
Abstract
Background:
Whether patients with inactive ulcerative colitis (UC) have symptoms compatible with functional bowel disorders (FBDs) other than irritable bowel syndrome (IBS) is unclear. Our aim was to investigate the prevalence and burden of these symptoms and determine impact on the UC course.
Methods:
We used Mayo score, sigmoidoscopy and calprotectin (f-cal) to define remission in 293 UC patients. Presence of symptoms compatible with FBD, severity of gastrointestinal, extraintestinal and psychological symptoms, stress levels and quality of life (QoL) were measured with validated questionnaires. At 1 year later, remission was determined by modified Mayo score and f-cal in 171 of these patients. They completed the same questionnaires again.
Results:
A total of 18% of remission patients had symptoms compatible with FBD other than IBS, and 45% subthreshold symptoms compatible with FBD. The total burden of gastrointestinal symptoms in patients with symptoms compatible with FBD was higher than in patients without FBD (p < 0.001), which had negative impact on QoL (p = 0.02). These symptoms were not correlated with psychological distress, systemic immune activity or subclinical colonic inflammation and were not a risk factor for UC relapse during follow up.
Conclusion:
Symptoms compatible with FBD other than IBS are common during UC remission influencing patients’ QoL but not the UC course.
Keywords
Introduction
Ulcerative colitis (UC), an inflammatory bowel disease (IBD) of the colon, 1 is characterized by remission periods and relapses with an unpredictable disease course. 2 Relapses are associated with bloody diarrhea, abdominal discomfort and urgency, generated by the colonic inflammation. Thus, it would be expected that patients were symptom-free during remission. However, a substantial proportion demonstrate symptoms resembling irritable bowel syndrome (IBS) 3 or other functional bowel disorders (FBDs). 4
FBDs are functional gastrointestinal (GI) disorders with symptoms attributable to the lower GI tract, including IBS, functional bloating, functional constipation and functional diarrhea. Diagnostic criteria define FBD, taking not only the nature but also the frequency and duration of symptoms into consideration. 5 Furthermore, there are subjects with symptoms characteristic of FBD but without sufficient duration or frequency to be diagnosed with a specific FBD. These ‘subthreshold’ symptoms still constitute a clinical problem.
The pathogenesis of symptoms compatible with FBD in inactive UC is unknown. There is, however, growing evidence regarding possible underlying mechanisms. 6 Clinically undetected low-grade inflammation, 7 changes after the resolution of the inflammation resulting in epithelial barrier disruption, 8 sensorimotor dysfunction 9 and visceral hypersensitivity, 10 and other factors along the brain–gut axis, for example, gut microbiota 11 and psychological factors, 12 have been suggested as important.
The prevalence of IBS-like symptoms during UC remission is reported to be 31%. 13 Symptoms compatible with FBDs other than IBS in quiescent UC are a common clinical problem but only a few studies have evaluated them. These report a prevalence of 36–42%.4,14 To our knowledge, no reports on the presence of subthreshold symptoms compatible with FBD in inactive UC are available. Finally, studies have been cross-sectional and whether symptoms compatible with FBD during remission influence the UC course has not been evaluated.
Our group recently reported a prevalence of 18% of IBS-like symptoms according to Rome III criteria in a cohort with inactive UC. 12 In the present study, we evaluated the same cohort, with the aim of describing the prevalence of symptoms compatible with FBDs other than IBS in inactive UC, study the burden of these symptoms and development over time, and determine impact on the UC course. The analysis of the prevalence and burden of FBDs other than IBS in inactive UC is based on the same study procedures as in our previously published study. 12 However, the analysis of the development of these symptoms over time and their impact on the UC course is based on a totally new follow-up investigation on the same cohort.
Methods
Subjects
Patients were recruited from four IBD units in the Västra Götaland region between September 2012 and April 2014. Adults with a UC diagnosis were eligible. Patients with other significant diseases, for example, malignancy, were excluded. Patients gave their written informed consent before participation. Approval was obtained by the Regional Ethical Review Board in Gothenburg (403-12/23 August 2012 and 7658-13/02 September 2013).
