
Abstract
Background:
Endoscopic submucosal dissection (ESD) for early gastric neoplasms is still a technically difficult and time-consuming procedure. Hybrid ESD (H-ESD) involves circumferential incision with partial submucosal dissection combined with subsequent mucosal resection by snaring, wherein the newly developed device allows us to perform H-ESD using a single device. This study aimed to determine the clinical outcomes of H-ESD compared with conventional ESD (C-ESD) for early gastric neoplasms.
Methods:
In this multi-center, retrospective study, using propensity score-matched analysis, we reviewed the charts of patients with early gastric neoplasms smaller than 20 mm treated with H-ESD or C-ESD at three hospitals between January 2017 and October 2018. The primary outcome was the procedure time, and the secondary outcomes were other factors, including the en bloc resection rate, complete resection rate, curative resection rate, and rate of adverse events.
Results:
Among 215 patients, 29 underwent H-ESD and 186 underwent C-ESD; 29 pairs were created by propensity score matching. In the H-ESD group, 82.8% of lesions met the absolute indication [mucosal lesions limited to 20-mm diameter, dominated by differentiated adenocarcinoma without ulcer (scar)] for endoscopic resection (ER). As a result, the procedure time of H-ESD was significantly shorter than that of C-ESD [20 (interquartile range, 12–27) min versus 40 (30–50) min; p < 0.001]. There was no significant difference in the secondary outcomes between the two groups.
Conclusion:
H-ESD contributed to reduced procedure time. Therefore, H-ESD could be an alternative endoscopic treatment for gastric neoplasms when the lesion fulfils the absolute indication for ER.
Background
Endoscopic mucosal resection (EMR) was originally developed as an endoscopic treatment alternative to invasive surgery for early gastric neoplasms (EGN), with a negligible risk of lymph node metastasis and improved quality of life for patients. 1 EMR is applied to lesions that meet the absolute indication: mucosal lesions smaller than 20 mm, dominated by differentiated adenocarcinoma, and not accompanied by ulcer (scar).2,3 Although EMR is a simple and useful technique, the problem of curability still remains. 4 In previous studies, the en bloc resection rate was not satisfactorily high enough, especially when it was applied to lesions larger than 20 mm and/or with ulcer (scar).4–7 In this situation, endoscopic submucosal dissection (ESD) has been developed to overcome these problems, and it has been shown to achieve a considerably high rate of en bloc resection even for larger or ulcerative lesions, 8 which enables us to make clear pathological diagnoses. ESD can be applied to the lesions with expanded indications,9–11 and it has become a gold standard of endoscopic treatment for EGN, facilitated by the development of the various ESD devices. However, the problem is that ESD for EGN is technically more difficult and time-consuming, with higher rates of adverse events, including perforation and bleeding, than EMR.6,12,13
Hybrid ESD (H-ESD) is the procedure of circumferential incision with partial submucosal dissection combined with subsequent mucosal resection by snaring. H-ESD is, thus, an intermediate technique between conventional ESD (C-ESD) and EMR, which can combine the merits both of ESD and EMR. More recently, a novel multifunctional device for H-ESD called SOUTEN (Kaneka Medics, Tokyo, Japan) was invented (Figure 1). It combines the feature of a needle-type tip and a snare, enabling us to perform the procedure of H-ESD more easily with this single device. 14

Image of the multifunctional device.
Although H-ESD for EGN would have more advantages over C-ESD in terms of procedure time and complication risk, evidence on these aspects is still lacking. Thus, the objective of the present study was to determine the differences in clinical outcomes between H-ESD and C-ESD with lesions smaller than 20 mm using propensity score matching analysis.
