless remained on vedolizumab.
Discussion
Unlike previous observational studies designed to replicate RCT entry criteria, we were interested in studying a real-world cohort that included anyone offered vedolizumab treatment as part of their routine clinical care. We aimed to provide an insight into case selection and to describe outcomes in real-world practice among those offered treatment. We found that patients treated with vedolizumab in routine UK practice differed from trial populations, with usage extended to older patients, those with IBD-U, proctitis or a stoma. Although we lacked comprehensive data on the full range of trial inclusion/exclusion criteria, we found that at least 30% of VEST participants had at least one criterion at baseline that would have made them ineligible for the GEMINI trials programme.2,3 At the time of first infusion, 19% of our cohort had a clinical activity index in the remission range. However, it should be noted that baseline symptom-based indices reflect only health status over the last 24 h for CD (HBI) or the last 3 days for UC (PMS).8,9 By way of contrast, just 5% of all cases were judged to be in remission based on the physician’s global assessment at baseline visit.
At 1 year, 58% of unselected cases continued to receive scheduled maintenance treatment. Persistence was similar across IBD subtypes among those selected for treatment. In a recent meta-analysis of observational studies, pooled estimates of 1-year persistence for vedolizumab were 73.8% in UC and 70.8% in CD. 13 Our lower figures may reflect that any patient treated with vedolizumab was eligible for VEST, regardless of clinical characteristics at baseline or the successful completion of induction, in contrast to some observational studies with stricter entry requirements. 14 As expected, current disease severity as measured by clinician- or patient-reported outcomes was associated with 1-year persistence in our cohort, both at the time of first induction dose and at the first maintenance infusion. However, we found no association with IBD sub-type or with bio-naïve status in univariate and multivariate analyses.
Treatment persistence does not equate to an objective response of gut inflammation to drug therapy. Subjective factors unrelated to inflammation can influence decisions about remaining on treatment. Hence, better patient- or clinician-reported health status is expected to predict decisions about treatment continuation. Nevertheless, the stronger association observed for IBD-Control-8 relative to other health status measures is interesting. This PROM has been endorsed by two international consensus committees for use in routine care,15,16 and used internationally.17–20 Unlike traditional HRQoL measures, IBD-Control measures “disease control from the patient perspective,” which considers physical, social and psychological impacts of IBD plus the novel domain of treatment perception.10,11 This may help to explain the association we observed for IBD-Control-8, since joint decision-making about treatment continuation is not solely based on symptoms (as reflected by activity scores), clinician-based assessments of disease activity (PGA) or (indeed) objective biomarkers.
We observed significantly improved IBD-Control scores and reduced prevalence of negative impacts across all its domains in those continuing treatment. Notably, the prevalence of fatigue at baseline was very high, and it remained the most prevalent impact among persistent patients but reduced significantly. This is consistent with a small study reporting reductions in visual analogue scale ratings of fatigue over 6 months among patients achieving remission on vedolizumab. 21
Previous reports of changes in HRQoL during vedolizumab treatment are relatively limited. Analysis of PROM data from the maintenance phase of the original GEMINI-1 trial showed improvement in Inflammatory Bowel Disease Questionnaire (IBDQ) scores, 36-Item Short Form Health Survey (SF-36) and EQ-5D among those receiving active treatment versus placebo for UC. 22 Similar data for the corresponding trial in CD have not been published, although sustained improvement in IBDQ scores has been reported in the GEMINI long-term safety trial. 23
Key strengths of the VEST study include multicentre participation, our focus on any patient offered treatment regardless of baseline characteristics, and the prospective collection of novel PROM data. However, the study has a number of important limitations. First, by design, it was an observational study lacking randomization or a control/comparator group. It was not intended to provide robust data on comparative effectiveness but rather to describe real-world case selection and describe the outcomes achieved among those offered vedolizumab treatment. Our data show that comparable levels of persistence were achieved among cases of CD and UC who were treated with vedolizumab.
Second, we did not systematically collect information on biomarkers (e.g. faecal calprotectin), endoscopic or radiological assessments. This was an observational study without protocol-driven testing. However, the lack of data on objective markers of inflammation does not detract from our reporting of real-world levels of drug persistence, clinician- and patient-reported outcomes experienced by those offered treatment in routine UK practice. Third, selection bias is unavoidable in an observational study of real-world practice, and our data suggest patients selected for vedolizumab with CD were relatively “milder” at baseline than those with colitis in terms of symptom scores, albeit PGA ratings were similar.
