
Abstract
Background:
Disease extent of ulcerative colitis (UC) is dynamic, often shows progression or regression over time. However, factors associated with disease progression in long-term follow-ups remain underexplored.
Objectives:
This study aimed to examine disease extent progression in Chinese patients in a long-term follow-up cohort and identify associated risk factors.
Design:
Retrospective analysis.
Methods:
We retrospectively analyzed 800 hospitalized UC patients from 1980 to 2021, and followed up to December 2023. The disease extent was categorized according to the Montreal classification. The Cox regression model was used to identify factors associated with progression.
Results:
At diagnosis, 19.1% had E1 (ulcerative proctitis), 29.8% had E2 (left-sided UC), and 51.1% had E3 (extensive UC). By the end of follow-up, the proportion of maximum disease extent of E3 cases increased to 74.9%, while E1 and E2 patients decreased to 6.6% and 18.5%, respectively. Cox regression analysis revealed that patients with a history of appendectomy before the onset of disease were at higher risk of disease progression in those initially diagnosed with E1. Lower usage of glucocorticoids, immunosuppressants, and biologics were found in progression to the E3 group than initial E3 group. Lower usage of immunosuppressants and biologics before progression were found in the progressed to E3 group than not progressed to E3 group.
Conclusion:
Disease extent progression was common in Chinese UC patients. We suggest the necessity of aggressive treatment strategies, especially for early-stage UC patients, to mitigate disease progression and reduce the risk of related complications.
Introduction
Ulcerative colitis (UC) is a chronic inflammatory bowel disease characterized by recurrent abdominal pain, diarrhea, mucus, and bloody stools. It is a long-term condition that can relapse throughout a patient’s life, with inflammation extending from the rectum to the various portions of the colon. The extent and severity of the disease fluctuate between episodes. 1
The management of UC relies on a thorough evaluation of several factors, including the extent of disease, activity scores, complications, and previous treatment responses. The Montreal classification system, the first established tool for assessing disease extent, categorizes UC into three subgroups: E1 (ulcerative proctitis, CP), where inflammation is limited to the rectum; E2 (left sided UC), where inflammation affects the colon up to the splenic flexure; and E3 (extensive UC), where inflammation extended beyond the splenic flexure. 2 Another classification system simplifies the categorization into distal colitis, treatable with enemas, and extensive colitis. 3 These classification systems are crucial in guiding treatment decisions, as different categories of UC require tailored therapeutic approaches. However, the disease extent is dynamic over time, with both progression and regression frequently observed.
Although the incidence of UC is rising in Asia, few studies have explored how the disease extent evolves over time in Asian populations. Phenotypic differences between Asian and Caucasian UC patients have been observed. A retrospective Chinese cohort study reported that 72.5% of patients had limited UC (E1 or E2), whereas 27.5% of patients were diagnosed with E3 at the time of diagnosis. The cumulative rate of disease extension was 9.9%, 14.9%, 19.6%, 24.6%, and 30.5% at 1, 2, 3, 4, and 5 years after diagnosis. 4 By contrast, a European study found that 61% of patients had limited UC and 21% experienced disease progression during follow-up. 5
Studies have also demonstrated that the extent of UC is associated with severity, prognosis, and the response to pharmacological treatment. For example, distal/left-sided colitis is associated with a higher likelihood of clinical remission, while extensive colitis shows a negative association with remission induction in patients treated with vedolizumab. 6 Moreover, extensive UC is associated with worse outcomes, including a higher risk of colorectal cancer and the need for stronger medications or more aggressive treatments, such as colectomy. 7
There is a scarcity of real-world data focusing on the long-term clinical features of UC patients in China. This study aims to examine the trends in disease extent evolution and identify risk factors associated with progression, to improve management strategies for high-risk UC patients.
Methods
Ethical considerations
This study was approved by the Ethical Committee of Peking Union Medical College Hospital (PUMCH; No. ZS-3563D). Written informed consent was obtained from each participant at admission.