Study design
Patients were included during a regular consultation. Information about disease duration and extent according to Montreal classification, 15 medication and other demographic characteristics was collected. Blood samples for hs-CRP (high-sensitive C-reactive peptide) and cytokine analysis and fecal samples for calprotectin (f-cal) analysis were collected. Clinical assessment, including rigid sigmoidoscopy, was performed to grade the disease activity according to Mayo score. 16 Patients with normal rectal mucosa but f-cal > 200 μg/g were examined within 2 weeks with flexible sigmoidoscopy to identify more proximal colonic inflammation. Self-assessment questionnaires to measure GI symptom severity, symptoms compatible with FBDs according to Rome III criteria, stress, psychological distress, non-GI somatic symptom severity and disease-specific quality of life (QoL) were completed.
The second part of the study was a 1-year follow up. Patients completed the same questionnaires. Additionally, they answered questions regarding current disease activity (stool frequency and rectal bleeding components of Mayo score, number of flares during the previous 3 and 12 months) and provided fecal samples for f-cal analysis. The two items of the Mayo score have been validated with good accuracy as appropriate for patient-reported outcomes (PROs) for UC. 17 F-cal was used as surrogate marker of macroscopic colonic inflammation, since f-cal levels correlate well with endoscopic UC activity. 18 Further clinical or endoscopic assessment of the disease activity was not performed at this point.
At inclusion, remission was defined as Mayo score ⩽ 2 with physician global assessment (PGA) = 0, rectal bleeding = 0, endoscopic subscore = 0 and no relapse during the previous 3 months. At follow up, remission was defined as modified Mayo score ⩽ 2 with rectal bleeding = 0, f-cal < 200 μg/g and no self-reported relapse during the previous 3 months.
Questionnaires
For detailed information about questionnaires, please see supplementary material. The GI symptoms severity was assessed with the Gastrointestinal Symptom Rating Scale (GSRS). 19 The FBD presence was determined with the FBD module of the Rome III diagnostic questionnaire 20 which determines if patients meet the criteria for FBD, and functional dyspepsia. Table 1 shows the definitions of FBD and functional dyspepsia according to Rome III criteria. Subthreshold symptoms compatible with FBDs refer to symptoms characteristic of FBD but not sufficient enough to be diagnosed as specific FBD according to Rome III criteria. This term has not previously been used in the literature but was created for the purpose of this study, since these subthreshold symptoms still constitute a clinical problem. The criteria used to define subthreshold FBDs are presented in Table 2. The Patient Health Questionnaire 12 (PHQ-12), a modification of the PHQ-15 after excluding its three gastrointestinal items,21,22 was used to determine the severity of non-GI somatic symptoms. QoL was assessed with the disease-specific IBD Questionnaire (IBD-Q). 23 Psychological distress was evaluated with the Hospital Anxiety/Depression Scale (HADS). 24 Finally, the degree to which subjects perceive life circumstances as stressful was measured with the Perceived Stress Scale (PSS-14). 25
Rome III diagnostic criteria for IBS, other functional bowel disorders (functional diarrhea, functional constipation, functional bloating) and functional dyspepsia.

GI, gastrointestinal; IBS, irritable bowel syndrome.
Subthreshold symptoms compatible with FBD; criteria and prevalence in patients in UC remission at enrollment.
