
Abstract
Background:
About half of the patients having colonoscopies experience procedure-related anxiety and emotional distress, which are associated with negative outcomes, including pain, higher sedation needs, longer procedure times, and avoidance of future care.
Objectives:
To improve procedure quality, we sought to understand from the patient’s perspective the emotional and psychological aspects of undergoing a colonoscopy and recommendations for improving care.
Design:
Qualitative interview study.
Methods:
We conducted semi-structured interviews with patients after colonoscopy. Questions were informed by the theoretical frame of trauma-informed care and fieldwork and collaborative discussions with endoscopists, multidisciplinary staff, and patients. Patients were recruited through purposive sampling to reflect a range of indications for colonoscopy, demographics, and health backgrounds. Interviews and data analysis were conducted in overlapping phases to ensure a diversity of perspectives. Thematic analysis was used to identify shared patterns across the data.
Results:
Nine patients completed interviews, and analysis generated the central dialectic “it’s a tool, it’s got hardships,” reflecting a shared belief that colonoscopies are both stressful and important to one’s health. Within this uniting concept, we identified themes of patient, provider, and process factors that have the potential to reduce or promote distress. Subthemes related to patients’ past experiences/expectations, coping, and access to support; providers’ communication and behavior; and process factors including prep/wait times, sedation and anesthesia, and team-based care. Factors that buffered against distress included perceived trust, transparency, and confidence; positive expectations rooted in prior healthcare experiences; flexible coping and feeling supported. Factors that contributed to increased vulnerability included having a minoritized identity, a history of past medical trauma, and uncertainty in communication and the colonoscopy process.
Conclusion:
Efforts to improve the colonoscopy experience should continue to address the interplay of these complex factors. Given that identification of those at the highest risk for distress may not always be possible, we recommend a universal trauma-informed approach and provide specific suggestions for implementation in endoscopy.
Plain language summary
Colonoscopies are a common medical test for adults that diagnose digestive problems and detect colon cancer. About half of patients feel worried or upset about the procedure. Research shows that fear and distress can come from not knowing what to expect, past bad medical experiences, fear of pain or cancer, and feeling out of control. People with a history of trauma may find colonoscopies especially difficult, but providers may not know who these patients are or how to support them. We want to improve colonoscopies for all patients, including those with past trauma. To do this, we interviewed nine patients from diverse backgrounds (age, gender, medical histories, reason for the colonoscopy) about their experiences and asked them for suggestions to improve care. All of the patients felt that colonoscopies are important for their health, but also stressful. Their feelings were shaped by personal histories and expectations, providers’ actions, and the overall environment. Stress could occur at any point including scheduling, preparation, talking to the team, waiting for the procedure to start, sedation, and getting results. Patients felt better when they trusted their providers, had clear communication, used coping strategies, and felt supported. They felt worse when they were unsure what to expect or why something was happening, had trouble communicating, had past negative experiences, or identified as a gender minority. Patients had clear ideas for how colonoscopies can be improved. We recommend trauma-informed care for all patients, even if trauma history is not known. This means being aware that many people have experienced trauma and that it can affect how they feel and act in medical settings. Providers can reduce distress by giving clear information ahead of time, asking what patients need to feel safe, and checking in before, during, and after the procedure. While this may take extra effort, trauma-informed care benefits both patients and care teams.