Methods
Study design and ethics
This was a retrospective, multi-center, observational cohort study conducted at Nihon University School of Medicine Surugadai Hospital, Nihon University School of Medicine Itabashi Hospital, and Yuri-Kumiai General Hospital. We assessed the ESD database and reviewed the endoscopic reports and medical records, and obtained the necessary medical information and clinical outcomes of the ESD procedures. Written informed consent for endoscopic treatment was obtained from each patient. The study protocol was approved by the Institutional Review Board of Nihon University School of Medicine Surugadai Hospital, Nihon University School of Medicine Itabashi Hospital and Yuri-Kumiai General Hospital. The approval number was 20180904.
Patients
From January 2017 to October 2018, 285 patients with gastric tumors underwent endoscopic resection (ER) at three hospitals. Eight patients with non-neoplastic lesions, four patients treated for multiple lesions, and one patient with postoperative stomach lesions were excluded. ESD in the postoperative stomach was considered to be more difficult than that in non-operative stomach. 15 Subsequently, 57 patients were excluded as their lesions were 20 mm or larger in diameter. Finally, 215 remaining patients with EGN lesions smaller than 20 mm, who underwent either C-ESD or H-ESD, were included in this study. H-ESD was performed in 29 patients, and C-ESD was performed in 186 patients (Figure 2).

A flow chart of enrollment of the patients in the present study. Initially, 285 patients with gastric neoplasms were reviewed. Finally, data from 215 patients were analyzed in the present study.
ESD
All ESD procedures, including C-ESD and H-ESD, were conducted under intravenous sedation with midazolam and pentazocine hydrochloride with a standard single-channel endoscope (GIF-Q260J; Olympus Optical, Tokyo, Japan). A transparent cap was attached to the distal end of the endoscope. VIO 300D, ICC200 (ERBE Elektromedizin GmbH, Tübingen, Germany), or ESG100 (Olympus Optical, Tokyo Japan) was used as an electrical power unit.
Conventional ESD
C-ESD was performed as previously described.16,17 In brief, circumferential marking dots were placed using the tip of an endo-knife. A solution of mixed hyaluronate and a small amount of indigocarmine was injected into the submucosa to lift the lesion and secure a safe area for dissection of the submucosa. Then, a circumferential mucosal incision around the marking dots was made, and the submucosal layer was dissected out using an endo-knife. Several endo-knives, including needle-type knife, insulated tip knife, and scissor-type, were used according to the preference of attending endoscopists.16,18,19 The procedure-related bleeding was stopped by coagulation with the endo-knife itself or hemostatic forceps.
Hybrid ESD
H-ESD was performed with the newly developed SOUTEN, which enabled us to complete the procedure with one device. The technical steps of H-ESD are shown in Figure 3. In brief, a circumferential mucosal incision, followed by partial submucosal dissection, was performed using a needle-tip attached to the end of a snare in a manner similar to C-ESD. The procedure of submucosal dissection was continued until the point at which the attending operator judged that the lesion could be snared successfully. After completing the planned submucosal dissection, the lesion was resected by snaring in a manner similar to EMR.
