
Abstract
Background:
Music has been shown to reduce pain and anxiety in patients undergoing colonoscopy. Distraction, a newer technique with less available evidence, has shown similar effective outcomes.
Objectives:
This systematic review and meta-analysis evaluate the current evidence available on music and task distraction and its potential to reduce pain in colonoscopy.
Design:
The study was performed within PRISMA guidelines and registered with PROSPERO. Inclusion criteria comprised peer-reviewed randomised controlled trial publications in English. Exclusion criteria comprised duplicate studies, non-peer-reviewed and non-English studies.
Methods:
A literature search was conducted with Medline, Embase, Cochrane and Google. Two independent clinicians reviewed the studies to avoid inclusion bias. Visual analogue score mean pain and Spielberger State-Trait Anxiety Inventory (STAI) mean anxiety were collected. Inverse variance DerSimonian-led meta-analytical approach was conducted using a random effects model and statistical software STATA.
Results:
Music intervention reported a significant (p < 0.05) weighted mean reduction of 1.50 for pain scores (95% CI 0.69–2.31) and a significant weighted mean reduction of 3.56 for anxiety scores (95% CI 0.86–6.27).
Distraction intervention reported a significant weighted mean reduction of 1.59 for pain scores (95% CI 0.79–2.39) and a significant weighted mean reduction of 7.49 for anxiety scores (95% CI 3.64–11.35). There was high heterogeneity recorded for both pain and anxiety studies (I² >90%).
Conclusion:
Music and distraction intervention has the ability to be introduced at minimal cost. Furthermore, no changes to endoscopy infrastructure are required. This allows a clinical real-world option that is immediately implementable for patients. This meta-analysis has demonstrated that there is a potential role for music and task distraction to reduce pain and anxiety for patients undergoing a colonoscopy. It supports a low cost and safe option for patients who may not be eligible for sedation. Whilst the body of evidence is growing, it is plausible to claim these interventions can be implemented and established into daily clinical practice.
Plain language summary
Music and distraction have been shown to reduce pain and anxiety for patients undertaking a colonoscopy.
This review and analysis evaluates the current evidence available in literature.
Studies were evaluated using established criteria and the two factors looked at where pain scores and anxiety scores reported by patients. Scores were compared between no intervention and either the music or distraction technique.
The results were that both music and distraction reduced both pain and anxiety scores for patients. The results were also of statistical significance adding further weighting that this is a direct impact of these interventions.
There is a possibility to introduce these interventions at minimal cost with no major changes needed to an endoscopy department and therefore could be implemented in a short time frame also.
In summary this review and analysis has highlighted that there is a role for music and task distraction to reduce pain and anxiety for patients undertaking a colonoscopy. It suggests a safe and low-expense option for patients who may not be able to have sedation.
Introduction
The diagnostic and therapeutic role of colonoscopy in the investigation of bowel symptoms has been widely documented. It is the gold standard procedure for detecting colorectal cancer.1,2 A significant barrier to patients attending for colonoscopy is the anticipated pain and discomfort they may experience, which can be up to 84%. 3 This can occur for both first-time and reattending patients. 4 Anxiety has also been demonstrated to be an important predictor of patient co-operation during a colonoscopy procedure. 5 Pain and anxiety can therefore result in reduced engagement with clinical services, which can have a detrimental effect on precancerous and cancer detection rates. 6
A frequently utilised method to reduce the level of anticipated discomfort and anxiety is to use medication administered prior to the commencement of a colonoscopy procedure. Pain relief and sedation administered include Fentanyl and Midazolam. This may not be a viable option in specific scenarios, such as attendance without an escort, common for patients who live alone. A medical history of renal or liver failure, advanced age, drowsiness and alcohol abuse are other possible contraindications. 7 The required post-procedure care for patients who are administered sedation can require prolonged observation, resuscitation support such as intravenous fluids and in some cases reversal of the medication administered. Entonox (Nitrous oxide and air) is an alternative option to reduce pain and anxiety, but also has contraindications to its use, such as chronic lung conditions, recent ear and eye procedures and recent head injury. 8 Therefore, there is a possibility of a significant proportion of patients who are susceptible to a higher likelihood of pain and discomfort during colonoscopy due to no viable option to improve their pain and anxiety. It highlights a need to improve or modify current methods to mitigate anticipated pain, discomfort and anxiety peri-procedure in the most effective manner possible.
The advantages of music in medical settings have been previously documented, such as in surgical operating theatres.4,9–11 A wide array of musical genres has been implemented in past studies with the most evidence for classical music reported. 12 This is due to a slow tempo of 60–80 beats per minute of sound and no significant rhythm, allowing relaxation, sedation and a decreased heart rate.4,13,14
Task distraction techniques as an alternative to music have been implemented historically, but have a less developed evidence base. Methods are relatively inexpensive and non-invasive, such as smartphone distraction, with a high likelihood of patients possessing a compatible device, allowing easy accessibility. 15 The benefits have been demonstrated in burn units where virtual reality (VR) has been used for pain management. 16 Distraction provides a positive focus and attention on a more pleasant sensation compared to what may be being experienced. 15
Task distraction can consist of video observation, VR observation and manual tasks. Multiple modalities can also be used consecutively, such as audio with video playback.17–19
VR and multimodal distraction engage specific mechanistic and neurophysiological pathways. These include attention modulation, in which attention can be redirected away from painful stimuli, thereby reducing pain perception. Pain processing pathways are activated and can reduce the emotional experience of pain and neurochemical pathways can increase serotonin and endogenous opioid neurotransmitters, contributing to analgesia. 20
Previous meta-analyses have been undertaken looking at the effect of music on colonoscopy (Table 1). However, these reviews have lacked scope, limited analysis and inclusion criteria, which this systematic review and meta-analysis aims to address. This systematic review and meta-analysis will aim to identify the effect of music and distraction on pain and anxiety for patients undergoing a colonoscopy.
Summary of music and distraction meta-analyses previously undertaken.

RCT, randomised controlled trials.
Two systematic reviews have been undertaken for distraction, focusing on visual distraction (Table 1). This is the first systematic review and meta-analysis to date reporting on multiple distraction techniques, including smartphone and VR. In addition, subgroup analysis undertaken on distraction reports upon how blinding, previous colonoscopy, sedation, intra-procedural therapy and type of distraction technique impacts pain and anxiety scores.
Methods
This review was conducted and reported in accordance with the Preferred Reporting Items for Systematic Reviews and Meta-Analyses (PRISMA) statement 27 (Supplemental Appendix 1). The study protocol was pre-registered with PROSPERO (Registration No: CRD42025639821).
Search strategy
A comprehensive literature search was conducted using Medline, Embase, Cochrane Library and Google Scholar databases up to December 2024 (Figure 1). Following this, a manual search was conducted for any additional relevant articles published alongside a review of previous meta-analyses to identify additional relevant published articles.