Introduction
Endoscopic procedures are central to the prevention, diagnosis, and management of gastrointestinal disease. 1 In the United States, colonoscopies are common; over 60% of adults have undergone at least one colonoscopy in their lifetime. 2 However, systematic reviews also indicate that around half of the patients having these procedures experience moderate to severe endoscopy-related anxiety and emotional distress. 3 Patient experience is considered a key metric of procedure quality,4 –6 and anxiety and emotional distress are associated with a number of negative outcomes, including pain during the procedure,7,8 higher sedation needs, longer procedure times, 9 and avoidance of future care.10 –14 For select groups of patients, colonoscopies may even cause the onset of new posttraumatic stress symptoms or other psychological problems.15 –17
The sources of procedure-related anxiety are varied. Common worries relate to the process of the procedure (e.g., fear of the unknown, fear of embarrassment, fear of experiencing pain, and fear of sedation/losing control), the patient-provider relationship (e.g., perceived power imbalances, difficulty with self-advocacy), 18 and the outcome (e.g., discovery of pathology).3,19 –21 Certain demographic and situational factors, including female sex, younger age, and no previous colonoscopy experience, are all associated with higher rates of colonoscopy-related anxiety,3,20,22 as having undergone a painful procedure in the past. 23
In particular, patients with a history of psychological trauma are at especially high risk of difficult endoscopy experiences. 24 In gastroenterology (GI) patient populations, trauma exposure, and its psychological sequelae are common—trauma is a well-known risk factor for the development of irritable bowel syndrome and other disorders of gut-brain interaction,25,26 and has been associated with inflammatory bowel disease (IBD). 27 Further, trauma can arise specifically from disease-related experiences, such as hospitalizations and disease monitoring in IBD.28,29 In other medical contexts, trauma history has a complex relationship with healthcare access and engagement,30,31 and is associated both with overall increased healthcare utilization and decreased engagement with preventive care, particularly screens that may be experienced as invasive or retraumatizing (e.g., routine breast and cervical cancer screenings).32 –34 In endoscopy, this relationship may be different in patients with post-traumatic stress disorder (PTSD) and is more adherent to both screening and surveillance colonoscopies.35,36 However, exposure to past trauma is associated with higher sedation needs during endoscopy37 –39 and patients are more adherent to follow-up colonoscopies when the initial procedure is completed with general anesthesia.35,40 Importantly, this emerging research has been completed using electronic medical record (EMR) documentation, and the rates of PTSD in these datasets are much smaller than would be expected. As patients may or may not disclose their trauma histories to healthcare providers, even when prompted,41,42 shared decision-making is paramount when referring patients for and performing endoscopic procedures.
Although colonoscopies are considered routine and low-risk, many patients who need colonoscopies do not receive them (non-scheduling and no-show rates vary, but range from around 15% 14 to 50% 12 ), and half of the patients who do receive them report considerable distress. 3 Given the common and complex interactions between trauma and GI conditions,25,26,28 we initiated a qualitative study to better understand the colonoscopy experience from the patient perspective, which can shed light on complexities that are not reflected by surveys or medical record data. Our goal in conducting this project was to identify general experiences and needs from an initial sample of unique patients and to use this information to develop broadly applicable general recommendations for universal trauma-informed endoscopy care.
Methods
Approach
This study was nested within an overarching initiative to increase access to behavioral health services within a gastroenterology and hepatology department at a rural academic medical center. This redesign effort was conducted by a multidisciplinary team of gastroenterologists, psychologists, administrative and secretarial staff, a patient navigator, and a patient partner, and relied on a design thinking approach. Details of this effort have been published previously. 43 For this subproject, we sought to better understand patients’ needs specific to endoscopy procedures, as opposed to outpatient care. This manuscript was prepared in accordance with the Standards for Reporting Qualitative Research (SRQR; Supplemental Material). 44
Participant selection
Adult, English-speaking patients awaiting colonoscopies in preprocedure rooms at Dartmouth Hitchcock Medical Center were approached about this study. Patients were asked if they would be willing to participate in an interview as part of a quality improvement project to better understand the colonoscopy experience from the patient’s perspective. Patients were selected for recruitment through purposive sampling to reflect patients with a range of indications for colonoscopy (screening, diagnostic, and disease/symptom management), ages, and genders, past colonoscopy experiences, and psychiatric backgrounds. 45 Those who agreed to participate answered preliminary questions prior to their procedure (focused on their thoughts and feelings at that moment and expectations for the procedure) and scheduled a time for a follow-up phone interview (10–20 min) within 1 week of their procedure. Verbal consent was obtained before the initial screening and confirmed before the follow-up call. Follow-up calls were audio recorded and then transcribed.
Interview development
Broadly, interviews sought to understand the emotional and psychological aspects of undergoing a colonoscopy, the influence of past medical encounters on the current experience, and patients’ recommendations for improving care. A semi-structured interview guide was developed through an iterative process of pilot research and group discussion with the larger program redesign team. In preparation for the interview development, the first author spent time across several weeks observing and interacting with staff in the endoscopy suite and shadowing patients through the endoscopy process from the waiting room to discharge. During this phase of the project, the interviewer took contemporaneous field notes, but discussions were not recorded or included in formal data analysis. Following this initial investigation stage, the larger program redesign team identified important information domains (e.g., components of patient experience, colonoscopy history, and hopes for the future), drafted primary prompts and follow-up questions, and then reviewed these for clarity and acceptability. This process resulted in a semi-structured interview guide informed by patient and provider stakeholders.