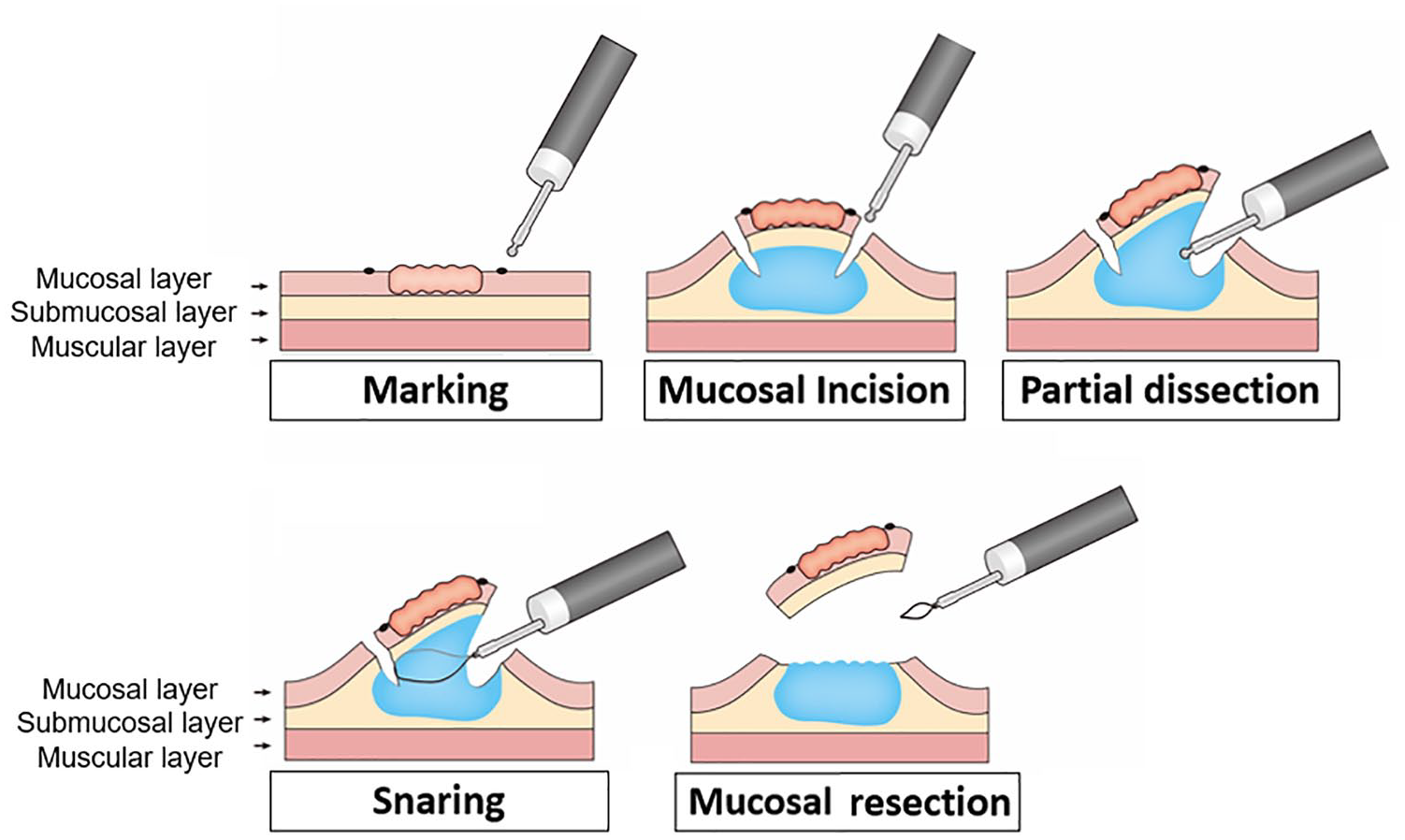
The procedures of H-ESD. (A–E) The schemas show each step of the H-ESD procedure: marking (A), mucosal incision (B), partial dissection (C), snaring (D), and mucosal resection (E).
Histopathological evaluation
After removal, ESD specimens were fixed in 10% formalin. The specimens were embedded in 10% paraffin, sectioned at 2-mm intervals, and stained with hematoxylin and eosin. Pathological diagnoses and evaluation of curability were made by the experts in gastrointestinal pathology according to the Japanese Gastric Cancer Classification and Japanese gastric cancer treatment guidelines.3,20
Clinical outcomes
The primary outcome was the procedure time, which was defined as the time from the start of mucosal incision to the completion of resection of the lesion. In addition, the secondary outcomes were the en bloc resection rate, complete resection rate, curative resection rate, and adverse events (perforation and/or delayed bleeding). En bloc resection was defined as resection in a single piece, as opposed to piecemeal resection in multiple pieces. Complete resection was defined as en bloc resection with horizontal and vertical margins free of tumor. Curative resection was defined as complete resection with curative intention according to the guideline. 3 Perforations were defined as a visible break of the gastric wall confirmed by endoscopy or free air confirmed by radiography or computed tomography scanning. Delayed bleeding was defined as clinical evidence of bleeding after ESD that required endoscopic hemostasis or transfusions. Endoscopists were divided into two categories: trainees and experts. Endoscopists having experience of no less than both 50 ESD procedures and 50 EMR procedures in gastrointestinal tract tumors were defined as experts. The others were defined as trainees. There was no specific training for H-ESD because H-ESD required a combined technique between EMR and ESD.