Study design and patients
We performed a single-center retrospective study of all hospitalized patients diagnosed with UC at PUMCH, with complete follow-up data were consecutively enrolled from January 1980 to December 2021. UC diagnosis was based on a comprehensive evaluation of clinical, imaging, endoscopic, and histological investigations, following the contemporary Chinese 8 and European UC consensus guidelines. 9 Patients were excluded if they had incomplete clinical data, declined follow-up, or if disease extent progression could not be determined. The reporting of this study conforms to the Strengthening the Reporting of Observational Studies in Epidemiology (STROBE) statement. 10
Data collection, follow-up protocol, and definitions
Demographic information (age at diagnosis, sex) and personal habits (smoking status and drinking) were collected. Clinical classifications followed the Montreal Classification. Disease extent, extraintestinal manifestations, complications (e.g., massive gastrointestinal bleeding, intestinal obstruction, perforation, or toxic megacolon), surgeries (e.g., previous gastrointestinal surgery before diagnosis and UC-related surgery), medical treatment (e.g., glucocorticoids, immunosuppressants, biologics, and small-molecule drugs), development of cancers, and mortality of the cohort were documented and analyzed at diagnosis and during follow-up.
A dedicated team was responsible for patient follow-ups. For patients who regularly visited clinics, the previously mentioned information was collected via an electronic database. For others, the team collected follow-up information by contacting the patients or their relatives by phone, and recorded the data into the electronic database. The most recent follow-up was completed in December 2023.
The extent of disease in UC was defined according to the Montreal classification. Disease extent at diagnosis was the initial diagnosis made at any hospital at the onset of the disease. Disease extent progression was defined as exceeding of maximum disease extent during follow-up to disease extent from diagnosis, such as CP (E1) at diagnosis progressing to left sided UC (E2) or extensive UC (E3) during follow up, or left sided UC (E2) at diagnosis progressing to extensive UC (E3) during follow up, based on endoscopic results. If no progression was observed, this condition was defined as disease extent perseverance. Patients initially diagnosed with E3 were excluded from the analysis of factors related to disease extent progression.
Statistical analysis
Continuous variables are shown as the mean ± standard deviation (x¯ ± s) or median (interquartile range, IQR), depending on whether they satisfied a normal distribution. Univariate analysis was performed by Student’s t test or the Mann–Whitney U test. Categorical variables are expressed as frequencies (%), and univariate analysis was performed by the Chi-square test (or Fisher’s exact test). Disease extent progression was evaluated using Cox regression analysis. All significance tests were two-tailed, with a p value < 0.05 considered statistically significant. SPSS 26.0 (IBM Corporation, Chicago, IL, USA) was used for data analysis. The Sankey diagram was generated using R 4.3.1 statistical software (The R Foundation for Statistical Computing, Vienna, Austria).
Results
Disease extent characteristics and evolution of the cohort
There were 806 patients diagnosed with UC during the study period. Six patients were excluded due to incomplete medical records or refusal to follow up, leaving 800 UC patients enrolled in our study. The flowchart and design of this study are shown in Figure 1. Among them, 431 were males and 369 were females, with a median age at diagnosis of 37 years (IQR: 27–49). The median follow-up time was 12.4 years (IQR: 9.3–16.4). The proportions of E1, E2, and E3 patients were 19.1%, 29.8%, and 51.1%, respectively, at diagnosis. By the end of follow-up, the maximum disease extent proportion of E3 patients increased to 74.9%, while E1 and E2 patients decreased to 6.6% and 18.5%, respectively (Figure 2). The median time of colonoscopy procedures that show disease progression was 3.0 years (IQR: 1.0–6.7). Table 1 shows the demographic and clinical features of the cohort at diagnosis and during follow-up.

Flow chart and design of this study.

Sankey diagram for the transition of disease classification in UC patients.
Demographic and clinical features of the cohort at diagnosis and during follow-up.