Fourth, the cohort included some patients with symptom-based indices in the remission range at baseline, reflecting real-world pathways. Such patients had higher levels of persistence than the majority with clinically active disease at the first infusion visit, such that the overall persistence figure for the VEST cohort is higher (58% overall, vs 54% for the active group). However, only 19 patients (5%) were judged to be in remission at baseline by their clinician based on global assessment. There are abundant data already from RCTs and observational studies describing traditional rates of response, remission and improvements in inflammatory markers focused on cohorts of patients with objectively verified “active” disease at baseline.2–4 Rates of clinical response and remission among “active” cases in the present study were somewhat lower than some previous reports, 7 albeit this may reflect the unselected nature of the cohort and our stringent non-responder imputation analyses.
Fifth, in common with any observational study, 7 our data reflect prevailing patterns of case selection in a specific health service context and during a defined time period. With the recent expansion of alternative drug treatments for IBD,24,25 the profile of patients selected for individual advanced treatments continues to evolve. Sixth, we demonstrated greater diversity of patients treated in clinical practice compared to RCT cohorts, but we did not have data on the full range of potential trial exclusions, such as major comorbidities – factors that may influence real-world treatment outcomes and are worthy of further study. 26
The lack of biomarker data in our study limited the evaluation of true anti-inflammatory effectiveness and reporting against modern “treat-to-target” goals. 27 However, our real-world data suggest it is not uncommon for patients to continue treatment despite clinically active disease post-induction (Supplemental Figure S2). This is consistent with the recent IBD PODCAST study, which suggested slow uptake of stringent STRIDE-II recommendations in clinical practice. 28
Conclusion
In conclusion, we have shown that over half of IBD patients selected for treatment with vedolizumab in UK clinical practice remained on treatment at 1 year, with only 3% experiencing possible side effects leading to immediate treatment cessation over this period. Significant, sustained improvements in quality of life and treatment perception were observed among those remaining on treatment, including a reduction in perceived impacts of IBD on planned activities and on the prevalence of pain, sleep disturbance, altered mood and fatigue.
Supplemental Material
sj-docx-1-tag-10.1177_17562848261446551 – Supplemental material for The UK vedolizumab real-life experience study in inflammatory bowel disease (VEST): patient characteristics, drug persistence and patient-centred outcomes
Supplemental material, sj-docx-1-tag-10.1177_17562848261446551 for The UK vedolizumab real-life experience study in inflammatory bowel disease (VEST): patient characteristics, drug persistence and patient-centred outcomes by Keith Bodger, Cheryl Booker, Frederick Taylor, Tariq Ahmad, Stuart Bloom, Jeffrey Butterworth, Klaartje Kok, Alan Lobo, Peter Irving and J. R. Fraser Cummings in Therapeutic Advances in Gastroenterology
Supplemental Material
sj-docx-2-tag-10.1177_17562848261446551 – Supplemental material for The UK vedolizumab real-life experience study in inflammatory bowel disease (VEST): patient characteristics, drug persistence and patient-centred outcomes
Supplemental material, sj-docx-2-tag-10.1177_17562848261446551 for The UK vedolizumab real-life experience study in inflammatory bowel disease (VEST): patient characteristics, drug persistence and patient-centred outcomes by Keith Bodger, Cheryl Booker, Frederick Taylor, Tariq Ahmad, Stuart Bloom, Jeffrey Butterworth, Klaartje Kok, Alan Lobo, Peter Irving and J. R. Fraser Cummings in Therapeutic Advances in Gastroenterology
Footnotes
Acknowledgements
We would like to thank all the patients who took part in the study as well as the contribution of research teams across all sites.
Declarations
ORCID iDs
Supplemental material
Supplemental material for this article is available online.
References
Supplementary Material
Please find the following supplemental material available below.
For Open Access articles published under a Creative Commons License, all supplemental material carries the same license as the article it is associated with.
For non-Open Access articles published, all supplemental material carries a non-exclusive license, and permission requests for re-use of supplemental material or any part of supplemental material shall be sent directly to the copyright owner as specified in the copyright notice associated with the article.