
Abstract
Small bowel disorders often present insidiously, with early symptoms being non-specific. Moreover, the small intestine’s unique anatomical position renders it difficult to access using conventional examination methods, frequently leading to delays in the diagnosis and treatment of small bowel disorders. Confocal laser endomicroscopy (CLE), as an emerging technique based on confocal microscopy, enables high-resolution assessment of gastrointestinal mucosa at cellular and subcellular levels. It provides real-time imaging, thereby achieving an ‘optical biopsy’. The application of this technology not only enhances the ability to identify early lesions and dysplasia but also addresses the limitations of traditional endoscopic biopsy techniques – such as poor targeting and low efficiency of random biopsies – by guiding targeted biopsies. While its potential in digestive diseases is significant, particularly as an adjunct to histopathology, its application in the small intestine is still emerging. Current obstacles, such as procedural complexity, high equipment costs and a lack of specific diagnostic criteria, limit its widespread use. This narrative review synthesises findings from studies published since 2005 to critically evaluate the role of CLE in conditions including inflammatory bowel disease, functional bowel disorders and small bowel polyps, providing a balanced perspective for future research and clinical translation.
Introduction
Small bowel disorders encompass inflammatory bowel disease (IBD), functional bowel disorders and small bowel polyps. Such diseases typically present with an insidious onset and low clinical specificity. This diagnostic difficulty is further compounded by the fact that the small intestine is situated deep within the abdominal cavity, measuring 5–7 m in total length. The affected areas are difficult to examine, often leading to delays in the diagnosis and treatment of small bowel disorders. 1 Conventional endoscopic modalities have notable limitations in this context. Capsule endoscopy, while useful for visualisation, cannot distinguish between benign and malignant lesions or perform biopsies; it also carries a risk of capsule retention, potentially requiring surgical intervention.2,3 Conversely, device-assisted enteroscopy allows for tissue sampling but is plagued by concerns over insufficient sampling, which may lower detection rates, and procedure-related risks such as perforation and haemorrhage. 4 Over the past decades, confocal laser endomicroscopy (CLE) has emerged as a non-destructive endoscopic adjunctive technique, to some extent compensating for the limitations of conventional endoscopy. 5 Building on the principles of confocal microscopy, CLE uses a low-power laser to illuminate tissues and detect reflected fluorescence, generating real-time, high-resolution images at the cellular and subcellular levels.6,7 This ‘optical biopsy’ capability enables real-time monitoring of structural alterations in vasculature and connective tissue, yielding images magnified up to 1000 times with submicrometre precision.6,8 In this regard, CLE serves as a functional bridge between imaging technology and pathological diagnosis, assisting clinicians in precisely selecting biopsy sites to achieve targeted biopsies and enhance detection rates. 9 These advantages not only enhance diagnostic accuracy but also potentially optimise the biopsy yield and reduce the frequency of blind random sampling, offering significant benefits in clinical practice. Existing literature primarily addresses CLE applications across the entire gastrointestinal tract, with relatively limited in-depth exploration of small bowel diseases. 10 Therefore, this paper employs a narrative review methodology. A comprehensive literature search was conducted across PubMed, Web of Science and Google Scholar for relevant studies published since January 2005. We utilised search terms including, but not limited to, ‘confocal endoscopy’, ‘small bowel diseases’, ‘optical biopsy’, ‘inflammatory bowel disease’, ‘functional bowel disease’, ‘small bowel polyps’, ‘celiac disease’ and ‘NSAID-associated enteropathy’. This narrative review objectively analyses the current status and research progress of CLE in small bowel diseases, along with its clinical value and practical challenges, aiming to provide a theoretical basis for further clinical implementation of this technology.