Preferred Reporting Items for Systematic Reviews and Meta-Analyses (PRISMA) flow diagram of study selection.
The full search terms used are described in Supplemental Appendix 1 and include MeSH terms ‘music’; ‘smartphone’; ‘distraction’; ‘virtual reality’ and ‘colonoscopy’.
For studies with full text not available for review, authors were contacted, with no response from two studies, and hence excluded.28,29 Major gastrointestinal meeting abstracts were not searched as part of the literature review and the meta-analysis search was limited to randomised controlled trials (RCT).
Primary and secondary outcomes
The primary outcomes were mean pain and anxiety scores reported by patients undertaking colonoscopy with and without intervention. The mean score was calculated using a graded score scale completed by the patients. The pain score used was the visual analogue score (VAS) developed by Price et al. 30 and anxiety score used was the Spielberger State-Trait Anxiety Inventory (STAI) developed by Charles Spielberger (1983). 31
Inclusion/exclusion criteria
Inclusion criteria were as follows: (1) Patients aged 18 years and older; (2) RCT study; (3) published in English; (4) relevant to the outcomes and (5) a colonoscopy procedure.
Exclusion criteria were as follows: (1) Duplicate publications or no original data present; (2) no full text available; (3) studies not in English; (4) Studies not relevant to the question and (5) a gastroscopy or sigmoidoscopy procedure only.
Study selection
Two authors (J.A. and N.P.) reviewed the studies with abstracts independently screened for relevance to the questions and outcomes. Duplicate studies and those meeting exclusion criteria were excluded. Full-text review then followed. For any data not identified within the manuscript, the corresponding authors were contacted for additional information or clarification.
Data extraction
Spreadsheet software was used to collect data from each study. Data extracted consisted of the following: (1) study details of authors, year of publication and journal; (2) study design and if an RCT; (3) mean pain score or mean anxiety score (scale used, range, standard deviation or interquartile range provided).
Three of the music studies and four of the distraction studies required the use of simple mathematical calculations for data extraction. This was to allow statistical comparison to be performed more efficiently. Data was also gathered on how music or distraction was delivered, timing and duration of interventions, previous procedures and the use of sedation, therapy, randomisation and blinding.
Statistical analysis
An inverse variance DerSimonian-led meta-analytical approach was conducted. Both weighted mean difference and proportional change were calculated. Summary scores and confidence intervals (CIs) were calculated. Significance was set at a p-value of <0.05. Meta-analysis of data was conducted using a random effects model. Where available, missing data were imputed, such as standard deviation, during statistical analysis.
Inter-study heterogeneity was assessed using the I2 value to measure the degree of variation not attributable to chance alone. A value of 0–29 was considered low heterogeneity, 30–59 was considered medium heterogeneity, and anything 60 or above was considered high heterogeneity. A sensitivity analysis was also undertaken.
The study was performed in line with Cochrane recommendations and PRISMA guidelines and using the statistical software StataCorp LLC (version 15).
Study quality assessment
Study quality was independently assessed using the Jadad scale for RCTs. Studies with a Jadad scale score of 3 or more were considered good studies. All studies were included in the statistical analysis and discussion (Supplemental Appendix 2a/2b). Publication bias analysis was also undertaken.
Results
Eligible studies
Music: A total of 29 music studies were identified from database searches (Figure 1). Classical music was the most popular genre, followed by the traditional music of the originating study country. After removal of duplicates, 19 studies for music were screened and identified for full-text review. After further evaluation and application of the exclusion criteria, 11 studies were eligible for inclusion in this meta-analysis (Table 2).15,16,33–40
Summary of study characteristics from music RCTs.