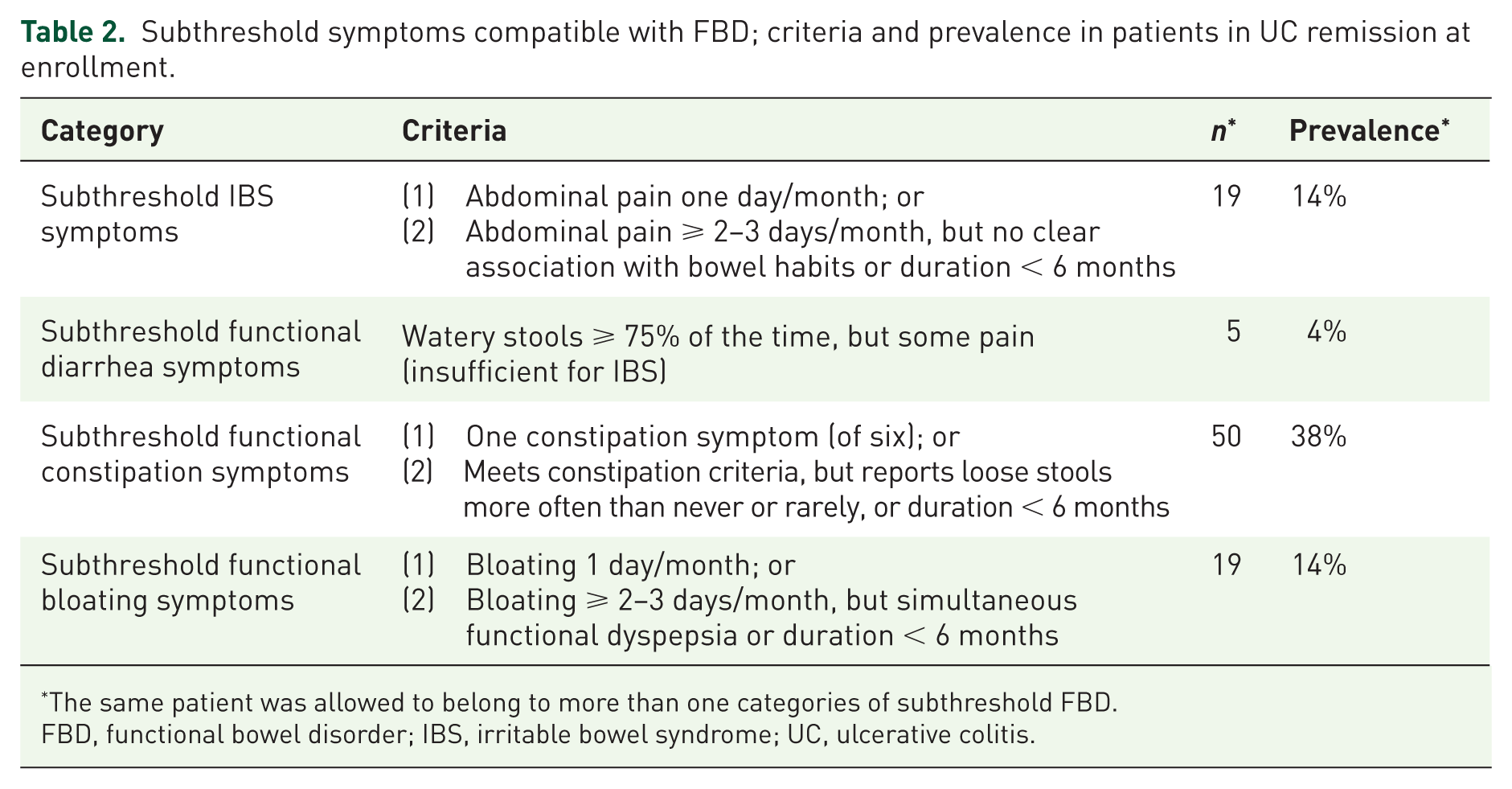
*The same patient was allowed to belong to more than one categories of subthreshold FBD.
FBD, functional bowel disorder; IBS, irritable bowel syndrome; UC, ulcerative colitis.
Laboratory analyses
F-cal was analyzed by sandwich enzyme-linked immunosorbent assay (Calprotectin ELISA; BÜHLMANN Laboratories, Basel, Switzerland) using a monoclonal capture antibody specific for calprotectin. hs-CRP was analyzed by enzyme-linked immunosorbent assay as routine test at the Clinical Immunology Laboratory, Sahlgrenska Hospital, Gothenburg, Sweden. Serum cytokines were measured as markers of systemic immune activity; interleukin (IL)-12p70 and interferon gamma (IFN-γ) as markers of T-helper-cell 1 (Th1)-mediated activity, IL-4, IL-10 and IL-13 as markers of Th2-mediated activity, IL-17A as marker of Th17-mediated activity. Moreover, IL-1β, IL-6, IL-8 and tumor necrosis factor (TNF), reflecting activity of the innate system, were measured. The analyses were performed using the MesoScale Discovery platform (MSD, Rockville, MD, US).
Data analysis
Group classification and comparisons
Patients were divided into four groups according to UC status and whether they fulfilled Rome III criteria for IBS/another FBD. Patients not meeting the remission criteria were classified as UCA (active UC); patients meeting remission (UCR) and IBS criteria as UCR+IBS; patients meeting remission and other FBD than IBS criteria (hence functional bloating, functional constipation or functional diarrhea) as UCR+FBD; and those in remission and not meeting IBS/another FBD criteria as UCR-.
