
Abstract
Background:
Improvement in internal hemorrhoids is frequently observed after endoscopic submucosal dissection (ESD) for rectal intraepithelial neoplasia. This study investigated the effectiveness of rectal ESD in the management of internal hemorrhoids.
Objectives:
Twenty-three patients who underwent ESD for tumors adjacent to the dentate line and associated with internal hemorrhoids.
Design:
A single-arm, retrospective multi-center study.
Methods:
The focal improvement (at the scarring area after ESD) and complete improvement rates of hemorrhoids at follow-up colonoscopies were evaluated.
Results:
Most patients (87%) had mild hemorrhoids. The focal and complete improvement rates of hemorrhoids were 83% and 48%, respectively. Complete improvement rates were 75% (3/4), 42% (5/12), and 43% (3/7) for tumors involving ⩾1/2, between 1/4 and 1/2, and <1/4 of the circumference at the dentate line, respectively. No recurrence was observed after initial improvement, with a median observation period of 35 months.
Conclusion:
ESD may be an effective treatment for internal hemorrhoids.
Introduction
Endoscopic submucosal dissection (ESD) is a reliable option for resecting intestinal intraepithelial neoplasia, regardless of the tumor size.1,2 However, due to limited working space, sphincter contractions and intraoperative bleeding caused by the presence of the hemorrhoidal plexus, performing ESD for rectal tumors adjacent to the dentate line is technically challenging. Despite these challenges, recent advancements in ESD techniques, equipment, and devices have enabled the safe and effective performance of the procedure, even in such challenging cases.3–5 Although improvement in hemorrhoids is frequently observed after ESD, comprehensive reports investigating the direct contribution of ESD to this improvement are lacking. This study aimed to evaluate the effectiveness of rectal ESD for the management of internal hemorrhoids.
Methods
A total of 3656 consecutive patients with 3851 colorectal tumors underwent colorectal ESD at the Hiroshima GI Endoscopy Research Group from January 2008 to December 2018. From this cohort, 34 patients with 34 tumors located adjacent to the dentate line and associated with internal hemorrhoids were recruited across 7 institutions. Of these, 11 patients were lost to follow-up. Finally, 23 patients who underwent follow-up colonoscopy after ESD, allowing for the assessment of changes in the degree of hemorrhoids, were enrolled in this study.
In this retrospective study, improvement in internal hemorrhoids was assessed by reviewing endoscopic images obtained during follow-up colonoscopy. The evaluation was qualitative, focusing on visible changes in hemorrhoidal swelling or prolapse. A validated grading system, such as the Goligher classification, and symptom-based scoring or proctological examination data were not available. Instead, hemorrhoid severity was classified as none, mild, or severe according to a previous report. 5 Downgrading at the scarring area after ESD and across the entire anorectal area was defined as focal and complete improvement, respectively. Histology was categorized as adenoma, intramucosal (Tis) carcinoma, and submucosal invasive (T1) carcinoma, according to the criteria outlined in the Japanese Classification of Colorectal, Appendiceal, and Anal Carcinomas. 6 Severe intraoperative bleeding was defined as the occurrence of more than five active bleeds requiring hemostatic forceps. Postoperative bleeding was defined as any apparent bleeding event. Stenosis was defined as the inability to pass the colonoscope or patient-reported difficulty in defecation.
The devices and methods used were almost identical to those previously reported. 5 Key points included the following: 1% lidocaine was locally injected into the anal canal for analgesic purposes before the usual submucosal injection and mucosal incision; blood vessels and active bleeding during submucosal dissection were appropriately coagulated using hemostatic forceps; and prophylactic coagulation of blood vessels in the ulcer bed was thoroughly performed after resection using hemostatic forceps.
This study was conducted in accordance with the Declaration of Helsinki, and written informed consent was obtained from all patients. The study protocol was approved by the institutional review boards of the participating hospitals and was registered in the University Hospital Medical Network Clinical Trials Registry (UMIN000016197).
This study was conducted and reported in accordance with the STROBE (Strengthening the Reporting of Observational Studies in Epidemiology) statement. As this was a retrospective exploratory study, no formal sample size calculation was performed.