RCT, randomised controlled trials.
Task distraction: A total of 82 distraction studies were identified from database searches (Figure 1). After removal of duplicates, 47 studies for distraction were screened and identified for full-text review. After further evaluation and application of the exclusion criteria, 16 studies were eligible for inclusion in this meta-analysis (Table 3).15,17–20,41–47
Summary of study characteristics from distraction RCTs.
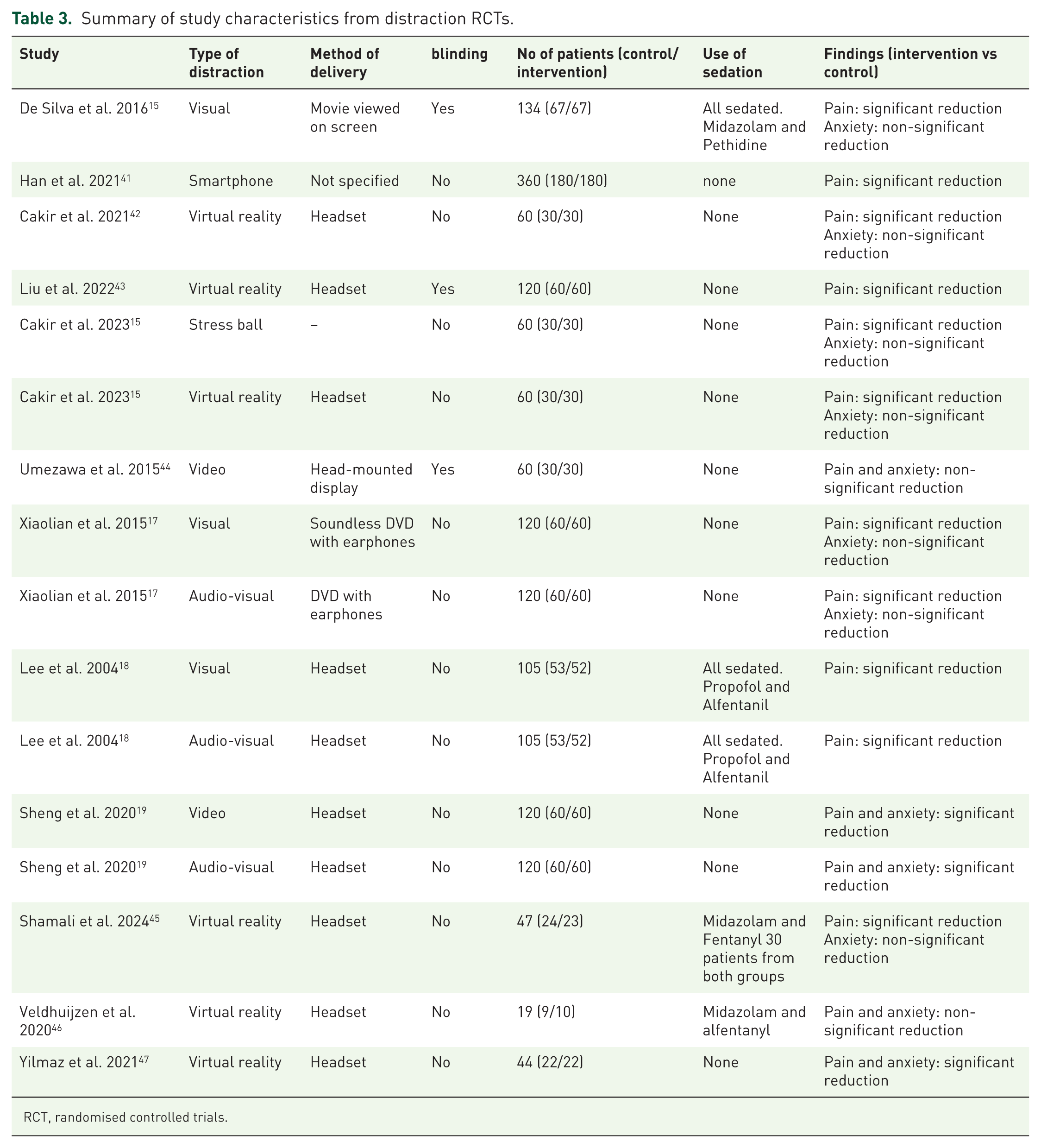
RCT, randomised controlled trials.
Music
A cumulative total of 1590 patients were recruited over 11 music RCT studies. Six studies analysed both pain and anxiety scores, four studies reported on pain scores only and one study on anxiety scores only. Seven studies scored at least three on the Jadad scale for reporting RCTs. 48 In 4 of the 11 studies, the endoscopist was blinded. Out of these four studies, two reported that pain scores significantly reduced with intervention. No blinded study showed anxiety scores significantly reduced with intervention. Table 2 summarises the RCT studies with music intervention.
Pain
Six of the 10 music RCT studies (775 patients) found the intervention group with music to have a significant improvement in pain scores. Four studies reported an improvement but no significant difference.
Overall, there was a significant (p < 0.0005) weighted mean reduction of 1.50 for pain scores with music intervention, with a 95% CI (0.69–2.31; Figure 2).
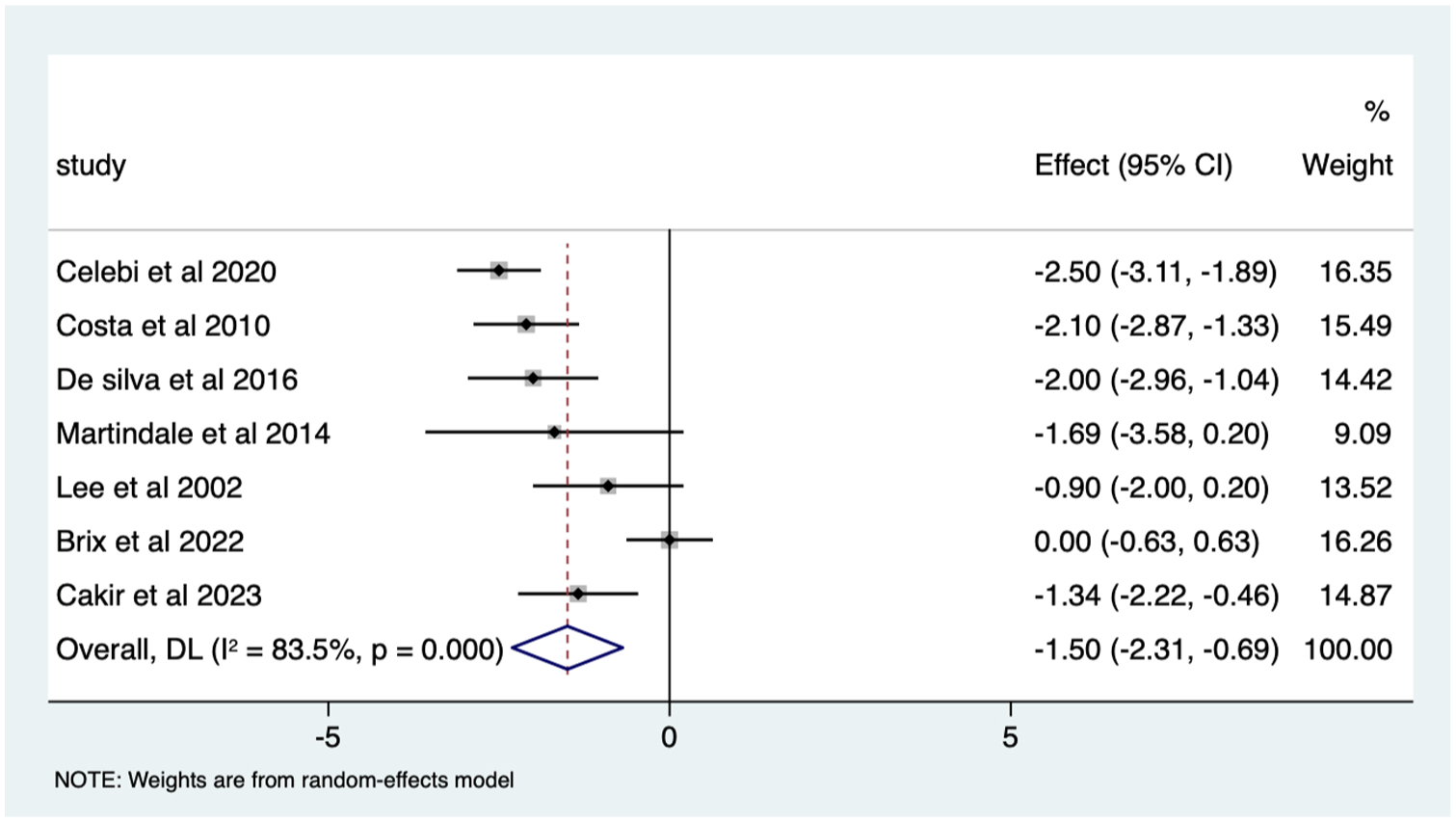
Music RCT pain score Forrest plot.
Overall, there was a significant pain score change of 37% in VAS (p < 0.0005) with a 95% CI (0.17–0.57; Supplemental Appendix 3).
The heterogeneity is high with an I2 value of 97.8%. The average quality score was 3, representing a good score.
Anxiety
Three of the seven studies (334 patients) found the intervention group with music to have a significant improvement in anxiety scores. Four studies found an improvement but no significant difference.
Overall, there was a significant (p < 0.05) weighted mean reduction of 3.56 for anxiety scores with music intervention, with a 95% CI (0.86–6.27; Figure 3).
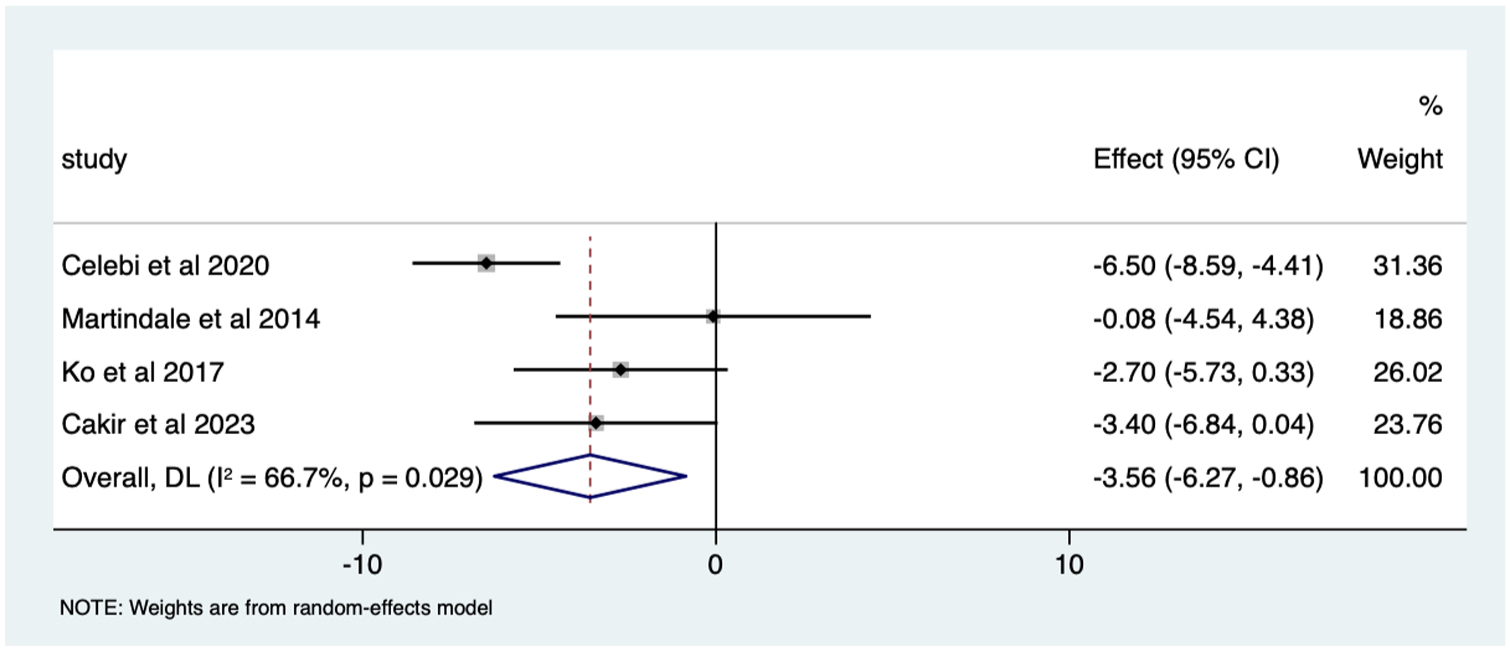
Music RCT anxiety score Forrest plot.
Overall, there was a significant anxiety score change of 46% in VAS (p < 0.0005) with a 95% CI (0.12–0.80; Supplemental Appendix 4). The heterogeneity was high with an I2 value of 99.2%. The average quality score was 3 representing a good score.