Statistical analysis
The sample size of this study could not be calculated because this was a retrospective study. Furthermore, this was not a randomized control study. There were confounding differences between the two groups, which might have influenced the treatment outcomes of this study. Therefore, propensity score matching was adopted to compensate for the confounding bias.21–23 Logistic regression of the following factors with endoscopic procedures (H-ESD versus C-ESD) and calculation of propensity score were conducted for: age (years), sex (male/female), location (upper third of the stomach/others), position (lessor curvature/others), shape (protruded/others), size (mm), depth (mucosa/submucosa), histology (differentiated/undifferentiated), ulcer (presence/absence), and operator skill (expert/trainee). This model yielded an area under the receiver operating characteristics curve of 0.69, which indicated a good predictive power. The propensity score for H-ESD was calculated using logistic regression analysis, which represented the possibility that a patient would undergo H-ESD. After estimating the propensity scores, patients in the H-ESD group were matched to patients in the C-ESD group. The matching algorithm used calipers with a width equal to one-quarter of the standard deviation (SD) of the log of the propensity score without replacement. The effect of the matching was evaluated in terms of the absolute standardized difference.
Continuous variables distributed non-normally were presented as median and interquartile range (IQR). The differences in the baseline clinicopathological characteristics and treatment outcomes of this study were compared between the two groups using the Fisher’s exact test for categorial data, or the Mann–Whitney U test for non-normally distributed continuous data. p < 0.05 was considered statistically significant for all tests. All statistical data analyses were performed using JMP Pro 13.0 software (JMP, Marlow, UK).
Results
Baseline clinicopathological characteristics of the patients before matching
All 29 patients for the H-ESD group and 186 patients for the C-ESD group completed their planned procedure. No patient was transferred from C-ESD to H-ESD or from H-ESD to C-ESD. The baseline clinicopathological characteristics of the patients (29 for H-ESD group and 186 for C-ESD group) finally enrolled in the present study are shown in Table 1. The median age of patients in the H-ESD group tended to be higher than that in C-ESD group, but it did not reach statistical significance. There was no significant difference in other factors between the two groups. As for histological types, the proportions of differentiated type in the H-ESD and C-ESD groups were 100% (29/29) and 92.5% (172/186), respectively. Regarding tumor depth, the proportions of lesions with submucosal invasion in the H-ESD and C-ESD groups were 10.3% (3/29) and 12.9% (24/186), respectively. As for the presence of ulceration, the proportion of the lesions with ulceration in H-ESD and C-ESD groups were 10.3% (3/29) and 10.8% (20/186), respectively. As a result, 82.4% (24/29) of lesions in the H-ESD group and 73.1% (136/186) in the C-ESD group met the absolute indication.
Comparison of baseline clinicopathological characteristics between the H-ESD and C-ESD groups.