Data analysis
The theoretical frame for this study was trauma-informed care (TIC), an approach to healthcare delivery that assumes that people’s behavior, including their interactions with the healthcare system, is driven by their past experiences, some of which might have been traumatic.46 –48 Data were analyzed using reflexive thematic analysis (TA), a theoretically flexible analytic approach to identifying and interpreting shared patterns of meaning within the data.49,50 In our analysis, we applied both deductive and inductive modes of interpretation. That is, we recognized that our analysis was influenced by our original frame of TIC and our expertise as both clinicians and researchers, and we also sought to center the lived experiences of the participants and the subjective meanings they ascribed to these experiences. 51 We elected to display our themes and representative quotations in a table for easy practical reference. 52
TA does not prescribe a particular sample size. 53 To support our goal of understanding broad perspectives while recognizing that there is no single typical patient during initial recruitment, we used a matrix to ensure that each patient reflected a unique combination of background factors (first vs repeat colonoscopy, colonoscopy indication, and gender) that, according to past research, are likely to shape patients’ perspectives. As interviews were ongoing, the first and senior authors met for a preliminary review of three interviews, reflecting unique colonoscopy histories and indications, to begin data familiarization and coding. Given strong concordance of coding, the first author then continued coding the remaining interview transcripts using the software program ATLAS.ti, 54 which extracted and organized coded segments. We conducted interviews and data analysis in several overlapping phases to ensure that this purposive critical case sampling strategy achieved the intended informational power, reflecting a diversity of patients undergoing colonoscopy. We continued until analyses ceased revealing new codes and thematic content relative to the initial analysis, a marker of saturation.55,56 All interviews were conducted by the first author, at the time a postdoctoral fellow in clinical psychology with a specialty emphasis on psychogastroenterology. Coded data and preliminary themes were reviewed with both the senior author and the second author, a gastroenterologist and endoscopist, and organized into an initial thematic map. To promote rigor in the interpretive process, this thematic map was also discussed at a multidisciplinary team meeting that included gastroenterologists, advanced practice providers, nurses, and administrative staff, all of whom were familiar with the TIC model. Demographic information, including relevant diagnoses and procedure indications, was abstracted from the EMR and confirmed with participants during interviews.
Results
Potential participants were approached by the first author on 6 different days between December 2022 and February 2023. Thirteen people agreed to be interviewed and completed preliminary preprocedure conversations, and nine completed follow-up calls within 1 week. The remaining four did not respond to follow-up within this window, which we imposed to ensure ecological validity with recent memories of the colonoscopy experience. Participant demographic characteristics are in Table 1.
Patient demographics.

During interviews, participants described their experiences before, during, and after their colonoscopy; related these to their overall health and prior interactions with the healthcare system; and considered how their own experiences might be similar and different from those of other people with different backgrounds. Our inductive-deductive analysis of the patient interviews suggested that most aspects of the procedure reflected an overarching theme that captured a tension or dialectic in patients’ experience: “It’s a tool, it’s got hardships.” That is, all patients viewed a colonoscopy as an important aspect of their healthcare with many benefits but also identified challenging aspects of the procedure. Within this central organizing concept, we identified subthemes that can be categorized as individual patient factors, provider factors, and structural/environmental factors. Finally, we split each subtheme to identify factors on each side of the dialectic: that is, the factors that improved the patient experience and those that increased the risk of distress. Themes, subthemes, and representative quotations are in Table 2.
Themes and representative quotations.