The choice of music varied, with the majority of studies aiming to implement music with an underlying relaxing tone. Six (54.5%) studies had patients listening via head/earphones. Three of these six studies showed significant pain reduction with headphones. One out of four studies had a significant anxiety score reduction with headphones. 32
Four (30.8%) studies used a speaker. Two out of three33,34 reported a significant pain difference and two out of three33,35 reported a significant anxiety score difference.
One (7.7%) study used a mounted headset, with significant pain reduction reported. 16
The onset of music being played was most often during the colonoscopy procedure, with three studies not explicitly describing the start, stop and duration of the music34,36,37 and three studies describing starting the music before the procedure.15,33,38 Two out of three had a statistically significant decrease in pain and one out of three a statistically significant decrease in anxiety in those studies starting music beforehand.33,38
Nine of the 11 music RCT studies used sedation alongside the music intervention, with some studies not detailing the specifics of name, dose, exact quantities used and if administered on patient demand. In the studies that reported sedation; midazolam and pethidine was used. Six studies reported a significant pain reduction and four no significant pain reduction. Five studies measured anxiety and sedation use, with only one study reporting a significant reduction. Two studies measured anxiety with no sedation use, with one study reporting a significant anxiety reduction.
Task distraction
A cumulative total of 1163 patients were recruited over 12 distraction studies. Nine studies analysed both pain and anxiety scores and three studies reported on pain scores only. Twelve RCT studies assessed pain with 16 distraction techniques used as intervention arms. Nine RCT studies assessed anxiety with 12 distraction techniques used as intervention arms. All 12 studies scored at least 3 on the Jadad scale for reporting RCTs. 48 In 3 of the 12 studies the endoscopist was blinded and of these three blinded studies, two demonstrated a significant reduction in pain score. No blinded study reported that anxiety scores were significantly reduced. Table 3 summarises the RCTs with distraction intervention.
Pain
Fourteen of the 16 techniques found the distraction intervention group to have a significant improvement in pain scale reporting. The remaining two techniques found non-significant improvement.
Overall, there was a significant (p < 0.0005) weighted mean reduction of 1.59 for pain scores with distraction intervention, with a 95% CI (0.79–2.39; Figure 4).