Inflammatory bowel disease
IBD subtypes primarily encompass ulcerative colitis (UC) and Crohn’s disease (CD). Although UC is largely confined to the colorectum, CD can affect any part of the gastrointestinal tract, including the small intestine. Therefore, CLE research in the small bowel has focused predominantly on CD. The pathogenesis of IBD is multifactorial, involving interactions between genetic predisposition, microbial shifts and host immunity. 11 It manifests as structural and functional alterations that are often invisible to conventional endoscopy. CLE, with its high-resolution imaging capabilities, shifts the research perspective from macroscopic morphology to cellular-level, enabling in situ dynamic observation of the gut microbiota and precise identification of epithelial cell junctions and goblet cell distribution.12,13 Central to IBD pathology is intestinal barrier dysfunction. By monitoring the abnormal leakage of fluorescein sodium from the blood vessels into the intestinal lumen, CLE translates this physiological defect into a quantifiable visual marker.7,14 This real-time assessment of mucosal barrier repair is closely associated with clinical outcomes. The Watson score was developed to systematically characterise these biomarkers, which grade mucosal integrity from I (normal) to III (structural defects). In 2012, Kiesslich et al. 15 established that patients with barrier dysfunction (Watson II/III) face a significantly higher relapse risk than those with endomicroscopic healing (Watson I). Concurrent research by Turcotte et al. 16 further identified the density of epithelial gaps at the terminal ileum as a potent predictor, with every 1% increase in gap density correlating to a 1.1-fold increase in the risk of major adverse events. This prognostic potential was subsequently validated in a randomised controlled trial by Karstensen’s team, which confirmed that ileal mucosal fluorescein leakage serves as an independent predictor of CD relapse. 17 The utility of these markers extends beyond native mucosa to postoperative settings. A prospective study by Auzoux et al. 18 found that in patients in endoscopic remission (Rutgeerts i0–i1), an elevated baseline Watson score (⩾2) remained significantly associated with symptomatic recurrence over a 38-month follow-up. Collectively, these findings – supported by longitudinal in vivo cellular imaging in animal models – demonstrate that CLE can offer insights into IBD pathogenesis and prognosis that are not readily available through conventional endoscopy. 19
Beyond functional assessment, CLE provides multi-dimensional morphological information essential for the tailored management of IBD. Normal small intestinal mucosa displays long, finger-like villi with visible goblet cells and continuous epithelial integrity, distinct from the circular or oval crypt structures dominating the colon. 20 In active small bowel IBD, CLE identifies marked architectural abnormalities: villi exhibit blunting, fusion or complete atrophy, often accompanied by cellular desquamation and enlarged epithelial spaces.21–24 While specific small bowel diagnostic criteria remain nascent, current clinical practice frequently draws upon established colonic patterns; for instance, UC typically presents with diffuse, continuous and severe crypt structural disruption, including bifid crypts, branched crypts, crypt shortening, reduced crypt numbers and irregular surface crypts. CD, conversely, is characterised by patchy lesions, with confocal imaging revealing discontinuous areas of crypt structural destruction, focal cryptitis and epithelioid granulomas.8,25,26 Nevertheless, these pathological manifestations must be interpreted within their specific anatomical context. Given that the small bowel’s structural framework is defined by villi rather than deep-seated crypts, the diagnostic focus must pivot towards assessing villous morphology and brush border integrity, rather than relying on colonic crypt metrics. To translate these microscopic observations into clinical practice, several scoring systems derived exclusively from colonic pathology have yet to be formally applied to the small bowel, but their potential utility in this context warrants discussion. The Kieslich team categorised the activity of IBD into inactive, mild to moderate and severe based on three indicators: crypt structure, inflammatory cell infiltration and microvascular alterations. 27 Similarly, Li et al. 28 employed a four-grade scale of crypt loss to enhance endoscopic-pathological concordance. In addition to crypt-centric metrics, more comprehensive indices have emerged. The CDEAS system integrates parameters including crypt count, distortion, micro-erosion area, inflammatory infiltration, vascular heterogeneity and goblet cell count. Goblet cell density itself has shown particular promise: in CD patients, it reaches 85% during remission but plummets to below 6% in active disease. 29 The subsequent ENHANCE index established an inflammatory grading model based on four objective parameters (vessel diameter >20 μm, crypt lumen dilatation, fluorescein leakage and crypt structural irregularity), achieving an overall accuracy of 79.6% with a total sensitivity of 57.8% and total specificity of 82.8%. 30 A critical limitation remains, however: as these standardised indices were developed solely based on colonic anatomy, their direct extrapolation to the small intestine may misrepresent clinical status due to the fundamental divergence in vascular patterns and tissue responses between the two regions. Specifically, while colonic activity is assessed via crypt irregularity, CLE evaluation in the small bowel must focus on villous blunting, fusion and the visibility of the brush border. As shown in preliminary CD studies, the loss of the typical finger-like villous structure serves as a more reliable indicator of active inflammation in the ileum than crypt counts. In the absence of a validated small-bowel-specific consensus, these criteria must be interpreted as exploratory frameworks rather than definitive standards. Pending such validation, the endoscopist’s expertise remains paramount. Chang et al. investigated the influence of endoscopists’ experience on the identification of mucosal barrier defects and intestinal permeability characteristics by CLE. The study showed that experienced analysts had an accuracy rate of up to 95.9% in identifying relevant features, significantly higher than that of inexperienced analysts (87.8%) and pathologists (85.6%, p < 0.001). Moreover, experienced analysts demonstrated the highest inter-observer consistency, and among all CLE features, the interpretation consistency of fluorescein leakage was the most ideal. 31 Consequently, until large-scale small-bowel validation is conducted, expert interpretation remains the cornerstone of CLE application in this context.