UCR+IBS, UCR+FBD and UCR- groups were compared regarding demographics, disease characteristics, treatment, severity of GI/non-GI somatic symptoms and QoL. Factors that might contribute to the generation of symptoms compatible with FBD other than IBS in remission were investigated by comparing the UCR+FBD and UCR- groups regarding colonic and systemic inflammation, systemic immune activity, psychological distress and perceived stress.
The disease status at follow up with regard to the disease status at enrollment was examined to investigate the stability of symptoms compatible with IBS/another FBD over time. Finally, the UCR+IBS/FBD and UCR- groups were compared concerning modified Mayo score and f-cal at follow up and number of flares during follow up to examine whether symptoms compatible with IBS/another FBD influence the UC course.
Sample-size justification
Based on the data from the literature13,14 and since we applied stricter criteria to define UC remission in our cohort, the expected prevalence of IBS in UC remission in our cohort was 20–25%. The assumed prevalence of FBD other that IBS in UC remission was considered to be equal and approximately 20–25%. Both the prevalence of IBS and this of other FBD than IBS were main questions of the project and thus the sample-size estimation was carried out separately for these two conditions. Moreover, it was expected that about 50% of the cohort would fulfill the UC remission criteria we used. Based on this, a cohort of 300 patients would result in subgroups of about 30 patients, which constitute subgroups of sufficient size for meaningful statistical analyses. 26
Statistics
Categorical data are reported as absolute numbers/percentages and compared using Pearson’s chi-square or Fischer’s exact test. Continuous data are reported as means with standard deviations when parametric and as median with interquartile range when nonparametric. Parametric data were compared with student’s t test and nonparametric with Mann–Whitney U test. Comparisons between groups were performed with analysis of variance for parametric, and Kruskall–Wallis test for nonparametric, data, with post hoc Bonferroni corrections. Statistical analyses were performed using SPSS version 23 (IBM Corp., Armonk, NY, USA).
Results
Study population characteristics and presence of symptoms compatible with FBD
Figure 1 illustrates the number of individuals at each study stage. Out of the individuals who completed the cross-sectional part of the study and were in remission, 24 (18%) fulfilled criteria for FBD other than IBS; functional diarrhea (n = 5), functional constipation (n = 4), functional bloating (n = 15) and as reported previously, 18% had IBS-like symptoms 12 [Figures 1(a) and 2(a)]. Moreover, 45% reported subthreshold symptoms compatible with FBD [Figure 2(b)]. Of those, constipation symptoms were most common (38%), followed by abdominal pain (14%) and bloating (14%; Table 2). Subsequently, only 19% reported no symptoms compatible with FBD or subthreshold FBD symptoms. Additionally, 9% (n = 12) had symptoms compatible with functional dyspepsia (50% belonged to the UCR+IBS group, 50% to UCR-). However, symptoms compatible with functional dyspepsia were not investigated further as the aim of the study was to evaluate FBD, that is, functional gastrointestinal disorders (FGID) attributable to the lower GI tract, which is the target organ in UC. Table 3 shows demographics, disease characteristics and treatment at enrollment for the groups.

Flowchart showing the study design.