Results
The clinical characteristics and outcomes of ESD are summarized in Table 1. Most patients (20/23, 87%) had mild hemorrhoids. En bloc and R0 resections were achieved in all patients, with a mean procedure time of 94 min. One patient experienced postoperative bleeding, which was successfully managed using endoscopic hemostasis. Another patient required three sessions of balloon dilation for postoperative stenosis.
Clinical characteristics and the outcome of endoscopic submucosal dissection.
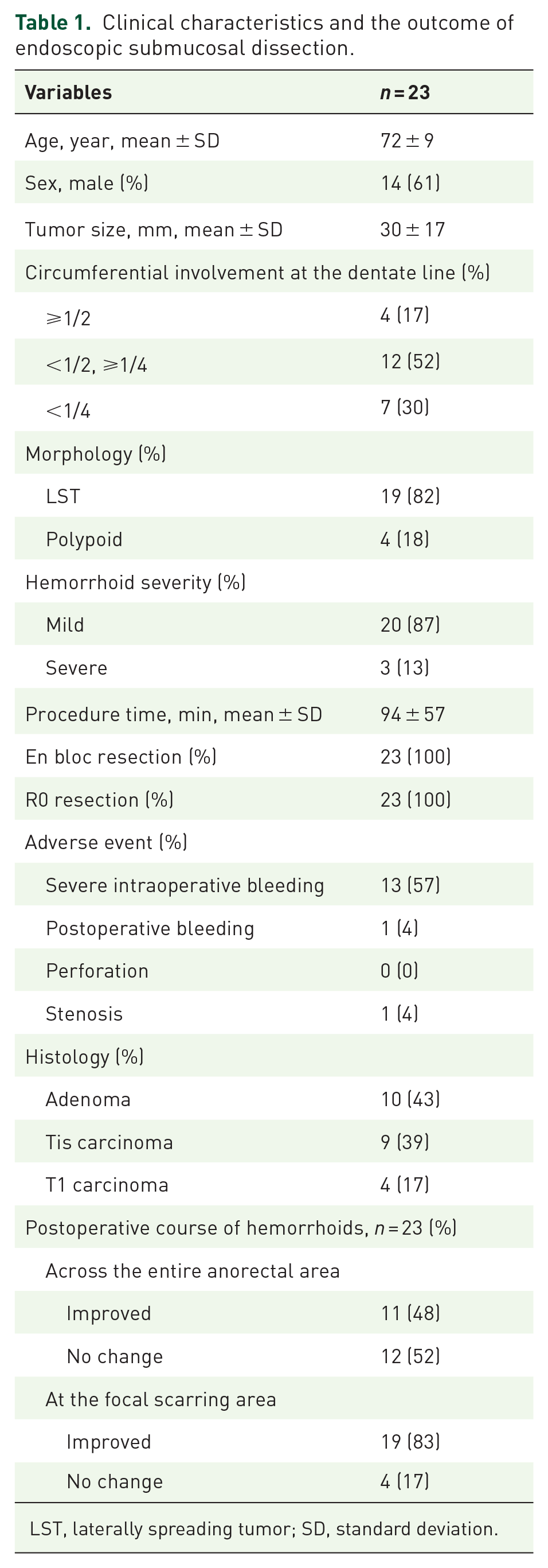
LST, laterally spreading tumor; SD, standard deviation.
Focal and complete improvement of hemorrhoids was observed in 83% and 48% of patients, respectively (Figure 1). All three patients with severe hemorrhoids achieved complete improvement. Complete improvement rates were 75% (3/4), 42% (5/12), and 43% (3/7) for tumors involving ⩾1/2, between 1/4 and 1/2, and <1/4 of the circumference at the dentate line, respectively. The median observation period was 35 months (range, 3–108 months), with no recurrence or progression of hemorrhoids observed after initial improvement.

Three representative cases of LSTs adjacent to the dentate line with mild internal hemorrhoids. (a–c) A 25-mm LST resected by ESD. Complete resolution of hemorrhoids was observed at 60-month follow-up. (d–f) A 25-mm LST resected by ESD. Focal improvement in hemorrhoids was observed at 78-month follow-up. (g–i) A 20-mm LST resected by ESD. Focal improvement in hemorrhoids was observed at 87-month follow-up.