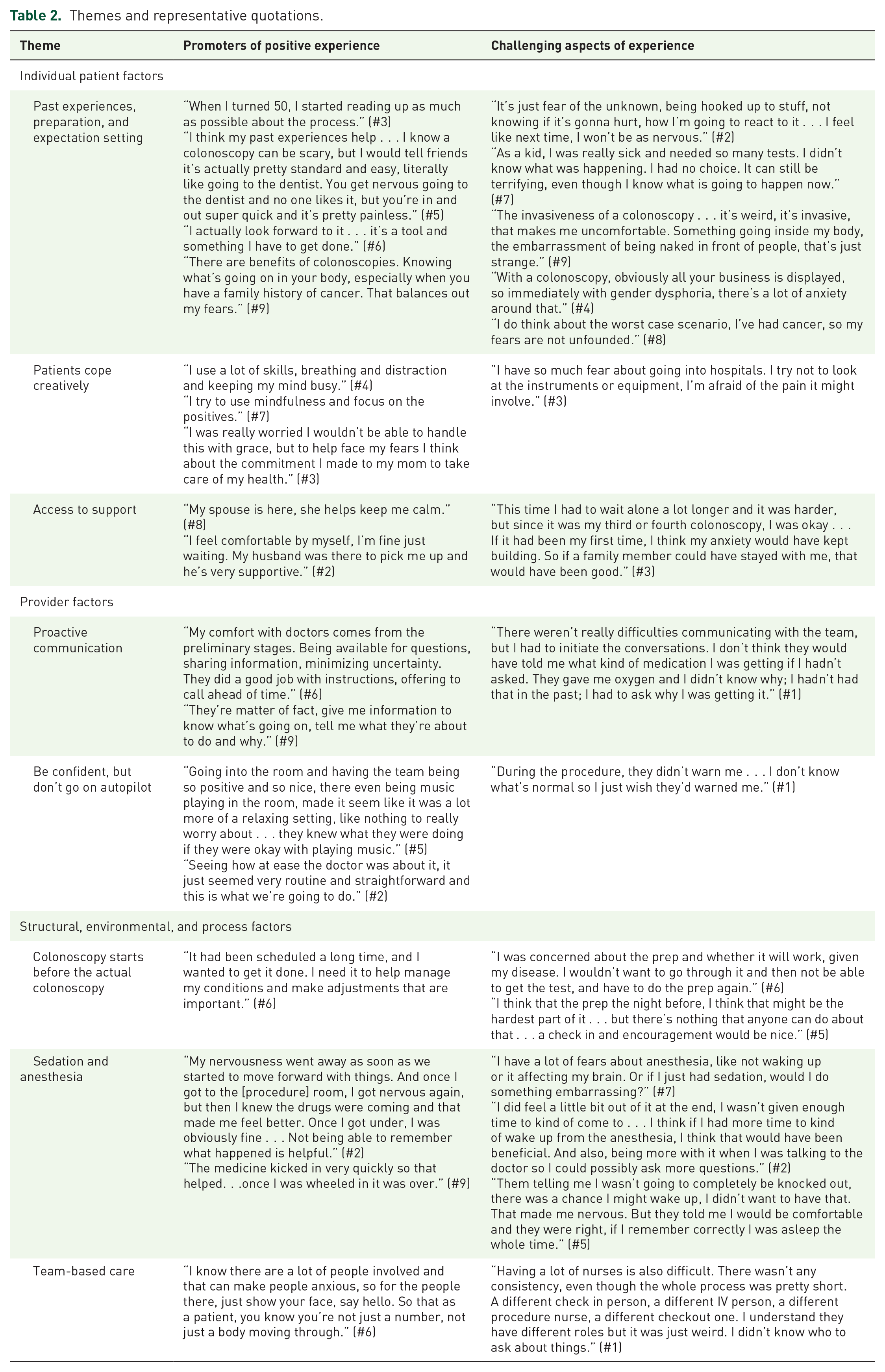
With respect to the Individual Patient Factors theme, patients identified personal factors, both related and unrelated to medical history, as key determinants of the colonoscopy experience. Three interacting subthemes comprised these individual factors, including “Past experiences, preparation, and expectation setting;” “Patients cope creatively;” and “Access to support.” Patients reflected on how uncertainty, invasiveness, and vulnerability in medical encounters increased colonoscopy-related anxiety. The impact of personal and family histories on healthcare varied—for example, for some, a family or personal history of cancer helped patients feel prepared for procedures; for others, childhood illnesses and cancer increased catastrophizing about potential bad outcomes. For all, the reassuring value of information provided by a colonoscopy mitigated distress and fear. The interaction of coping (“Patients cope creatively”) and support (“Access to support”) can explain the variable impact of these historical factors. That is, the influence of past events was attenuated depending on whether patients felt equipped to manage the stress of a colonoscopy and whether they had support that they felt met their needs. Some felt that their coping abilities meant that no additional support was necessary, whereas others identified the benefit of support from family members and hospital staff.