As treatment targets for IBD shift from clinical symptom control towards microscopic mucosal healing and endomicroscopic remission, the value of CLE for real-time functional imaging becomes increasingly evident. By quantifying fluorescein leakage patterns and vascular tortuosity, CLE enables a more granular assessment of therapeutic endpoints beyond the resolution of conventional endoscopy.32–35 The frontier of this technology lies in molecular endomicroscopy, which allows for the in vivo visualisation of biological targets to predict drug efficacy – a cornerstone of personalised medicine. 36 Notably, patients with high mTNF immunocytes – the primary therapeutic target for anti-TNF agents – demonstrated a treatment response rate as high as 92% (compared to only 15% in patients with low mTNF+ cells), with a longer duration of response. 37 In this approach, fluorescent-labelled antibodies function as molecular probes that bind directly to these mTNF targets, enabling clinicians to visualise target density as a biological predictor of therapeutic success. Expanding this proof of concept, preliminary studies have demonstrated the feasibility of using fluorescent-labelled vedolizumab to image α4β7 integrin expression in vivo. 38 Although currently limited to small-scale pilot studies (n = 5), this strategy suggests that visualising drug–target binding during endoscopy could rationalise the selection of vedolizumab for CD patients. Crucially, such molecular markers facilitate the early identification of treatment responders, thereby mitigating the complications and costs associated with ineffective therapies. By optimising the attainment of deep remission, this personalised strategy holds the potential to improve long-term disease management and significantly reduce hospitalisation rates.39,40
Long-term complications in small-bowel IBD patients, including carcinoma in situ and malignant transformation, warrant close attention. Although data specifically targeting the small bowel are sparse, evidence from colonic surveillance indicates that CLE significantly enhances the detection of dysplastic lesions. A randomised controlled trial found that chromoendoscopy-guided CLE increased the detection rate of neoplasia, with a sensitivity of 94.7% and specificity of 98.3% for diagnosing intraepithelial neoplasia. 27 Another meta-analysis confirmed that compared with magnifying endoscopy and virtual chromoendoscopy, CLE demonstrated the highest accuracy in distinguishing between neoplastic and non-neoplastic lesions. 41 Additionally, fluorescently labelled MMP-14 antibodies have been shown to successfully highlight tumour transformation by targeting proteolytic activity within inflamed mucosa, effectively distinguishing it from benign inflammatory lesions. 39 However, clinical application in the small bowel is tempered by inherent technical constraints: the fluorescent agents used in CLE cannot label cell nuclei, precluding the precise histological grading of dysplasia. Furthermore, CLE’s penetration depth is restricted to the mucosal layer, rendering it incapable of assessing submucosal invasion or the transmural extent of CD-associated complications. 8 Additionally, the tortuous anatomy and frequent strictures of the small bowel present significant challenges for endomicroscopic access compared to colonic surveillance. Therefore, histological assessment after biopsy remains the gold standard. In summary, by capturing real-time microscopic dynamics, CLE refines the IBD diagnostic-therapeutic algorithm, although the standardisation of small-bowel-specific protocols remains an ongoing challenge.