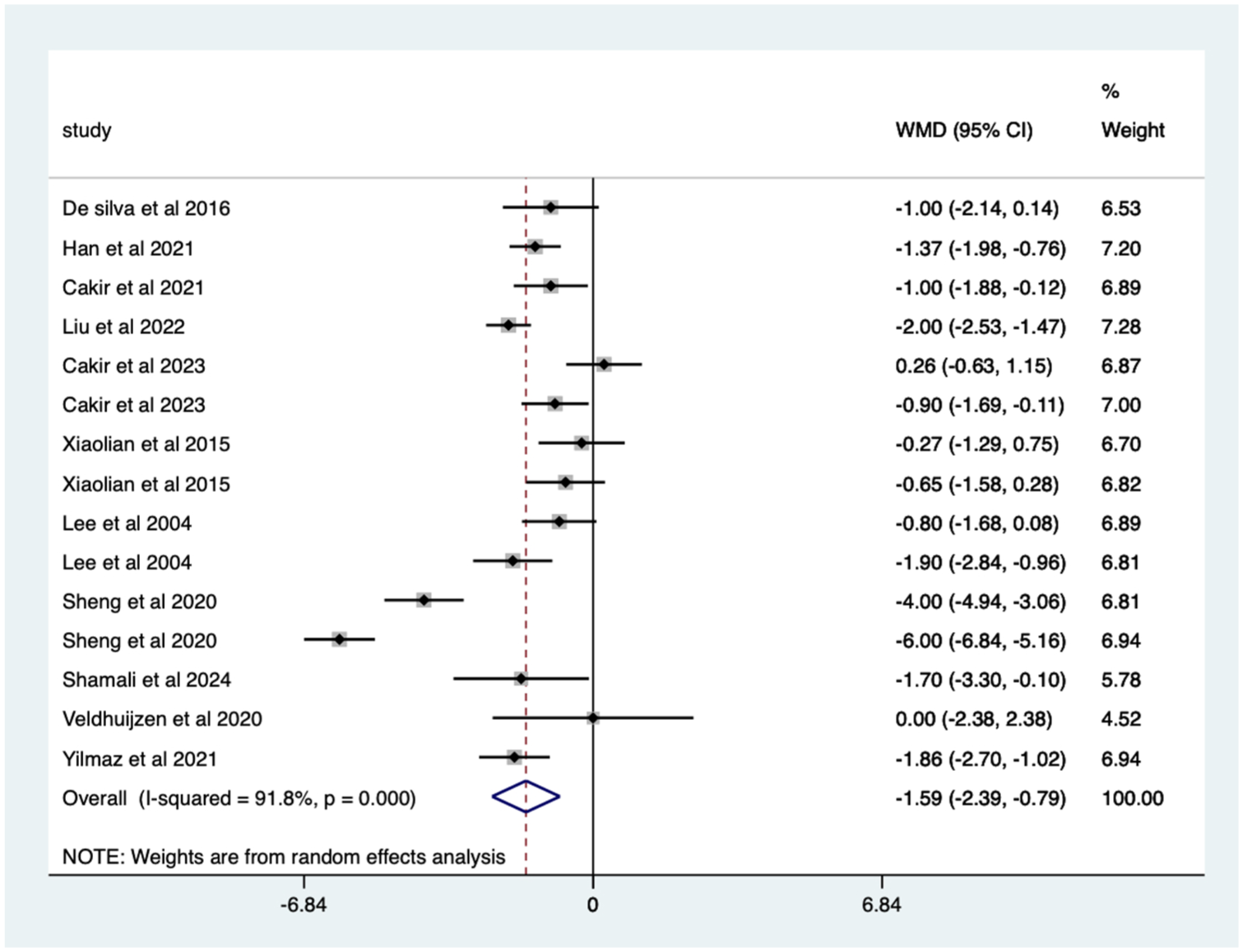
Distraction RCT pain score Forrest plot.
The heterogeneity was high with an I2 value of 91.8%. The average quality score was 3, representing a good score.
Anxiety
Three of the nine techniques found the intervention group with distraction to have a significant improvement on the anxiety scale scoring. Six techniques found no significant difference.
Overall, there was a significant (p < 0.0005) weighted mean reduction of 7.49 for anxiety scores with distraction intervention, with a 95% CI (3.64–11.35; Figure 5).
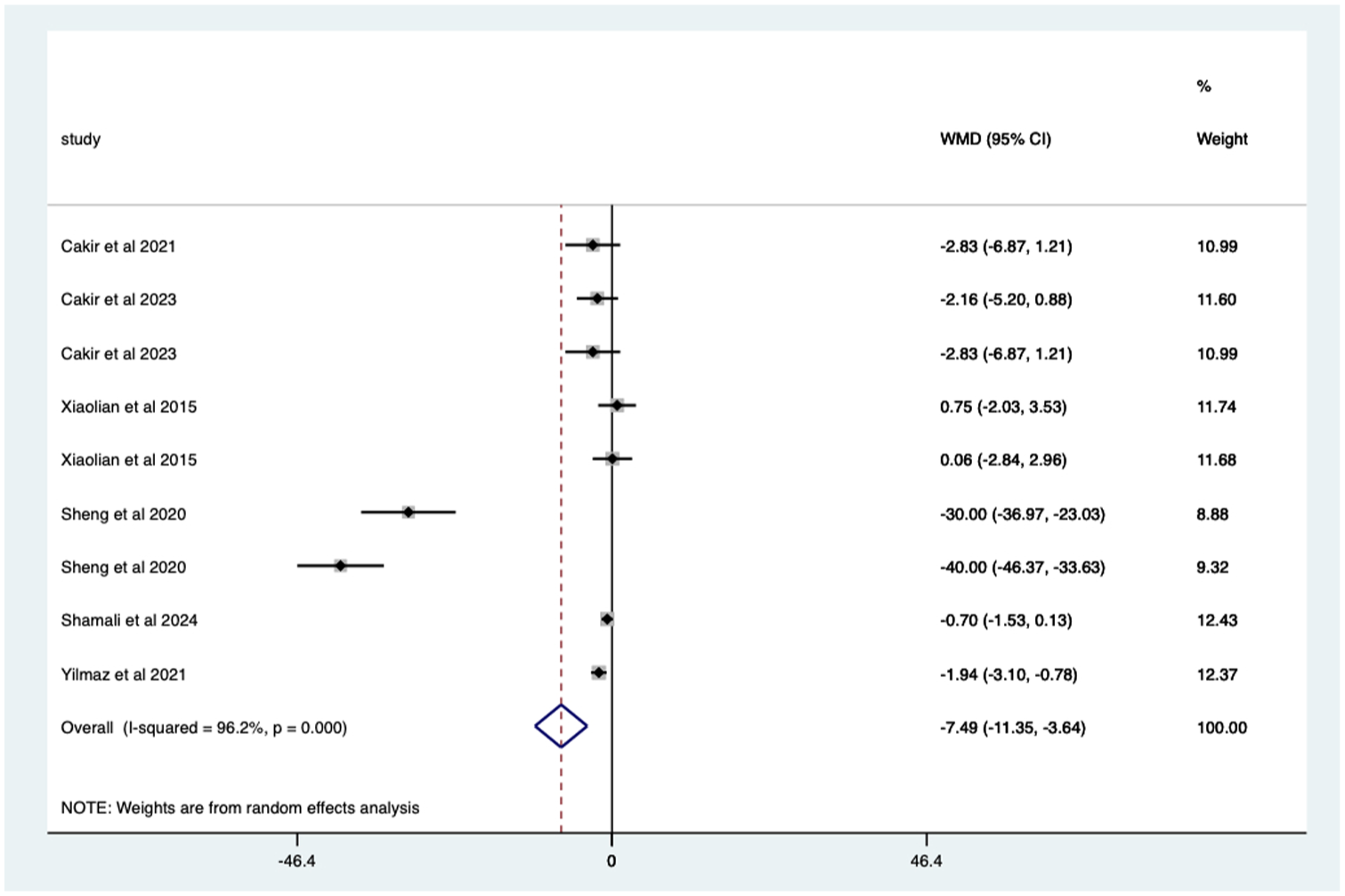
Distraction RCT anxiety score Forrest plot.
The heterogeneity is high with an I2 value of 96.2%. The average quality score was 3, representing a good score.
The distraction methods used included five visual/video, four combined audio and video, six VR, one smartphone and one stress ball.
Four out of five visual technique studies found distraction intervention to reduce pain scores significantly. One out of three visual technique studies found that distraction intervention reduced anxiety scores significantly.
All four audio-visual technique studies reported a statistically significant decrease in pain with intervention. One out of three audio-visual technique studies reported a statistically significant decrease in anxiety.
Five out of six VR technique studies reported a significant pain score reduction with intervention, and one VR technique study reported a significant anxiety score reduction.
The smartphone technique study reported a significant reduction in pain with intervention and the stress ball technique study reported a significant pain score reduction and no significant anxiety score reduction.
Four of the 12 studies used sedation alongside the distraction intervention. Three studies reported a significant pain reduction for the five distraction techniques used.
One study used propofol and alfentanyl, whilst three used midazolam and pethidine.
The three studies measuring anxiety and using sedation all reported a non-significant anxiety score reduction.
Distraction sub-analysis
The 12 distraction studies were analysed in further detail, looking at multiple components which may influence the effect of the intervention. These included:
Blinding
Patients who have undertaken a previous colonoscopy
Sedation
Undergoing therapeutic intervention
Distraction type
(All references to significance in the results below refer to a p-value of <0.01.)
Blinding
Pain
Studies with blinding – significant mean 1.55 (CI 0.57–2.52) pain score reduction (Figure 6).