Patients also identified interacting Provider Factors that influenced their experiences. In particular, they discussed the importance of provider-initiated conversations (“Proactive communication”) and the value of individualized care within a routine procedure (“Be confident, but don’t go on autopilot”). Patients recognized the dissonant experiences between the patient and the provider on the day of a colonoscopy. For all, the fact that colonoscopies are routine for providers was reassuring and helped promote trust in the process. However, patients also shared that this could contribute to them feeling like a number or feeling worried about whether the process was proceeding normally. Patients expressed appreciation when providers explained not only the “what” but the “why” in reducing uncertainty and providing care that felt personalized.
Finally, Structural, Environmental, and Process factors also contributed to patient experiences. Importantly, patients viewed the colonoscopy process as beginning long before they came to the hospital (“Colonoscopy starts before the actual colonoscopy”). They identified the process as beginning at scheduling, whether the colonoscopy was part of regular healthcare maintenance or a helpful step in diagnosing the symptoms, and this is where anticipatory anxiety began. The preparation process, in particular, was a source of increased anxiety, with prominent feelings of being alone and worries about preparation quality interfering with getting the valuable health information they needed. Patients also discussed “Sedation and anesthesia” as central to the colonoscopy experience and a source of both comfort and anxiety. The importance of expectation setting and proactive communication applied to discussions around sedation as well, and patients cited anticipatory challenges and surprises related to understanding their sedation plans. In interviews, patients grappled with the fact that physical and emotional comfort could at times feel at odds; that is, the desire not to feel pain or remember the experience also involved an increased sense of vulnerability and giving up control, and could lead to challenges encoding important post-procedure communications from the medical team. Finally, patients recognized beneficial and challenging aspects of “Team-based care” as important parts of their colonoscopy experiences. Patients were cognizant of the complexities of the teams of staff and providers and felt that this could contribute to both communication challenges and the sense of being anonymous. At the same time, patients appreciated when it was apparent that members of the medical team worked in concert and communicated well with each other (“Be confident, but don’t go on autopilot”), explained their roles (“Proactive communication”), and made small gestures that recognized patients’ humanity and made them feel supported (“Access to support”).
Discussion
The results of this quality improvement study demonstrate that the interactions between a variety of patients, providers, and structural factors determine the psychological and emotional impact of a colonoscopy. All participants, regardless of their identities, past experiences, and mental health histories, identified the vulnerability and invasiveness inherent in the colonoscopy process, as well as the importance and utility of the procedure for managing their health. Certain factors appeared to serve as a buffer against this vulnerability, including perceived trust, transparency, and confidence; having had a prior illness detected early through screening; and use of coping strategies and a sense of feeling supported. Other factors, including having a minoritized identity, a history of past medical trauma, and uncertainty in both patient-provider communication and the colonoscopy process, rendered participants more likely to have a challenging emotional experience. At the time of the interview, within a week of colonoscopy, all patients continued to grapple with these positive and challenging aspects of the procedure and hold them in a dialectic. It is not clear from this study whether this balanced outlook on the experience remained, or whether patients’ perspectives shifted and solidified over time to a more extreme positive or negative position. Tracking longitudinal shifts over time was beyond the scope of this project, which prioritized recency as part of ecological validity, but is worthy of future investigation to improve a comprehensive understanding of patient perspectives. The sample size in this study precluded the possibility of conducting formal between-group analyses based on demographic factors and health histories. Other future directions include conducting deeper, targeted explorations of the impact of each of the factors identified in this study (e.g., qualitative or mixed-methods explorations focused on those with diagnosed PTSD or minoritized gender identities, or first-time vs repeat colonoscopy), as well as broader investigation of the generalizability of these factors (e.g., quantitative surveys in a different setting). These findings are overall consistent with previous research that establishes the varied reasons for procedure-related anxiety, including fears about the colonoscopy process and outcome, and the protective nature of education and patient-provider trust.