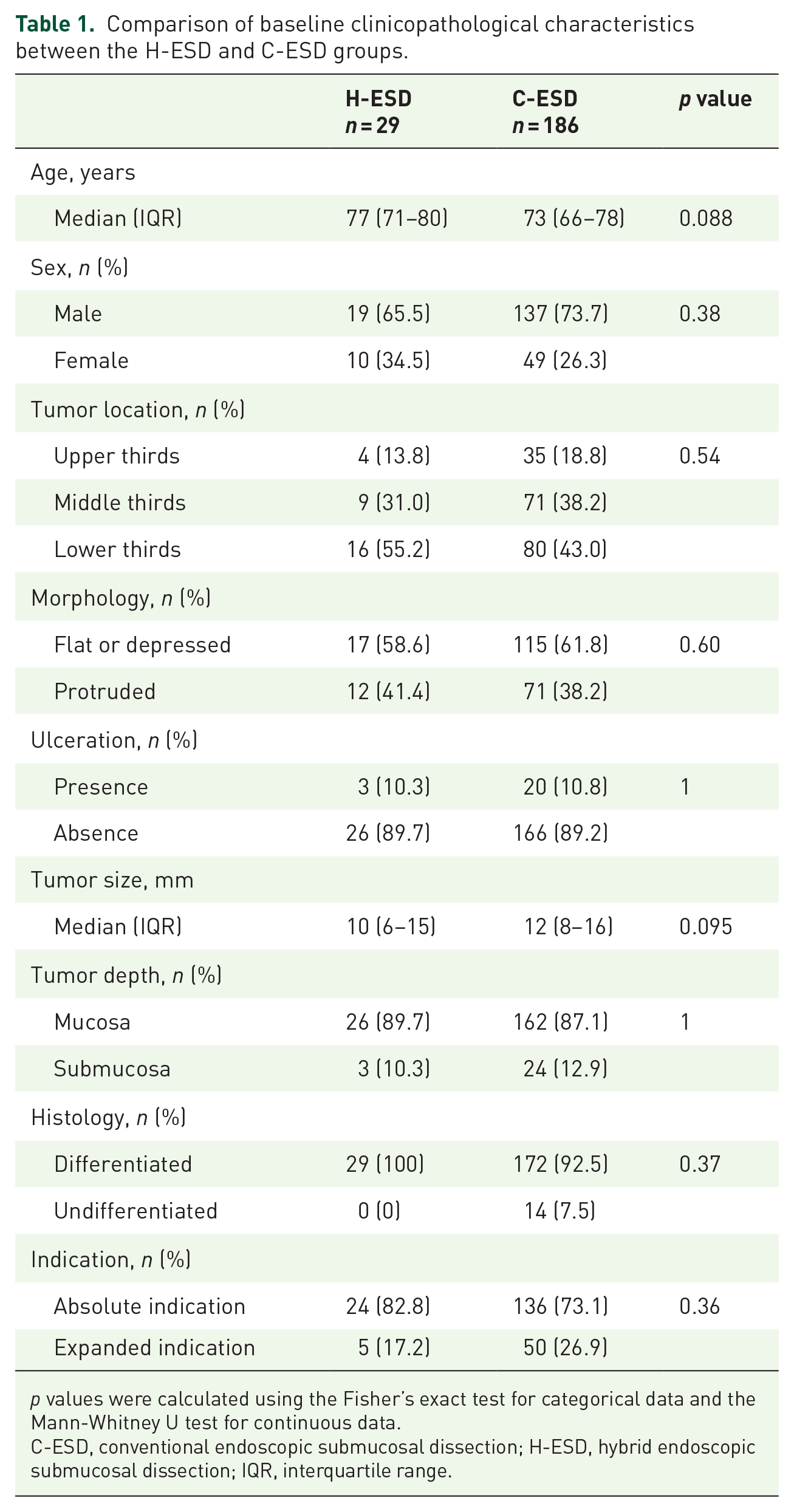
p values were calculated using the Fisher’s exact test for categorical data and the Mann-Whitney U test for continuous data.
C-ESD, conventional endoscopic submucosal dissection; H-ESD, hybrid endoscopic submucosal dissection; IQR, interquartile range.
Comparison of treatment outcomes between H-ESD and C-ESD
The treatment outcomes, before propensity score matching, are shown in Supplemental Table S1. The results suggested that the median procedure time of the H-ESD group [20.0 min, (12.0–27.0)] was shorter than that of the C-ESD group [43.5 min, (30.0–62.0)] (p < 0.001). It seemed that there was no difference in the other outcomes between the two groups.