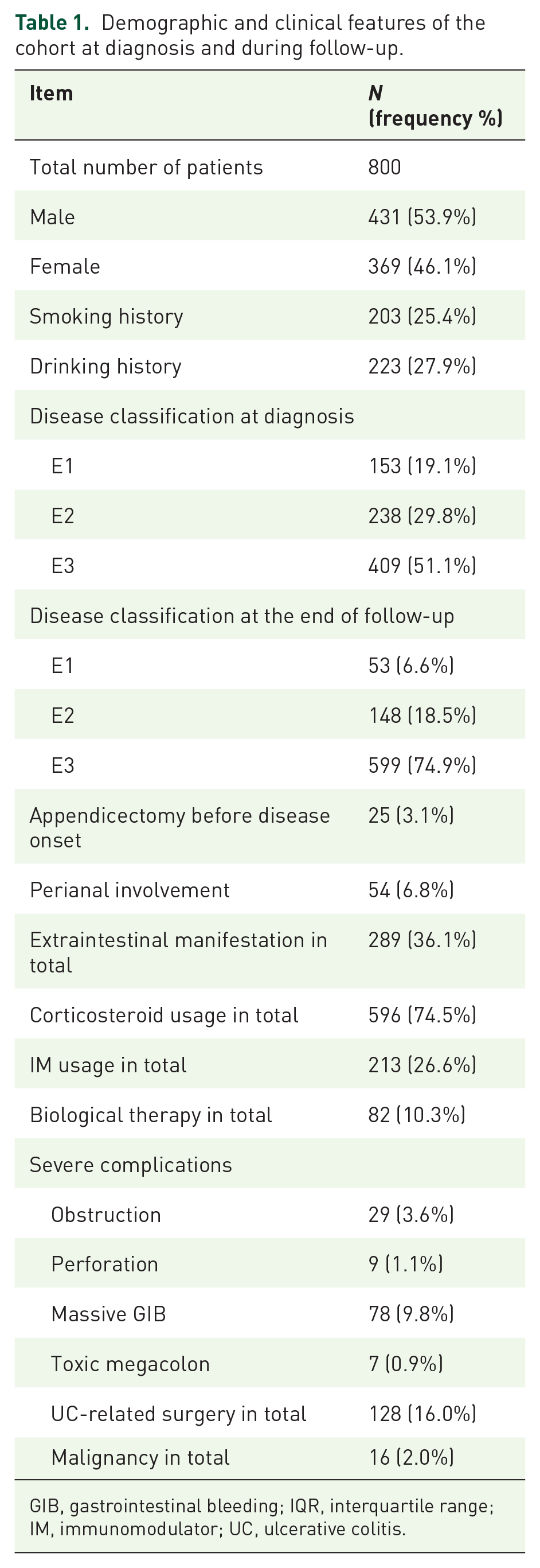
GIB, gastrointestinal bleeding; IQR, interquartile range; IM, immunomodulator; UC, ulcerative colitis.
Extraintestinal manifestations were reported by 289 (36.1%) during follow-up, and 54 (6.8%) experienced perianal involvement. Severe complications occurred in the following proportions: 29 patients (3.6%) had intestinal obstruction, 9 patients (1.1%) experienced perforation, 78 patients (9.8%) had massive gastrointestinal bleeding, and 9 patients (1.1%) developed toxic megacolon. In total, 128 (16.0%) patients experienced UC-related surgery, and 16 (2.0%) patients developed malignant tumors during follow-up.
Risk factors for disease extent progression in initially diagnosed E1 patients
Of the 153 patients initially diagnosed with E1, 53 remained as E1 during follow-up, while 22 progressed to E2 and 78 progressed to E3. Cox multivariate analysis revealed that patients with a history of appendectomy prior to disease onset had a significantly higher risk of disease extent progression than those without such a history (hazard ratio (HR) 13.35, 95% confidence interval (CI) 3.70–48.14, p < 0.001; Table 2 and Figure 3).
Multivariate Cox model analysis of influence risks for disease extent progression of E1.

CI, confidence interval; HR, hazard ratio; IM, immunomodulator.