A number of factors that improve patient experience and reduce procedure-related distress have been identified previously, many of which are already considered standard of care or best practices. For example, studies indicate that patients highly value clear verbal and written communication, multimodal preparation instructions, and the prompt sharing of results,21,57,58 sentiments that were echoed by the participants in our study. In addition, adequate sedation is associated with higher patient satisfaction with the procedure.6,59 –63 The majority of colonoscopies are performed with either moderate or deep sedation (a small minority are performed without any sedation), though practices vary by setting. 59 Patient education and expectation setting about sedation are especially important, as many patients are unaware of the differences between these sedation types. In the case of moderate sedation, patients who are unprepared may be more distressed by awareness during the process if they were expecting to be completely unconscious, whereas those who are adequately prepared are less worried about this possibility. 64 In our study, although we did not specifically assess sedation type, feeling adequately sedated was associated with positive overall feelings about the procedure, though participants were also fearful of risks (losing control and death) and cited the after-effects of anesthesia as a barrier to communication and trust following the procedure. Finally, accompaniment by a trusted escort has been shown to reduce anxiety after the procedure, 65 and participants in our study discussed the importance of a supportive other to help with distraction and grounding prior to the procedure, and comprehension and communication after. Past research highlights how support from family and friends is associated with a positive procedure experience, both in terms of the practical (understanding preparation instructions, interpreting results) and emotional (mitigating fears, providing reassurance) aspects of the procedure. 21 Many of these aspects of high-quality care apply broadly to all hospital procedures, not only endoscopies.
Efforts to reduce anxiety and improve patient experience have targeted both patient and environmental factors. These include pre-endoscopy interventions directed at patient preparedness, including education8,66 –68 and cognitive and emotional processing, 69 that have been shown to reduce preprocedure anxiety. During the periprocedural time, low-cost interventions such as relaxing music, distraction, and virtual reality,70,71 as well as hospital clothing that protects a patient’s modesty beyond the standard open-back hospital gown, have also demonstrated benefits.72,73 Even without preprocedure interventions, in the periprocedural time, staff can reassure patients that their dignity will be protected and their bodies will remain covered until the procedure begins, and that the minimum amount of the buttocks will be exposed for scope insertion. They can also support patients’ intrinsic coping by asking simple questions such as “When you are feeling stressed or overwhelmed, what do you do that helps?” and encouraging engagement from patients’ friends or family if relevant. More recently, experts have issued recommendations for providing TIC in gastroenterology, focused on education of all levels of staff regarding the ubiquity of trauma and diversity of trauma responses, implementing trauma screening in the clinic, emphasizing patient autonomy and transparent communication, and creating a safe physical environment.74 –76 With respect to GI procedures, suggestions for providing TIC during anorectal examinations include obtaining consent before and during procedures, ongoing monitoring for distress, and debriefing after the procedure. 77
Prior research has shown that certain cognitive and emotional styles commonly associated with baseline anxiety and posttraumatic stress, including emotional avoidance and pain catastrophization, predict in-procedure pain and emotional distress.7,78,79 Thus, it is possible that preprocedure interventions designed to address these mental health concerns and processes could improve patients’ experiences. In patients who are known to a gastroenterology clinic, it is likely that a preprocedure referral to an embedded GI psychologist could help not only with the development of adaptive coping strategies but also with increased knowledge about the procedure and associated process. In settings without mental health providers, any opportunity for preprocedure contact with a provider, for example, a member of the nursing staff or a patient navigator, is likely to improve adherence and outcomes. 80 If patients with known trauma can receive services before their procedure, the likelihood of a failed procedure (e.g., incomplete preparation and incomplete procedure due to trauma or pain) may decrease, providing a corrective experience for the patient and bolstering their mental health recovery, and reducing the chance of burnout among staff and providers by reducing the number of stressful clinical encounters and empowering resilient coping when they do occur.81,82
Yet the findings in the present study suggest that such targeted interventions may be helpful but insufficient. First, all participants, regardless of prior experience and formal mental health history, expressed worry and concern of varying degrees of severity. Second, as previously discussed, many people are hesitant to reveal trauma and other sensitive mental health information to providers due to fears of stigma and concern about retraumatization. This may be especially relevant in the endoscopy context, as many procedures are performed “open access,” 83 meaning that limited health information may be available and there are limited opportunities to develop patient-provider trust in advance. This highlights the importance of a universal, trauma-informed approach to care for all patients, not only those with previously identified mental health concerns. Although there are challenges to implementing TIC, including cost, time, and buy-in, interest among GI staff, providers, and patients is clear, 76 and evidence suggests that collaborative approaches that involve patient and staff stakeholders facilitate implementation and have benefits for both patients’ and staff’s well-being. 84 Recommendations informed by our fieldwork and patient interviews, as well as potential barriers and challenges to implementing these changes, are in Table 3.