Studies with blinding; pain score Forrest plot.
Studies with no blinding – significant mean 1.39 (CI 0.38–2.40) pain score reduction (Figure 7).

Studies with no blinding; pain score Forrest plot.
Anxiety
Studies with no blinding – significant mean 7.49 (CI 3.64–11.35) anxiety score reduction (Figure 8).

Studies with no blinding; anxiety score Forrest plot.
Studies with blinding – One distraction study underwent blinding but had incomplete information with no standard deviation data.
Previous colonoscopy
Pain
Studies with previous colonoscopy – significant mean 1.80 (CI 0.71–2.89) pain score reduction (Figure 9).

Studies with patients undergoing previous endoscopy; pain score Forrest plot.
Studies with no previous colonoscopy – significant mean 1.04 (CI 0.15–1.94) pain score reduction (Figure 10).

Studies with patients undergoing no previous endoscopy; pain score Forrest plot.
Anxiety
Studies with previous colonoscopy – significant mean 10.15 (CI 5.33–14.97) anxiety score reduction (Figure 11).

Studies with patients undergoing previous endoscopy; anxiety score Forrest plot.
Studies with no previous colonoscopy – non-significant mean 0.42 (CI −2.43 to 1.59) anxiety score reduction (Figure 12).

Studies with patients undergoing no previous endoscopy; anxiety score Forrest plot.
Sedation
Pain
Studies with sedation – significant mean 1.23 (CI 0.68–1.78) pain score reduction (Figure 13).

Studies with patients undergoing sedation; pain score Forrest plot.
Studies with no sedation – significant mean 1.87 (CI 0.7–3.03) pain score reduction (Figure 14).

Studies with patients undergoing no sedation; pain score Forrest plot.
Anxiety
Studies with sedation – non-significant mean 0.65 (CI −0.15 to 1.45) anxiety score reduction (Figure 15). Studies with no sedation – significant mean 9.10 (CI 3.36–14.84) anxiety score reduction (Figure 16).

Studies with patients undergoing sedation; anxiety score Forrest plot.

Studies with patients undergoing no sedation; anxiety score Forrest plot.
Previous endotherapy
Pain
Studies with no endotherapy – significant mean 1.65 (CI 1.05–2.24) pain score reduction (Figure 17).

Studies with patients undergoing no endotherapy; pain score Forrest plot.
Studies with endotherapy – significant mean 1.70 (CI 0.43–2.97) pain score reduction (Figure 18).

Studies with patients undergoing endotherapy; pain score Forrest plot.
Anxiety
Studies with endotherapy – significant mean 10.54 (CI 2.36–18.71) anxiety score reduction. Studies with no endotherapy – non-significant mean 1.48 (CI −0.13 to 3.10) anxiety score reduction (Figure 19).
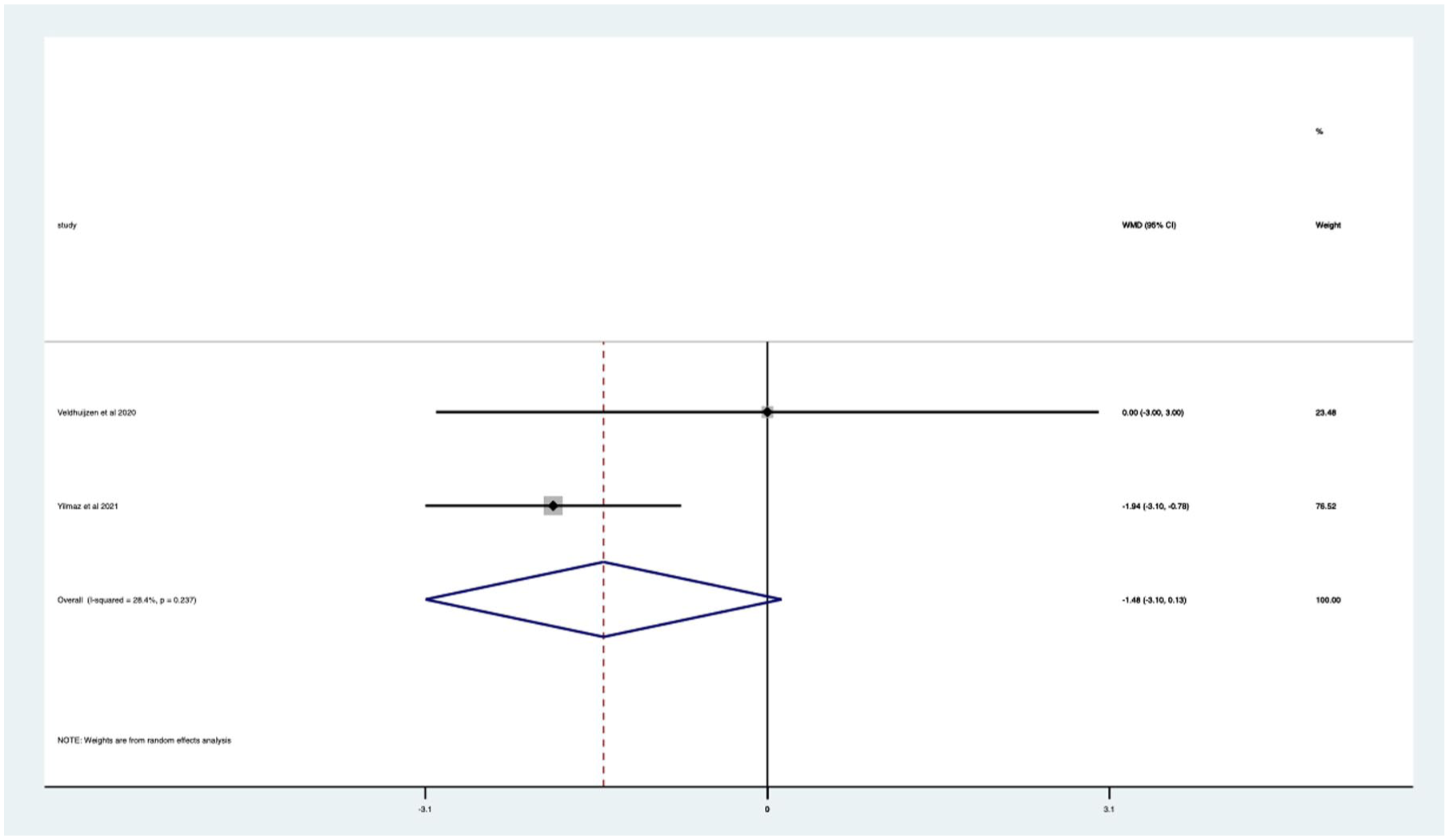
Studies with patients undergoing no endotherapy; anxiety score Forrest plot.
Studies with endotherapy – significant mean 10.54 (CI 2.36–18.71) anxiety score reduction (Figure 20).

Studies with patients undergoing endotherapy; anxiety score Forrest plot.
Distraction type
Pain
VR studies – significant mean 1.24 (CI 0.75–1.73) pain score reduction (Figure 21).

Studies with VR distraction; pain score Forrest plot.
Audio-visual studies – significant mean 2.28 (CI 0.39–4.16) pain score reduction (Figure 22).