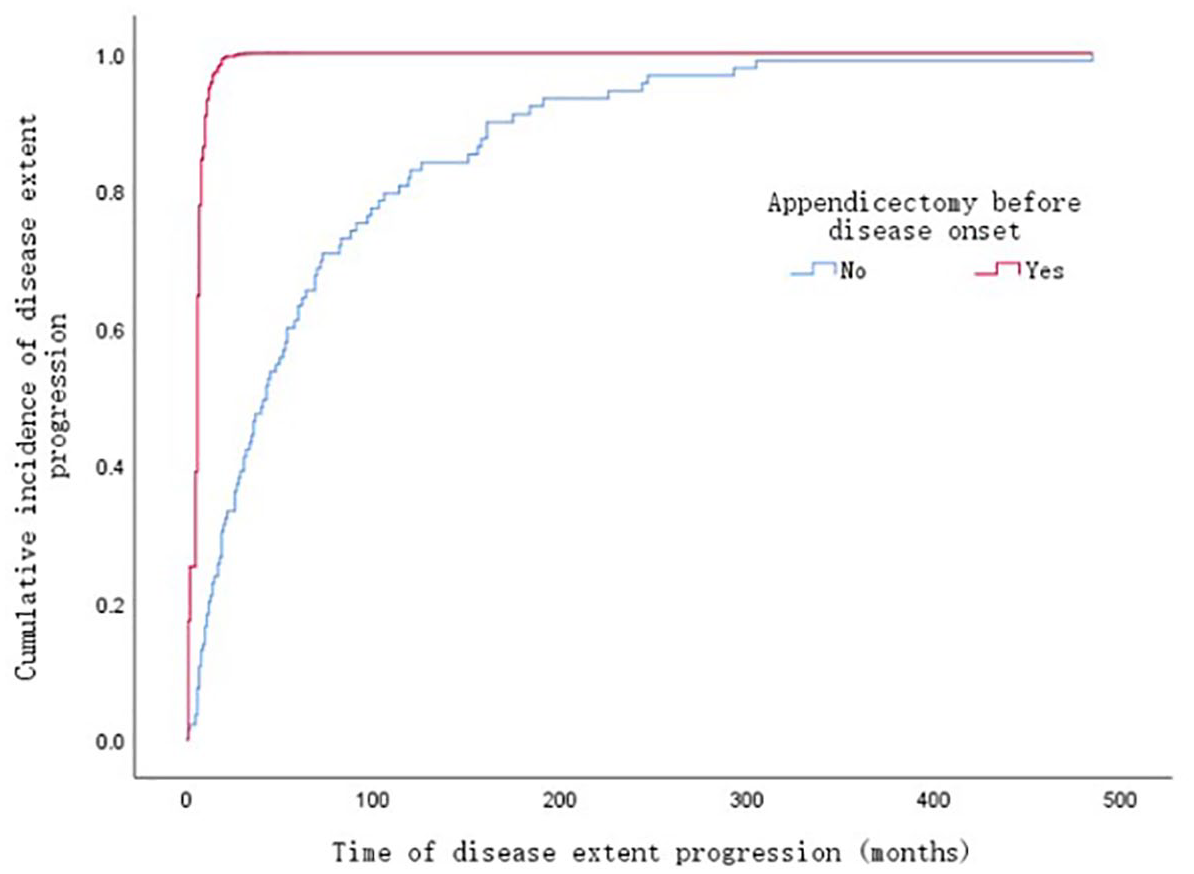
Cumulative incidence of disease extent progression in patients initially diagnosed with E1.
Risk factors for disease extent progression in initially diagnosed E1 and E2 patients
Among the 153 E1 and 238 E2 patients at initial diagnosis, 212 experienced disease extent progression during follow-up. The median time of disease extent progression was 2.8 years (IQR: 0.9–5.8) in initially diagnosed E1 patients, and the median time of disease extent progression was 3.9 years (IQR: 1.1–7.8) in initially diagnosed E2 patients. There was no difference in the time of disease extent progression between initially diagnosed E1 and E2 patients (p = 0.258). However, Cox regression analysis did not identify any significant risk factors associated with disease extent progression in this group (Table 3).
Multivariate Cox model analysis of influence risks for location progression in total.

CI, confidence interval; HR, hazard ratio; IM, immunomodulator.
Differences between patients initially diagnosed with E3 and those who progressed to E3
To explore whether there were differences between patients initially diagnosed with E3 and those who progressed to E3 during follow-up, the 599 patients diagnosed with E3 were divided into two groups: The initial E3 group (N = 409) and the progression to E3 group (N = 190). Univariate analysis illustrated that the proportion of male patients and patients with a history of smoking was lower in the progression to the E3 group (p = 0.008 and 0.028, respectively). In addition, the use of systemic glucocorticoids, immunosuppressants, and biologics before disease progression were significantly lower in the progression to the E3 group (p < 0.001). However, no significant difference was observed in medical treatment between the two groups during the overall follow-up. Similarly, there were no statistical differences in complications, extraintestinal manifestations, and UC-related surgeries between the two groups (Table 4).