Functional bowel disorders
Functional bowel disorders constitute a group of conditions characterised by chronic abdominal pain, diarrhoea or constipation as primary manifestations, without any identifiable organic pathology or biochemical abnormalities to account for the symptoms. Irritable bowel syndrome (IBS), as a common functional bowel disorder, may arise from multiple factors, including visceral hypersensitivity, gut microbiota dysbiosis and alterations in mucosal and immune function. 42 Some scholars have also proposed the ‘food antigen hypothesis’. Specifically, CLE-guided food challenge tests have captured real-time mucosal permeability alterations and eosinophil activation following antigen exposure, confirming pathological changes associated with non-classical food allergies. 43 Research indicates that food allergy patients exhibit significantly higher frequencies of barrier dysfunction in the terminal ileum, with micro-erosions and fluorescein leakage observed in over 90% of cases. 44 Fritscher-Ravens et al. 45 also supported this hypothesis by documenting postprandial increases in intraepithelial lymphocytes via CLE recording. However, the diagnostic accuracy of this approach is not consistently supported by all studies. A 2022 multicentre, double-blind trial by Bojarski et al. 46 reported a sensitivity of only 51.4% and specificity of 67.9% for diagnosing wheat sensitivity – falling significantly below the pre-defined 80% accuracy threshold. 46 This suggests that CLE-guided antigen testing results can vary significantly across different study cohorts.
Despite its widespread clinical application, traditional endoscopy lacks sufficient sensitivity and specificity in identifying functional pathological alterations in IBS patients, frequently resulting in missed diagnoses. 47 The application of CLE addresses this limitation by facilitating the identification of microinflammation in vivo. Robles-Medranda et al. employed CLE in conjunction with histological assessment to identify the presence of colonic mucosal microinflammation in vivo, which occurred at a rate six times higher than in healthy individuals. Endoscopic alterations in crypt morphology, size and distribution; widened intercellular spaces; fluorescein leakage into crypt lumens and prominent, dilated, branching vessels are all considered indicators of inflammation. It is noteworthy that while this pivotal study established CLE criteria for detecting microinflammation based on colonic findings, it also briefly noted the presence of similar inflammatory changes in the small bowel. This preliminary observation supports the use of CLE for detecting microinflammation and prompts a critical discussion regarding the role of low-grade inflammation in IBS pathogenesis. 48 However, the cause of increased epithelial interstitial space remains unexplained. As CLE progresses, some studies hypothesise that increased shedding of epithelial cells, leading to greater density of mucosal interstitial spaces, may be one factor contributing to impaired intestinal barrier function. 49 It may therefore be inferred that CLE also serves as a valuable tool for assessing intestinal epithelial barrier dysfunction in patients with disorders of gut–brain interaction. 50 Although current research remains largely exploratory with small sample sizes, its dynamic assessment capabilities support the development of personalised treatment strategies. By potentially revealing specific pathological mechanisms (e.g. microinflammation, barrier dysfunction), CLE could facilitate a shift from a purely symptom-based management paradigm towards a more mechanism-informed approach, pending further validation in small intestinal disorders.