Studies with audio-visual distraction; pain score Forrest plot.
(Smartphone distraction studies did not have enough data to perform sub-analysis.)
Anxiety
VR studies – significant mean 1.39 (CI 0.44–2.33) anxiety score reduction (Figure 23.

Studies with VR distraction; anxiety score Forrest plot.
Audio-visual studies – significant mean 17 (CI 0.74–33.26) anxiety score reduction (Figure 24).

Studies with audio-visual distraction; anxiety score Forrest plot.
(Smartphone distraction studies did not have enough data to perform sub-analysis.)
Publication bias assessment
Egger’s regression test was performed on the study data with a non-significant result, suggesting no publication bias (p = 0.641). Figure 25 displays the funnel plot with full statistical analysis in Supplemental Appendix 5.
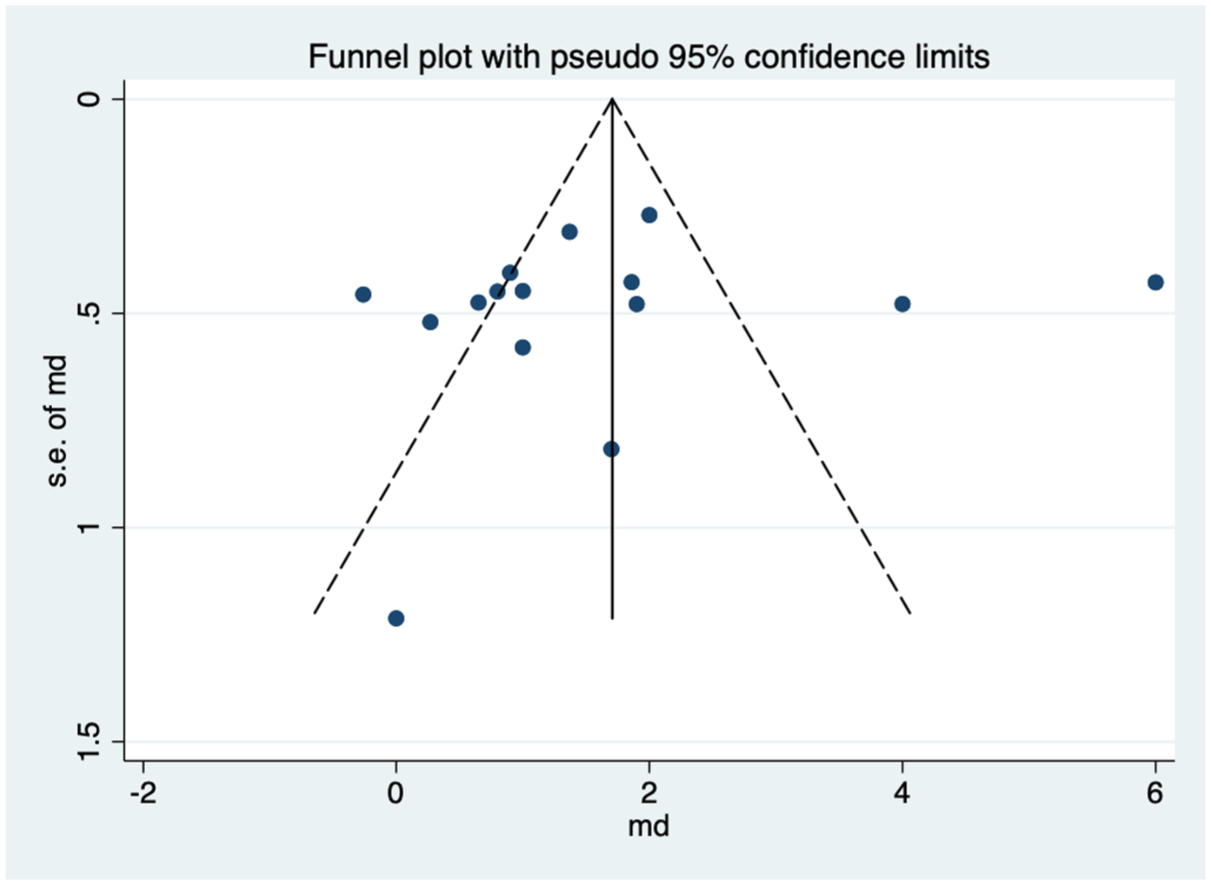
Publication bias funnel plot.
Discussion
This systematic review and meta-analysis consisted of 27 RCT studies with 2753 patients. Overall outcomes for both pain and anxiety demonstrated a significant reduction in both scores using music and distraction techniques.
This paper has demonstrated the possible benefits of non-invasive, inexpensive interventions in the reduction of pain and anxiety scores. It has reinforced the evidence known on the more established technique of music and introduced task distraction as a comparable and similarly impactful means to improve pain and anxiety scores for patients.
The mean pain score reduction with music supports the findings of two previous meta-analyses.4,23 The mean anxiety score reduction with music also concurs with findings from Wang et al. 4 The mean pain score reduction with distraction supports the findings of two recent meta-analyses.25,26 The mean anxiety score reduction with distraction is also in agreement with findings from Saab et al. 26
A 1.5 and 1.59 pain score reduction represents a comparable 15%–16% decrease in pain reported by patients with the aid of intervention. This has the possibility of a significant clinical impact when studies have reported with sedation, a comparable decrease in pain of 10%. 49 The clinical impact of the reduction in anxiety with these interventions has also been demonstrated, in particular with task distraction (7.49), where a score reduction between 5 and 10 is often considered meaningful. 50
Alongside the two main primary outcomes analysed, other outcomes were identified to show the benefit from the intervention. Patients reported greater satisfaction, more willingness to undergo a repeat colonoscopy procedure, shorter duration of procedure, shorter caecal intubation time and lower average sedation use.15–18,20,32–40,41–47
Both interventions provide a low-cost and easy-to-implement option with potential scope to scale up with minimal or no adverse effects. 51 Post-procedure care will also return at a lower cost compared to sedation. 52 A strength of this meta-analysis is the wide array of studies included from western and eastern clinical settings ensuring wide representation of patient populations.
The sub-analysis of distraction techniques provided further supportive conclusions which can be inferred which may help improve pain and anxiety when implementing these interventions.
Blinding has been demonstrated to further strengthen the impact of distraction intervention for pain scores. This may be explained by the removal of any bias from both the endoscopist and patient, which may influence the impact of the intervention. Studies without blinding still reported a significant reduction in anxiety scores. A question left to answer is whether blinding will further improve the reduction of anxiety scores.
Patients who have undertaken a previous colonoscopy also demonstrated a greater impact from distraction. This may be as a result of previous experience with the procedure and the familiarity on the day, allowing the unknown aspects of an experience not to apply which will impact pain and anxiety.
Patients who did not undertake sedation compared to those who did reported a superior improvement in pain and anxiety with distraction techniques. This may be due to the patient being conscious and so with their cognition not being impaired, the distraction interventions were able to be more effective. Sedation is a confounding factor that should be highlighted, as this will have a knock-on effect on how music and distraction techniques are perceived by the patient, given the sedatory effect. It will also be a contributor to the reduction of pain and anxiety and therefore separating its effect from the interventions of music and distraction becomes more complex.
Patients who undertook endotherapy also reported a superior impact on pain and anxiety compared to those who did not. This may be due to a longer procedure, due to therapy being undertaken and therefore more time for the effect of the distraction technique to be applied. Audio-visual had a greater effect on pain and anxiety scores compared to visual alone and this is possibly due to the synergistic effect of both an audio and visual distraction modality being applied simultaneously.
There was a wide variability in study design for the music RCTs. The range of musical genres implemented was diverse and when patients were given a choice of music, this was demonstrated to be non-superior to pre-selected music by the study.15,16,32–40 The mode of music delivery varied between headphones and speaker output, with no clear method demonstrated to be significantly superior. The possible advantage of headphones is the ability to undertake blinding within the study. The disadvantage is reduced verbal communication with the patient, such as during position change requests. Speaker output for music could also prove distracting to the medical team. The duration of music or task distraction exposure was not explicitly outlined in all the studies, with the timing of music or distraction mostly commencing at the start of the procedure. Further analysis in this area may provide an optimum time to commence an intervention that has not been discovered. Two of the 11 music studies and 8 of the 12 distraction studies used no sedation and reported improvement in pain and anxiety, suggesting a positive impact that is not only reliant on sedative and analgesic medication.
Sensitivity analysis
In this study, the subgroup analysis was used as the sensitivity analysis to ensure robust findings across the various patient cohorts. This was to address the I² values for all meta-analyses in this study, exceeding 80%, indicating substantial heterogeneity. Additionally, certain trials display exceptionally large effect sizes, and the sub-analysis has highlighted how this, however, does not significantly influence the overall results and therefore enhances the reliability of the study findings.