Differences between patients initially diagnosed with E3 and those who progressed to E3 at the end of follow-up.

GIB, gastrointestinal bleeding; IQR, interquartile range; IM, immunomodulator; UC, ulcerative colitis.
Differences between patients who progressed to E3 and did not progress to E3 at the end of follow-up
To identify risk factors for progression to E3, patients initially diagnosed with E1 and E2 were divided into two groups: Not progressed to E3 (N = 201) and progressed to E3 (N = 190) at the end of follow-up. Progressed to E3 group was younger, with a median age of 33 (26, 46) years than not progressed to E3 group, which had a median age of 39 (28, 52) years (p = 0.003), had a higher rate of perianal disease (8.0% vs 3.0%, p = 0.014), and a higher rate of UC-related surgery (20.0% vs 5.0%, p < 0.001). The percentages of immunomodulator usage, biological therapy before progression were lower in progressed to the E3 group, p = 0.022 and 0.007, respectively. The overall rates of corticosteroid usage, immunomodulator usage, and biological therapy were higher in the progressed to E3 group, p < 0.001, p < 0.001, and p = 0.005, respectively. There were no statistical differences in extraintestinal manifestations and other complications between the two groups (Table 5).
Differences between patients progressed to E3 and not progressed to E3 at the end of follow-up.

GIB, gastrointestinal bleeding; IM, immunomodulator; IQR, interquartile range; UC, ulcerative colitis.
Discussion
This is a large-scale, single-center, real-world study that provides valuable insights into the evolution of disease extent in Chinese UC patients. First, we found that E3 accounted for the majority of hospitalized UC patients, and the proportion of E3 increased as the duration of the disease course. Second, disease extent progression was common; more than half of the initially diagnosed E1 and E2 patients experienced disease extent progression during follow-up. Third, patients with a history of appendectomy before disease onset had a higher risk of disease extent progression in E1 patients. Finally, male patients and smokers were less likely to progress to E3. In addition, lower usage rates of systemic glucocorticoids, immunosuppressants, and biologics were associated with disease extent progression to E3.
The progression of disease extent was common in UC patients. Previous population-based studies reported that disease extension from the initial location occurred in 10%–19% of patients after 5 years and in 11%–28% after 10 years. 11 In a recently published Chinese cohort, 57% experienced disease extent progression in a median follow-up duration of 5.3 years. 12 In a retrospective Asian cohort study, 17.6% of patients experienced proximal disease extension over a median follow-up of 7.5 years. 4 A meta-analysis reported the overall rate of UC extension was 22.8%, with colonic extension being 17.8% at 5 years and 31% at 10 years. Extensions from E1 to E3, E2 to E3, and E1 to E2 occurred at rates of 17.8%, 27.5%, and 20.8%. 13 Since pancolitis is associated with higher relapse and hospitalization rates, 14 identifying risk factors for UC progression is crucial for improving clinical outcomes.
Montreal E1 refers to the involvement limited to the rectum. In our study, patients with a history of appendectomy before UC onset had a higher risk of disease extent progression in those initially diagnosed with E1. While the appendix is thought to have a role in the pathogenesis of UC, the nature and basis of this association remain unclear. 15 Appendectomy before diagnosis may affect the course and outcome of the disease, potentially reducing the need for colectomy but increasing the risk of colorectal cancer. 16 Although recent meta-analyses suggest that appendectomy does not affect disease progression, 17 inconsistencies in findings may arise from differences in study design and adjustments for confounding factors. To better understand this relationship, it is essential to explore the underlying mechanisms that may link appendectomy and UC progression. One possibility is the crucial role of the appendix in the generation of immunoglobulin A (IgA)-producing B cells that colonize the colon. A reduction in these cells could predispose individuals to IBD. 18 IgA is thought to protect against a colitogenic microbiome, 19 so patients with UC may possess an abnormal repertoire of IgA-producing B cells that inadvertently foster the development of a colitogenic microbiome. This could explain the link between appendectomy and disease progression in E1 patients, as reduced IgA production and microbiota dysbiosis may contribute to worsened outcomes. 20 Despite these insights, major questions about the role of the appendix in the pathogenesis of UC remain unresolved, highlighting the need for further research to clarify the clinical significance of this association.