Small bowel polyps
Small bowel polyps are abnormal growths protruding from the surface of the intestinal mucosa into the intestinal lumen, carrying a potential for malignant transformation. 51 The sensitivity of traditional endoscopy for detecting small bowel polyps is approximately 80%, with even lower detection rates for minute lesions. While histological analysis following biopsy or resection is the definitive diagnostic method, the procedural complexity of enteroscopy can necessitate auxiliary tools to streamline clinical decision-making. 52 CLE offers augmented diagnostic capabilities by providing real-time morphological insights, which may aid in the differentiation between benign and neoplastic lesions, thereby supporting more informed interventional strategies. Peutz-Jeghers syndrome (P-J syndrome) is an autosomal dominant genetic disorder characterised by multiple hamartomatous polyps in the gastrointestinal tract, most commonly affecting the small intestine. Due to its complications and the high incidence of small bowel cancer, regular monitoring is of paramount importance. 53 CLE has been utilised to assess polyps in patients with P-J syndrome, offering a supplementary means to assess surface micro-architecture and potentially identify focal atypia within hamartomas. 54 In support of this, Pittayanon et al. 55 established criteria for distinguishing non-adenomatous from adenomatous lesions under CLE, noting that non-adenomatous lesions exhibit normal epithelial borders, while adenomatous ones manifest as mucosal opacity and structural irregularity. Complementing these findings, Professor Kenshi Yao proposed a vessel plus surface classification system based on microvessels and micro-surface features to determine tumour benignity or malignancy. 56 This method enhances diagnostic objectivity, proving particularly suitable for real-time differentiation of complex lesions. Muhammad et al., drawing upon confocal characteristics of Barrett’s oesophageal dysplasia, established diagnostic criteria for duodenal dysplasia in pCLE. These criteria manifest visually as dark, irregular epithelial borders, varying degrees of epithelial border thickening and atypical vascular dilation. Through comparative analysis of CLE imaging with histopathological findings, it was determined that the accuracy, sensitivity and specificity of in vivo diagnosis via pCLE were 83%, 92% and 78%, respectively. 51 Additionally, CLE serves to evaluate lesion margins, depth and whether residual tissue remains following polypectomy.57–59 Consequently, the value of CLE complements that of a mere diagnostic tool – its potential in guiding precise endoscopic resection and post-operative monitoring may optimise the full-cycle management pathway for small bowel polyps, embodying the practice of precision medicine in endoscopy.
Celiac disease
Celiac disease is an immune-mediated hereditary disorder triggered by gluten intolerance, which provokes an abnormal immune response leading to alterations in the intestinal epithelium and chronic inflammation. This ultimately results in malabsorption and nutritional metabolic disorders. 60 Upper gastrointestinal endoscopy with multiple biopsies from the distal duodenum constitutes the gold standard for diagnosing celiac disease. However, repeated procedures significantly increase the risk of complications such as haemorrhage and perforation, and may compromise the accuracy of mucosal healing assessment. 61 Among celiac disease, the intestinal epithelium primarily exhibits three structural alterations: villous atrophy, changes in goblet cell density and crypt hypertrophy. 62 CLE enables more precise assessment of small intestinal villous atrophy, including mosaic patterns, villous fan-shaped changes and reduced duodenal villi, thereby reducing the number of biopsies required and enhancing diagnostic sensitivity.63–66 Boschetto et al. 62 proposed a method for assessing alterations in small intestinal epithelial structure by monitoring duodenal epithelial villi and goblet cell density via CLE. Analysis of the endoscopic images revealed that this approach demonstrated an accuracy exceeding 80%. 67 If crypt hypertrophy is defined as the identification of a single crypt within the duodenal mucosa, it maintains high sensitivity (92.3%) and specificity (88.2%) for diagnosing celiac disease. 68 Despite these high diagnostic metrics for structural damage, evidence suggests that CLE cannot yet fully replace traditional histopathology. A pivotal study by Venkatesh et al. in a paediatric cohort highlighted this discrepancy; while CLE achieved 100% sensitivity in identifying advanced mucosal destruction (Marsh 3a/b), it proved significantly less effective at detecting increased intraepithelial lymphocytes. This specific limitation indicates that CLE may lack the requisite sensitivity to diagnose early-stage celiac disease (e.g. Marsh 1), where villous architecture remains largely preserved. 9 Similar findings in adult populations by Zambelli et al. 66 corroborate that while CLE images correlate strongly with advanced Marsh grades, the inability to reliably quantify intraepithelial lymphocytes remains a barrier to a non-biopsy approach. Therefore, CLE currently functions as a specialised adjunctive tool; its primary clinical value lies in guiding targeted biopsies rather than serving as a replacement for traditional histological examination. 69
Nonsteroidal anti-inflammatory drug-induced enteropathy
Nonsteroidal anti-inflammatory drug-induced enteropathy (NSAID-induced enteropathy) refers to a condition of intestinal damage caused by prolonged or excessive use of NSAIDs. Although these medications are widely employed to alleviate various chronic pains and treat conditions such as osteoarthritis and rheumatoid arthritis, their long-term administration can lead to disruption of the intestinal mucosal barrier by inhibiting the cyclooxygenase pathway.70,71 It is estimated that approximately 60%–70% of long-term NSAID users exhibit damage to the small intestinal mucosa, with some cases progressing to irreversible intestinal wall fibrosis or strictures. 72 In indomethacin-induced injury, CLE is instrumental in quantifying epithelial gap density, a morphological marker of cell shedding and apoptosis. While CLE captures structural defects, molecular analyses indicate this damage is driven by TNF-α, NF-κB and caspase-3 up-regulation, alongside tight junction protein depletion. Real-time imaging has confirmed that both mucosal protectants (e.g. teprenone) and acid-suppressants (e.g. rabeprazole) effectively limit gap formation. This stabilisation is largely attributed to the suppression of TNF-α signalling, which preserves intestinal barrier integrity.7,73,74 Beyond direct chemical injury, the intestinal microbiota may also contribute to pathogenesis. A placebo-controlled study using video capsule endoscopy demonstrated that rifaximin significantly reduced the incidence of small bowel mucosal breaks by more than half, highlighting the role of intestinal bacteria in NSAID-associated damage. 75 By enabling real-time visualisation of epithelial gap dynamics and the interplay between microbiota and the mucosal barrier, CLE offers a useful approach for investigating the multi-factorial pathogenesis of NSAID-induced enteropathy. Such observations may inform the development and efficacy assessment of novel therapeutic interventions (Figure 1, Table 1).