All 29 patients in the H-ESD group could be matched with patients in the C-ESD group by propensity score matching. The clinicopathological characteristics after matching between the two groups are shown in Table 2, which were quite similar without any significant differences. The matching of the two groups was considered to be well-balanced, with the absolute standardized differences of all factors ranging between ±1.96√2/n. 24
Comparison of clinicopathological characteristics of the patients between H-ESD and C-ESD after propensity score matching.

p values were calculated using the Fisher’s exact test for categorical data and the Mann-Whitney U test for continuous data.
ASD, absolute standardized difference; C-ESD, conventional endoscopic submucosal dissection; H-ESD, hybrid endoscopic submucosal dissection; IQR, interquartile range; U/M or L, upper/middle or lower third.
The treatment outcomes of H-ESD and C-ESD after matching are summarized in Table 3. The median procedure time of H-ESD [20 min, (12–27)] was significantly shorter than that of C-ESD [40 min, (30–50)] (p < 0.001). This indicated that a nearly 50% reduction in procedure time could be achieved by H-ESD compared with C-ESD. Furthermore, lesions with a procedure time longer than 40 min were significantly fewer in H-ESD than in C-ESD (3.4% versus 48.3%, p < 0.001). There was no significant difference in other treatment outcomes between the two groups. The en bloc resection, complete resection, and curative resection rates of H-ESD were 100%, 100%, and 96.6%, respectively, while those of C-ESD were 100%, 93.1%, and 93.1%, respectively. As for adverse events, neither perforation nor delayed bleeding was observed in the H-ESD group. Although perforation was not observed in C-ESD, delayed bleeding occurred in one patient, which was successfully managed conservatively without surgery.
Comparison of treatment outcomes between the H-ESD and C-ESD groups after propensity score matching.

p values were calculated using the Fisher’s exact test for categorical data and the Mann-Whitney U test for continuous data.
C-ESD, conventional endoscopic submucosal dissection; H-ESD, hybrid endoscopic submucosal dissection; IQR, interquartile range.
Discussion
In the present study, we compared the efficacy and safety of H-ESD and C-ESD for EGN using propensity score matching. We have shown for the first time that H-ESD yielded a significantly shorter procedure time than C-ESD, without any increase in adverse events, when the lesions were smaller than 20 mm. Therefore, H-ESD can be selected for endoscopic treatment of EGN that fulfilled the absolute indication for ER according to Japanese guidelines.
In previous reports, including a meta-analysis of endoscopic treatment for EGN, it was shown that the procedure time was significantly longer, and the complication rates, including perforation and postoperative bleeding, were significantly higher in C-ESD than those in EMR. The mean procedure time, postoperative bleeding, and intraoperative perforation rate in C-ESD reached up to 93.9 min, 15.6%, and 5.3%, respectively. 25 Recently, a multicenter prospective study of gastric ER, which showed real-world evidence in Japan, showed favorable short-term outcomes. 26 ESD consisted of 99.4% of ERs for EGN. Postoperative bleeding and intraoperative perforation were reduced in 4.4% and 2.3% of patients, respectively. However, the mean procedure time was still 91.4 min. Although the treatment outcomes, including en bloc resection rate, complete resection rate, curative resection rate, and adverse event rate for C-ESD, have been satisfactory enough owing to the development of ESD devices and improvement of endoscopic skills, the problem with long procedure time is yet to be resolved. For this reason, the procedure time was set as the primary outcome of the present study. We showed that the procedure time was significantly shorter in H-ESD than in C-ESD.