Although disease extent is frequently used as a measure of severity, distal UC does not always result in less disability than extensive disease. While distal UC may involve a more limited area of the colon, it does not guarantee a milder course, as patients can still progress to more extensive disease over time. 21 Symptomatically, patients with distal UC may experience symptoms that are just as severe, or even more burdensome, than those with extensive disease, which significantly impair patients’ health-related quality of life. This is largely due to the nature of rectal inflammation, which is strongly associated with some of the most disruptive symptoms of UC, such as urgency, tenesmus, and incontinence. 22 Despite these debilitating symptoms, managing UP remains a significant challenge for gastroenterologists. 23 UP is frequently excluded from clinical trials, which contributes to an underestimation of its disease burden in both research and clinical practice. As a result, UP patients are often undertreated, leaving them to endure persistent symptoms and complications. Approximately one-third of UP patients require advanced therapies during their disease course, and biologic treatments are necessary for those with refractory or steroid-dependent cases of UP. 24
By contrast, Montreal E3, or extensive colitis, involves inflammation extending beyond the splenic flexure. Our study revealed that compared to those initially diagnosed as the E3 group, patients who progressed to E3 were less likely to be male or have a history of smoking compared to those initially diagnosed with E3. Smoking, though generally discouraged for health reasons, appears to have a paradoxical protective effect in UC. However, evidence regarding smoking’s impact on hospitalization rates, colectomy, and the need for oral corticosteroids or immunosuppressants is conflicting, and further research is needed to clarify this relationship. 25
Another significant factor in disease progression to E3 is treatment usage. In our cohort, patients who progressed to E3 had lower rates of systemic glucocorticoids, immunosuppressants, and biologics usage prior to their progression. This suggests that insufficient early intervention may contribute to disease progression. Research indicates that patients initially diagnosed with distal UC will develop more extensive disease over time, with rates of progression exceeding 50% over 25 years. 26 Disease progression is also associated with a higher incidence of extraintestinal manifestations, a corticosteroid-refractory course, and a greater need for immunosuppressants and biologics compared to those with distal colitis. 27 These findings emphasize the importance of intensified treatment strategies for patients with E1/E2 UC.
In our cohort, 54 (6.8%) patients experienced perianal involvement during follow-up. Perianal disease in inflammatory bowel disease has always been linked to Crohn’s disease. However, it could occasionally be seen in UC patients. In a case–control study, 5% of UC patients developed perianal disease, being more frequent among men (62%), with distal (50%) or extent (34%) disease. 28 In another hospital-based cohort, the cumulative probabilities of perianal disease at 1, 5, 10, and 20 years after UC diagnosis were 1.0%, 2.3%, 4.0%, and 6.3%, respectively. 29 The frequency of patients with UC exhibiting perianal lesions rose in correlation with an extended diagnostic duration.
There were several limitations to our study. First, as a retrospective, single-center study, it may introduce biases such as selection and recall bias, limiting control over confounding variables that could affect the interpretation of disease progression risk factors. And findings derived from a hospital-based cohort may exhibit bias and may not represent all outpatients and inpatients. However, because our study consecutively enrolled patients over a long period, we experienced a low dropout rate, which enhances the representativeness of our findings. Second, the data collection spanned from 1980 to 2021, a period during which treatment protocols and therapeutic options, including the use of biologics and immunosuppressants, have significantly evolved. As a result, patients from earlier years may not have had access to these newer treatments, potentially impacting disease progression outcomes. In addition, we did not calculate disease extent progression rate annually during this relatively long follow-up time, and the disease extent of UC may vary over time with the advent of novel therapeutic agents. To address these limitations, future research should prioritize prospective, multicenter studies to minimize biases and provide clearer insights into disease dynamics. Furthermore, assessing annual disease progression rates in future studies will be crucial in understanding the timing and effects of modern treatment strategies on disease extent.