Recommendations for patient-centered, trauma-informed endoscopy care.

Our findings and these recommendations should be considered in light of the study’s limitations. We recognize that in qualitative studies, the data generated is “co-created” and susceptible to bias and influence by the interview questions. This could mean that certain perspectives are overemphasized. For example, it is possible that patients might have overemphasized both positive and negative aspects of the experience because of our direct inquiry, or that our questions might have heightened distress. We sought to mitigate bias by designing the study as an interdisciplinary team, seeking patient perspectives throughout the development process, and engaging reflexively throughout our analysis.
Although we used purposive sampling to recruit a diverse sample in terms of demographics (age and gender), indication for colonoscopy, and number of past colonoscopies, our sample was also small, English-speaking only, and from a single rural academic medical center. The perspectives and recommendations here may be mere snapshots and may not be generalizable to other populations and settings. In addition, we could not consider colonoscopy outcomes in our sampling, given that participants were recruited before their procedures. By chance, at the time of the follow-up interview, none of the participants had a bad outcome (e.g., active disease progression necessitating surgery and detection of cancer). Perspectives from these patients could be particularly important, as these outcomes may be more likely to result in medical posttraumatic stress. The one participant in our study who was transgender experienced an adverse event involving misgendering by staff following their procedure, an unfortunately common healthcare experience for transgender people. 85 This participant’s experience highlights the importance of acknowledging not only the vulnerability inherent in these procedures but also the additional distress faced by people from minority backgrounds due to misgendering, power imbalances, and/or systemic inequities, for example. Given that transgender people are at higher risk of worse gastrointestinal health outcomes overall due to minority stress and barriers to accessing quality preventive care,86,87 more research should be conducted to better understand the endoscopy experiences of this group and to establish best practices for gender-affirming endoscopy care.88,89 In addition, absent from this research are the perspectives of individuals who, because of anticipatory fears or negative past experiences, may avoid colonoscopies entirely.10 –14 Future research should investigate further the potential role of mental health concerns, including prior trauma, in procedure no-shows and cancellations. Given that TIC efforts may be particularly beneficial for these patient populations, future work should consider targeted recruitment strategies.
Conclusion
Recent efforts to define and implement TIC in GI settings are promising, as our research and others identify that patient support needs are not being met 58 and providers and staff are already overburdened. 81 The present study highlights that colonoscopies have the potential to be both stressful and reassuring, and the psychological impact of a procedure depends on patient, provider, and environmental factors, highlighting the importance of a system-wide trauma-informed approach. Future directions include monitoring patient perspectives over time; in-depth exploration with specific subpopulations; larger, quantitative studies to evaluate the relative contributions and interactions of the patient, provider, and process factors; and measuring the impact of TIC changes on patient and staff experience as well as procedure quality metrics. With TIC increasingly considered the standard of care, future efforts should focus on innovation in trauma-informed endoscopy to improve both patient and provider experience and ensure that all patients who need these procedures have an equal opportunity to have them completed.
Supplemental Material
sj-docx-1-tag-10.1177_17562848251346250 – Supplemental material for “It’s a tool, it’s got hardships”: a qualitative study of patient experience of colonoscopy and implications for trauma-informed care
Supplemental material, sj-docx-1-tag-10.1177_17562848251346250 for “It’s a tool, it’s got hardships”: a qualitative study of patient experience of colonoscopy and implications for trauma-informed care by Katrina S. Hacker, Michael A. Curley, Corey A. Siegel and Jessica K. Salwen-Deremer in Therapeutic Advances in Gastroenterology
Footnotes
Acknowledgements
The authors thank the patients and staff at the Dartmouth Hitchcock Medical Center endoscopy unit and the GI motility team for their input and support in conducting this project.
Declarations
Supplemental material
Supplemental material for this article is available online.
References
Supplementary Material
Please find the following supplemental material available below.
For Open Access articles published under a Creative Commons License, all supplemental material carries the same license as the article it is associated with.
For non-Open Access articles published, all supplemental material carries a non-exclusive license, and permission requests for re-use of supplemental material or any part of supplemental material shall be sent directly to the copyright owner as specified in the copyright notice associated with the article.