The en bloc resection rate in EMR decreases with larger lesions. 6 The en bloc resection rate of EMR was significantly lower than that of ESD, especially for lesions larger than 10 mm.4,6 In contrast, according to Japanese guidelines, the absolute indication of EMR or ESD for EGN is as follows: a differentiated-type adenocarcinoma without ulcerative findings, a T1a depth of invasion diagnosed clinically, and a 20-mm diameter. 3 In fact, the snare size of the multifunctional device used in the present study was not large enough to perform an en bloc resection for lesions larger than 20 mm. Thus, we determined that the EGNs that fulfilled the absolute indications per the Japanese guidelines were eligible for H-ESD in the present study. As a result, the horizontal and vertical margins of all lesions were both negative for any neoplastic component, while 100% en bloc and complete resection rate was achieved by H-ESD. However, lesions larger than 20 mm may be subjected to H-ESD when partial submucosal dissection is sufficient for snaring. Therefore, the indication of H-ESD should be further explored in future studies, especially considering lesion size.
Several clinicopathological factors, including tumor size, tumor location, tumor position, presence of ulceration (scar), tumor depth, tumor histology, and operator skill, are reported to be associated with the difficulty and adverse events of ESD.27–32 Before propensity score matching, there were no significant differences in the baseline of those factors between H-ESD and C-ESD groups. In this condition, the procedure time of H-ESD was significantly shorter than that of C-ESD (Supplemental Table S1). However, the median age of H-ESD tended to be older than that of C-ESD (p = 0.088), and the median tumor size of H-ESD tended to be smaller than that in C-ESD (p = 0.095). Thus, it was possible that some of those factors affected the treatment outcomes of the study. Therefore, propensity score matching was adopted to reduce the confounding bias between the two groups. As a result, the superiority of H-ESD over C-ESD in the procedure time could be also observed after propensity score matching in the present study.
H-ESD was originally invented as a rescue treatment for colorectal neoplasms in which endoscopists faced technical difficulties in continuing the procedure of C-ESD. The safety and efficacy of H-ESD for colorectal neoplasms as a rescue therapy have been reported previously. 33 The procedure time of H-ESD was significantly shorter than that of C-ESD, although H-ESD was applied only to colorectal neoplasms with difficulties in the ESD procedure. It was also reported that there were no significant differences in the en bloc resection rate, perforation rate, and bleeding rate between H-ESD and C-ESD, and local recurrence did not occur in any case. Therefore, the planned H-ESD, not a rescue H-ESD, has been applied for colorectal neoplasms, where superior clinical outcomes were obtained compared with C-ESD.33,34 Later, H-ESD was also applied to EGN; however, a previous report could not prove the superiority in the in the procedure time of H-ESD. 35 There was a limitation that a snare tip for polypectomy was used for both ESD and H-ESD procedures, which might not be suitable for mucosal incision or submucosal dissection, and the sample size was quite small. Therefore, it could not demonstrate shorter procedure time of H-ESD compared with C-ESD. In this situation, the recently developed multifunctional device could influence the treatment outcomes of H-ESD as previously reported. 36 Thus, we conducted the present study to compare the treatment outcomes between H-ESD using a multifunctional device and C-ESD, wherein H-ESD was applied as a first-line therapy and not as a rescue therapy. The findings have shown that the treatment outcomes of H-ESD using a multifunctional device are sufficient for its consideration as a first-line endoscopic treatment for EGN. Considering H-ESD as a first-line endoscopic treatment, it is important to consider not only treatment outcomes, such as procedure time, but also the total cost of the procedure. When H-ESD-related procedures, including mucosal incision, submucosal dissection, and snaring, were performed using more than one device, similar to rescue H-ESD, the total cost of H-ESD was higher than that of C-ESD. 33 The problem was solved by the development of a multifunctional device allowing us to complete all procedures with a single device. In fact, the SOUTEN used in the present study is less expensive than a conventional endo-knife, which contributes to the reduction of the medical cost for H-ESD. 36 Taken together, compared with C-ESD, H-ESD using a multifunctional device yields not only comparable treatment outcomes but also cost-saving in the endoscopic treatment of EGN smaller than 20 mm.