Discussion
Our findings indicate that most patients exhibited improvement in hemorrhoids after rectal ESD. This improvement may be attributed to the cutting and sealing of the submucosal vessels associated with hemorrhoids during the procedure, suggesting that ESD, unlike endoscopic mucosal resection, is the only effective approach. 4 In addition, prophylactic coagulation of residual blood vessels in the ulcer bed after resection may further enhance this effect. Another contributing factor may be the submucosal fibrosis that accompanies mucosal healing, which inhibits angiogenesis and vascular regeneration. These mechanisms suggest that the effectiveness of ESD for hemorrhoids is influenced by the circumference of resection at the dentate line. In the present study, complete improvement was more frequently observed in cases involving ⩾1/2 of the circumference at the dentate line than in those involving smaller resection areas. Furthermore, circumferential or near-circumferential resection reportedly contributes to the complete healing of hemorrhoids. 4 Conversely, partial excision could theoretically exacerbate hemorrhoids around the scar owing to altered blood flow. Although we observed no such cases, incomplete healing of the hemorrhoids was observed in some cases. This incomplete healing may be partly because the primary goal of the patients in this study was tumor resection rather than hemorrhoid treatment. Therefore, sufficient circumferential resection to fully address the hemorrhoids was not performed. More extensive circumferential resection, particularly targeting hemorrhoids, could have led to better outcomes.
Surgical treatments, including excisional and non-excisional methods, are typically performed for severe hemorrhoids; however, adverse events, such as bleeding, stenosis, and postprocedural pain, particularly with excisional methods, remain problematic. Therefore, office-based, less-invasive treatment options, such as rubber band ligation, infrared coagulation, and injection sclerotherapy, have become available and standardized for mild hemorrhoids.7,8 These treatments have recently been performed using an endoscope rather than an anoscope. 9 ESD offers a similarly less invasive approach. Moreover, the recurrence rate of conventional options has been reported to be approximately 3.3%–16.9%.8,9 Conversely, no cases of recurrence were observed after initial improvement in the present study, suggesting that ESD is not only a less invasive but may also be more effective for at least mild hemorrhoids compared with the conventional options.
This study has some limitations. First, this was a single-arm retrospective study with a small sample size that examined the secondary effects of ESD on hemorrhoids. Moreover, a control group, such as patients undergoing ESD for proximal lesions with coexisting hemorrhoids, was not included. We fully acknowledge that a comparative analysis could have strengthened the interpretation of our findings. However, due to the retrospective nature of our study, hemorrhoid status was not consistently documented in non-lower rectal ESD cases, making meaningful comparison infeasible. Second, although all eligible cases during the study period were recruited, the final analysis was limited to patients who underwent follow-up colonoscopy. This may have introduced attrition bias, as patients who were lost to follow-up might differ from those included in the analysis. Third, the severity of hemorrhoids in this study was mild in most cases; therefore, their efficacy in more severe cases remains unclear. Furthermore, the evaluation of hemorrhoids was based solely on retrospective endoscopic image review, without the use of validated classification systems or symptom-based assessments. Therefore, the association between endoscopic improvement and clinical symptom relief could not be determined.
Conclusion
ESD may be an effective treatment for hemorrhoids and could be included as one of the treatment options available. Further comparative studies with a sufficiently large number of patients are necessary to confirm our findings.
Supplemental Material
sj-docx-1-tag-10.1177_17562848251355710 – Supplemental material for Effectiveness of endoscopic submucosal dissection in the management of internal hemorrhoids: a retrospective cohort study
Supplemental material, sj-docx-1-tag-10.1177_17562848251355710 for Effectiveness of endoscopic submucosal dissection in the management of internal hemorrhoids: a retrospective cohort study by Hidenori Tanaka, Toshio Kuwai, Shinji Nagata, Naoki Asayama, Yuko Hiraga, Tomohiko Kohno, Yuzuru Tamaru, Masaki Kunihiro, Koki Nakamura, Ken Yamashita, Yoshihiro Kishida and Shiro Oka in Therapeutic Advances in Gastroenterology
Footnotes
References
Supplementary Material
Please find the following supplemental material available below.
For Open Access articles published under a Creative Commons License, all supplemental material carries the same license as the article it is associated with.
For non-Open Access articles published, all supplemental material carries a non-exclusive license, and permission requests for re-use of supplemental material or any part of supplemental material shall be sent directly to the copyright owner as specified in the copyright notice associated with the article.