Conclusion
UC is a dynamic disease, and disease extent progression is common in Chinese UC patients. Patients with a history of appendectomy before the onset of disease had a higher risk of disease extent progression in E1 patients. Lower usage of glucocorticoids, immunosuppressants, and biologics was found in progression to the E3 group than initial E3 group. Lower usage of immunosuppressants and biologics before progression was found in the progressed to E3 group than in not progressed to E3 group. These findings suggest the need for aggressive treatment strategies, particularly for patients with early-stage UC, to mitigate progression and associated complications.
Supplemental Material
sj-docx-1-tag-10.1177_17562848251339878 – Supplemental material for Progressing or preserving, disease extent evolution in hospitalized patients with ulcerative colitis in China: a real-world study
Supplemental material, sj-docx-1-tag-10.1177_17562848251339878 for Progressing or preserving, disease extent evolution in hospitalized patients with ulcerative colitis in China: a real-world study by Yinghao Sun, Gechong Ruan, Mingyue Guo, Yuge Wei, Xiaoyin Bai, Wei Han, Bei Tan, Ji Li, Yue Li, Hong Yang and Jiaming Qian in Therapeutic Advances in Gastroenterology
Supplemental Material
sj-docx-2-tag-10.1177_17562848251339878 – Supplemental material for Progressing or preserving, disease extent evolution in hospitalized patients with ulcerative colitis in China: a real-world study
Supplemental material, sj-docx-2-tag-10.1177_17562848251339878 for Progressing or preserving, disease extent evolution in hospitalized patients with ulcerative colitis in China: a real-world study by Yinghao Sun, Gechong Ruan, Mingyue Guo, Yuge Wei, Xiaoyin Bai, Wei Han, Bei Tan, Ji Li, Yue Li, Hong Yang and Jiaming Qian in Therapeutic Advances in Gastroenterology
Footnotes
Appendix
Differences between patients diagnosed in 2005 or before and post 2005.

| Item | Cohort 1 (n = 164) | Cohort 2 (n = 636) | p Value |
|---|---|---|---|
| Male | 84 (51.2%) | 347 (54.6%) | 0.444 |
| Disease classification at diagnosis | <0.001 | ||
| E1 | 39 (23.8%) | 114 (17.9%) | |
| E2 | 68 (41.5%) | 170 (26.7%) | |
| E3 | 57 (34.8%) | 352 (86.1%) | |
| Disease classification at the end of follow-up | 0.142 | ||
| E1 | 11 (6.7%) | 42 (6.6%) | |
| E2 | 39 (23.8%) | 109 (17.1%) | |
| E3 | 114 (69.5%) | 485 (76.3%) | |
| Extraintestinal manifestation in total | 49 (29.9%) | 198 (31.1%) | 0.757 |
| Severe complications | |||
| Obstruction | 7 (4.3%) | 22 (3.5%) | 0.621 |
| Perforation | 1 (0.6%) | 8 (1.3%) | 0.695 |
| Toxic megacolon | 0 (0.0%) | 7 (1.1%) | 0.355 |
| Massive GIB | 13 (7.9%) | 65 (10.2%) | 0.377 |
| UC-related surgery in total | 28 (17.1%) | 100 (15.7%) | 0.674 |
GIB, gastrointestinal bleeding; UC, ulcerative colitis.
Acknowledgements
None.
Declarations
Supplemental material
Infliximab (IFX) entered Chinese market in 2006, receiving initial approval for treating CD and subsequently for UC in 2019. The advent of biologics has notably transformed the therapeutic landscape for UC. Therefore, we categorized patients into two cohorts based on their diagnosis timeline: Cohort 1 included those diagnosed in 2005 or before, while Cohort 2 comprised individuals diagnosed post-2005. We then compared the differences in disease extent, extra-intestinal manifestations and complications between the two groups. We found that the percentage of E3 at diagnosis was higher in cohort 2, while there was no difference in disease classification at the end of follow up between the two cohorts. No difference was found in extra-intestinal manifestation or complications between the two cohorts (Appendix Table). Supplemental material for this article is available online.
References
Supplementary Material
Please find the following supplemental material available below.
For Open Access articles published under a Creative Commons License, all supplemental material carries the same license as the article it is associated with.
For non-Open Access articles published, all supplemental material carries a non-exclusive license, and permission requests for re-use of supplemental material or any part of supplemental material shall be sent directly to the copyright owner as specified in the copyright notice associated with the article.