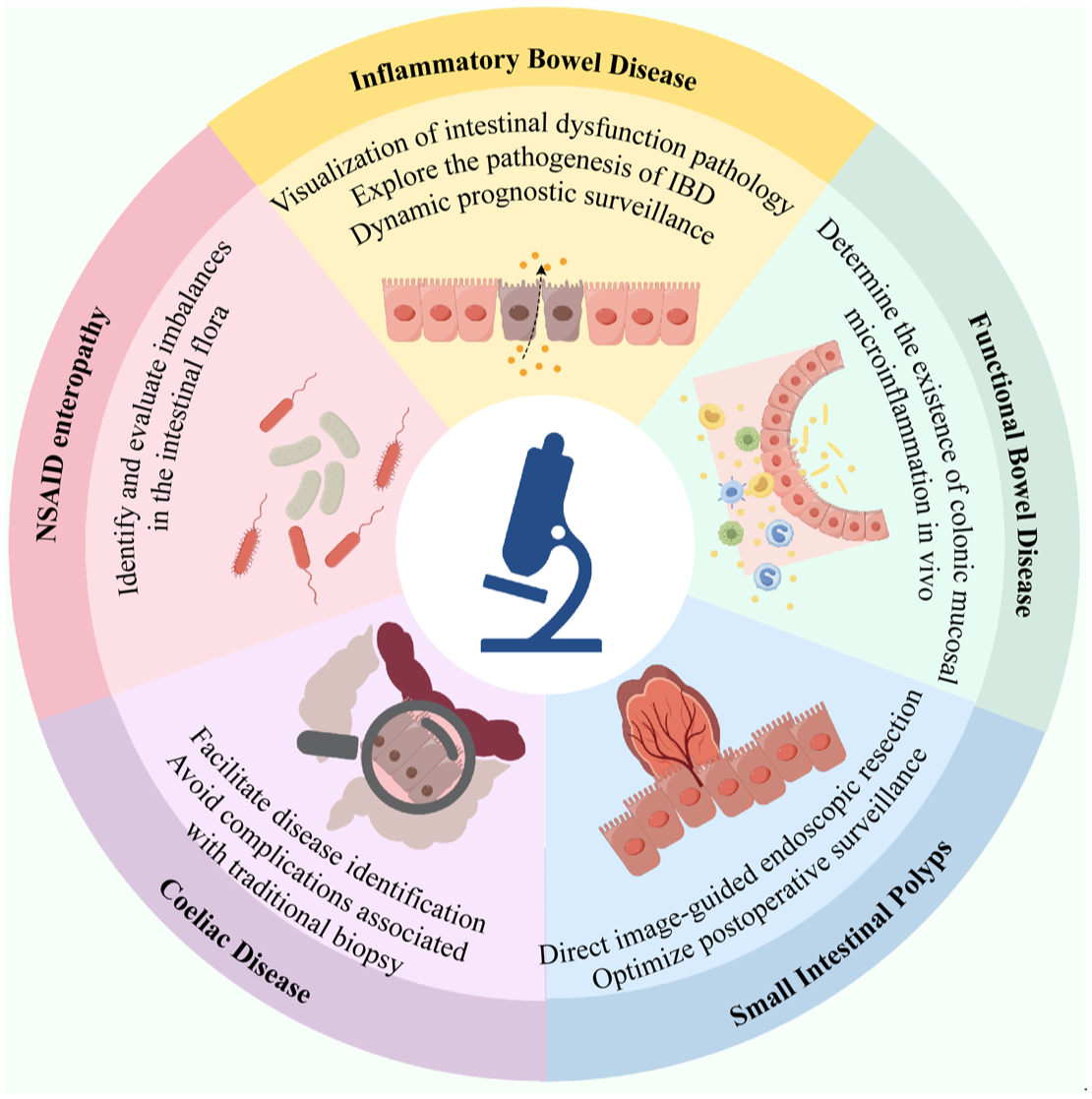
The role of confocal laser endomicroscopy in the diagnosis and treatment of small intestinal diseases.