Limitations
Some difficulties in the analysis included studies in which the STAI anxiety score scale varied in range and studies that did not explicitly provide scores and ranges of scores. Similar to previous meta-analyses undertaken with music, there was high heterogeneity present across the analysis which was also present for distraction. Possible explanations are regional variation, such as age and co-morbidities, methodology with music choice/distraction technique and lack of blinding in studies. The distribution from the funnel plot performed for publication bias (Figure 25) is reasonably symmetrical, with a few studies outside the funnel, which may suggest a minor publication bias or heterogeneity. Another limitation in the meta-analysis of distraction studies is the double use of controls to perform a pairwise comparison for RCTs with more than one intervention. This may affect the independent data and pooled estimates. However, the authors feel the conclusions drawn are still valid without this adding significantly to the heterogeneity and bias. A further limitation is where required missing data was imputed, such as the standard deviation during statistical analysis. The study quality was also impacted by the Jaded score for music, with few studies scoring 2 or less. The studies on distraction include a variety of distraction techniques and a question that is raised is the impact of distraction overall versus a specific type of distraction technique being utilised. Lastly, whilst an aim for low bias in the analysis was planned by using only RCT studies, the authors are aware of possible non-randomised studies that could have been utilised in addition to contribute to these findings.
Considerations for future studies include controlling for variables and taking the best performing information available from previous similar studies, such as music/distraction choice, duration, and delivery method. Potential areas of further research include exploring optimal duration and type of music or type of distraction technique. Future studies could also consider randomisation to be undertaken alongside blinding for the patient and endoscopist. The effect on supporting staff and the endoscopist themselves is an additional area to explore in future work, such as the effect of music on endoscopists and support staff in relation to concentration and relaxation. Finally, economic analysis of the scalability of these interventions will be crucial to add further evidence to the potential cost-saving benefits and implementation capability.
Conclusion
This systematic review and meta-analysis have demonstrated a potential role for music and task distraction to improve pain and anxiety for patients undergoing a colonoscopy. The use of such interventions can be in addition to or exclusively utilised during a colonoscopy. It also provides an alternative safe option for patients who may not be eligible for sedation. Whilst evidence is still not directly comparable, it is plausible for the claim of establishing in daily clinical practice.
This meta-analysis utilising studies from both western and eastern cultures allows a better understanding to develop tools and methods to influence pain and anxiety for all patient groups, taking into consideration all cultural differences. In addition, the heterogeneity reflects daily practice with similarities in varying cultures and patient demographics that will be encountered in real-world applications.
As there are no comparative studies looking at task distraction versus music intervention, in the absence of a trial which formally randomises the three arms of task distraction, music and control, this meta-analysis has reported uniquely the nearest results from the data that reflect real-world practice.
Future recommendations to strengthen future studies include increasing patient recruitment to ensure adequate power and decreasing the risk of bias, controlling for variables that may have a confounding factor on results, such as music choice, sedation choice and dosage, and finally conducting studies in a randomised manner with blinding.
Supplemental Material
sj-docx-1-tag-10.1177_17562848251378236 – Supplemental material for The effect of music and distraction on pain and anxiety during colonoscopy: a systematic review and meta-analysis
Supplemental material, sj-docx-1-tag-10.1177_17562848251378236 for The effect of music and distraction on pain and anxiety during colonoscopy: a systematic review and meta-analysis by Jabed F. Ahmed, Hutan Ashrafian, Ara Darzi, Ferdinando R. Baena and Nisha Patel in Therapeutic Advances in Gastroenterology
Supplemental Material
sj-docx-2-tag-10.1177_17562848251378236 – Supplemental material for The effect of music and distraction on pain and anxiety during colonoscopy: a systematic review and meta-analysis
Supplemental material, sj-docx-2-tag-10.1177_17562848251378236 for The effect of music and distraction on pain and anxiety during colonoscopy: a systematic review and meta-analysis by Jabed F. Ahmed, Hutan Ashrafian, Ara Darzi, Ferdinando R. Baena and Nisha Patel in Therapeutic Advances in Gastroenterology
Supplemental Material
sj-docx-3-tag-10.1177_17562848251378236 – Supplemental material for The effect of music and distraction on pain and anxiety during colonoscopy: a systematic review and meta-analysis
Supplemental material, sj-docx-3-tag-10.1177_17562848251378236 for The effect of music and distraction on pain and anxiety during colonoscopy: a systematic review and meta-analysis by Jabed F. Ahmed, Hutan Ashrafian, Ara Darzi, Ferdinando R. Baena and Nisha Patel in Therapeutic Advances in Gastroenterology
Supplemental Material
sj-docx-4-tag-10.1177_17562848251378236 – Supplemental material for The effect of music and distraction on pain and anxiety during colonoscopy: a systematic review and meta-analysis
Supplemental material, sj-docx-4-tag-10.1177_17562848251378236 for The effect of music and distraction on pain and anxiety during colonoscopy: a systematic review and meta-analysis by Jabed F. Ahmed, Hutan Ashrafian, Ara Darzi, Ferdinando R. Baena and Nisha Patel in Therapeutic Advances in Gastroenterology
Footnotes
References
Supplementary Material
Please find the following supplemental material available below.
For Open Access articles published under a Creative Commons License, all supplemental material carries the same license as the article it is associated with.
For non-Open Access articles published, all supplemental material carries a non-exclusive license, and permission requests for re-use of supplemental material or any part of supplemental material shall be sent directly to the copyright owner as specified in the copyright notice associated with the article.