The precutting EMR technique has already been applied to the gastrointestinal tract tumors including gastric neoplasms.37,38 This technique is defined as circumferential mucosal incision followed by snaring without any submucosal dissection. However, H-ESD includes the procedure of partial submucosal dissection, which assist in resecting the lesion completely. The complete resection rate was reported as 75.7–90.2% in precutting EMR for gastric neoplasms.39,40 In this study, 100% complete resection rate was achieved by adding partial submucosal dissection. Therefore, a higher rate of complete resection might be achieved in H-ESD than that in precutting EMR for gastric neoplasms.
Some limitations were associated with the present study. First, this was a retrospective study and not a study involving a randomized population. There was a possibility of selection bias, as lesions that were easy to snare were selected for H-ESD. Second, the sample size was relatively small, even though this was a multi-center study. Although 100% complete resection rate was achieved in H-ESD, and the procedure time of H-ESD was significantly shorter than that of C-ESD, this study did not prove a non-inferior outcome in curability and safety of H-ESD against C-ESD due to the small sample size. Therefore, a multi-center prospective study with a larger population should be conducted to clarify this point in future. Third, the indication for H-ESD was limited to lesions smaller than 20 mm, which met the absolute indication of ER led by the Japanese guidelines. Therefore, the treatment outcomes of the present study could not be applied to EGN beyond the absolute indication: larger size than 20 mm, submucosal invasion, poorly differentiated component, and ulcers (scar). Third, this study included only short-term outcomes of H-ESD or C-ESD. Long-term outcomes, such as the rate of residual lesions or recurrent lesions, were not included in this study. Although an extremely low rate of residual or recurrent lesions are estimated due to 100% complete resection rate for H-ESD, a further study should also include the long-term outcomes.
In conclusion, the procedure time of H-ESD using a multifunctional device was significantly shorter than that of C-ESD, although there were no differences in the curability and adverse events between H-ESD and C-ESD for lesions smaller than 20 mm. Therefore, H-ESD could be an alternative endoscopic treatment of EGN when the lesion fulfils the absolute indication for ER.
Supplemental Material
TAG939420_Supplemental_Table_1_CLN – Supplemental material for Reduction in the procedure time of hybrid endoscopic submucosal dissection for early gastric neoplasms: a multi-center retrospective propensity score-matched analysis
Supplemental material, TAG939420_Supplemental_Table_1_CLN for Reduction in the procedure time of hybrid endoscopic submucosal dissection for early gastric neoplasms: a multi-center retrospective propensity score-matched analysis by Mitsuru Esaki, Sho Suzuki, Toshiki Horii, Ryoji Ichijima, Shun Yamakawa, Hitoshi Shibuya, Chika Kusano, Hisatomo Ikehara and Takuji Gotoda in Therapeutic Advances in Gastroenterology
Footnotes
Acknowledgements
We thank Hiroko Fujisawa for helping with illustration.
Author contributions
ME, SS: Study concept and design, drafting of the article
TH, RI, SY, HS, CK, HI: Data collection, analysis of the data
SS, TG: Critical revision of the article
Conflict of interest statement
Mitsuru Esaki, Sho Suzuki, Toshiki Horii, Ryoji Ichijima, Shun Yamakawa, Hitoshi Shibuya, Chika Kusano, Hisatomo Ikehara, and Takuji Gotoda have no conflicts of interest or financial ties to disclose.
Funding
The authors received no financial support for the research, authorship, and/or publication of this article.
Supplemental material
Supplemental material for this article is available online.
References
Supplementary Material
Please find the following supplemental material available below.
For Open Access articles published under a Creative Commons License, all supplemental material carries the same license as the article it is associated with.
For non-Open Access articles published, all supplemental material carries a non-exclusive license, and permission requests for re-use of supplemental material or any part of supplemental material shall be sent directly to the copyright owner as specified in the copyright notice associated with the article.