CLE diagnostic features of small intestinal diseases.

CD, Crohn’s disease; CLE, confocal laser endomicroscopy; IBD, inflammatory bowel disease; UC, ulcerative colitis.
Summary and outlook
This paper discusses the application and research progress of CLE in small bowel diseases. CLE, an endoscopic technique capable of providing high-resolution live tissue examination, is currently primarily employed for conditions such as IBD, functional bowel disorders and intestinal polyps. It offers significant advantages in revealing the presence of microinflammation, assessing intestinal barrier function, identifying gut bacteria, distinguishing polyps with early malignant potential and monitoring villous atrophy in the small intestine. This makes it highly significant for investigating the pathogenesis of small bowel diseases, facilitating diagnosis and evaluating treatment outcomes, thereby enhancing the precision and efficacy of small bowel disease management.
Despite these advantages, the widespread clinical adoption of CLE in the small bowel faces significant practical and technical barriers, and it cannot yet replace the histopathological gold standard. First, the technology is limited by inherent physical constraints, such as a penetration depth of only 250 µm, which restricts assessment to the superficial mucosa and hinders the evaluation of submucosal lesions. Furthermore, the extremely narrow field of view, while offering high resolution, can lead to cognitive bias regarding the spatial distribution of lesions, thereby increasing the risk of missed diagnoses.76–78 Second, anatomical accessibility remains a major hurdle; unlike colonic examinations, probing the deep small intestine relies heavily on balloon-assisted enteroscopy, which extends procedure times and requires a high level of expertise available only in specialised centres. 77 In real-world clinical practice, the application of small bowel CLE is primarily confined to the duodenum or selected cases during device-assisted enteroscopy, which limits its broader use in routine deep-intestinal screening. Moreover, most available evidence stems from small-scale pilot studies; hence, the real-world reliability and diagnostic accuracy of CLE in the deep small intestine require further investigation, given that limited sample sizes may not adequately reflect clinical outcomes across diverse patient populations. Additionally, a lack of universal diagnostic standards and high equipment costs present significant barriers to widespread adoption. Safety considerations also remain paramount; although intravenous fluorescein is typically well-tolerated, the potential for rare but severe adverse events – ranging from nausea to anaphylaxis – necessitates a meticulous risk–benefit appraisal. In clinical practice, the ‘optical biopsy’ approach must be strategically utilised where the benefits of minimising physical tissue trauma outweigh these systemic risks. Furthermore, the steep learning curve and inter-observer variability further limit its broader implementation in primary care settings.10,78
Looking forward, the innovation of CLE will focus on intelligence and molecular characterisation. The integration of image fusion, panoramic stitching and video-grade high-resolution 3D imaging is expected to provide seamless visualisations and more precise lesion localisation. Simultaneously, AI-driven automated diagnostic systems will help flatten the learning curve and improve diagnostic consistency across observers. Beyond morphological assessment, the rise of molecular endoscopy will drive CLE towards functional diagnosis at the molecular level, utilising specific probes to achieve early and precise disease stratification. In conclusion, while CLE is currently a complementary tool, it is poised to become an indispensable ‘optical navigation’ instrument in the precision management of small bowel disorders as technologies mature and evidence-based validation accumulates.