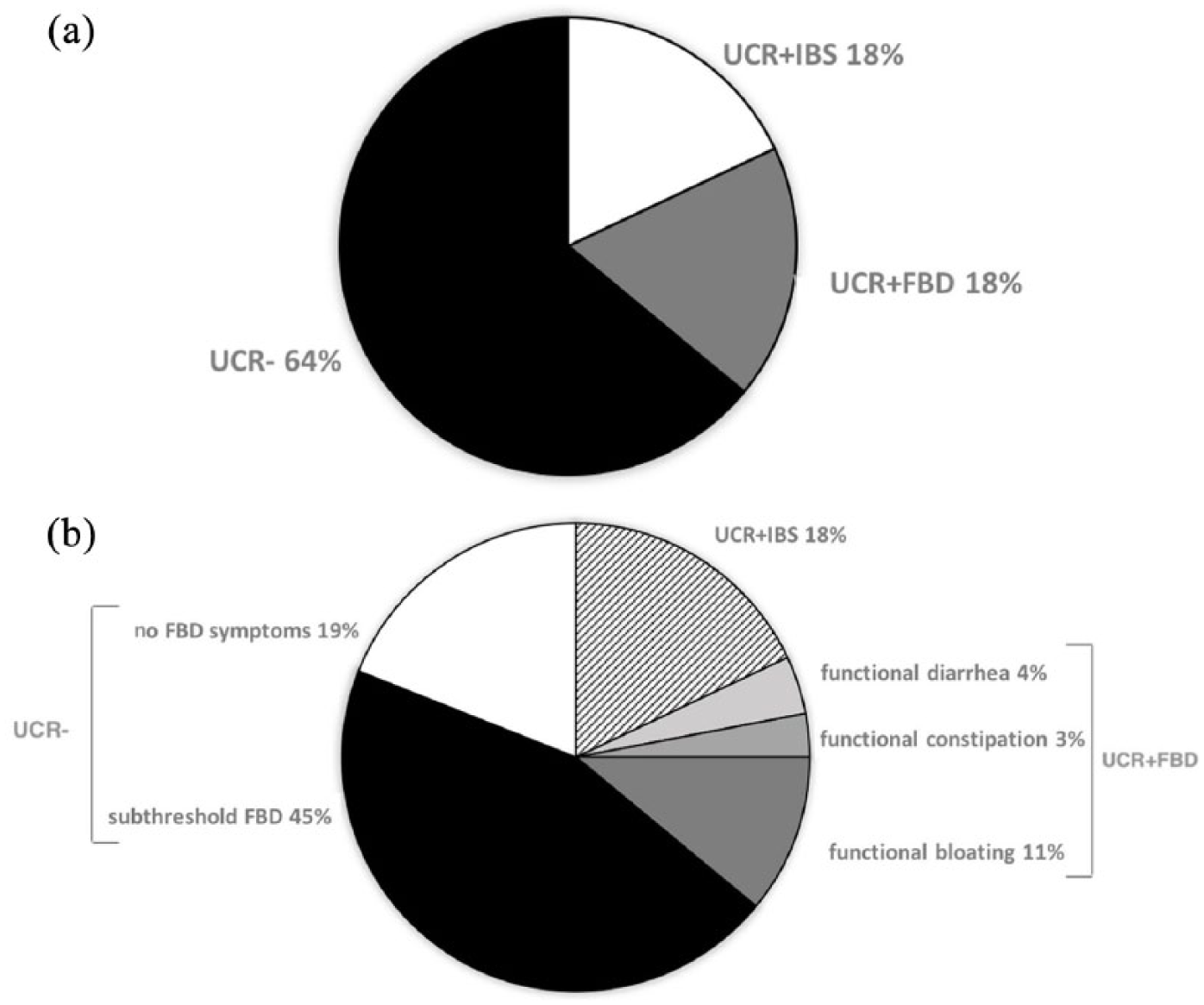
The patient groups and subgroups in UC remission at enrollment.
Demographic data, disease characteristics and current medical treatment at inclusion for UC patients in remission.

Demographic data, disease characteristics and current medical treatment at inclusion for UC patients in remission fulfilling the Rome III criteria for IBS (UCR+IBS), other FBD (UCR+FBD) and without symptoms compatible with IBS or other FBD (UCR-).
Not statistically significant differences were observed when comparing the three groups.
ASA, aminosalicylic acid; FBD, functional bowel disorder; IBS, irritable bowel syndrome; TNF, tumor necrosis factor; UC, ulcerative colitis; UCR, ulcerative colitis in remission.
Symptoms compatible with FBD and other GI and non-GI symptoms and QoL
UCR+FBD patients reported more severe over-all GI symptoms, evaluated by the total GSRS, than UCR- (Table 4). However, no individual GSRS symptom differed between UCR+FBD and UCR- patients, except for indigestion, which was higher for UCR+FBD. The UCR+FBD group reported less severe total GI symptoms compared with UCR+IBS. The burden of non-GI somatic symptoms (PHQ-12) was not higher in the UCR+FBD than the UCR- group, whereas UCR+IBS patients had higher scores than the other two groups (Table 4). The total IBD-Q score was lower in UCR+FBD patients than UCR-, however only the subscore measuring bowel symptoms differed between the groups. UCR+IBS had lower total IBD-Q score and subscores of bowel symptoms and emotional functions than UCR+FBD (Table 5).
Severity of GI (GSRS, total score and five domains) and non-GI somatic symptoms (PHQ-12) in UC patients in remission.
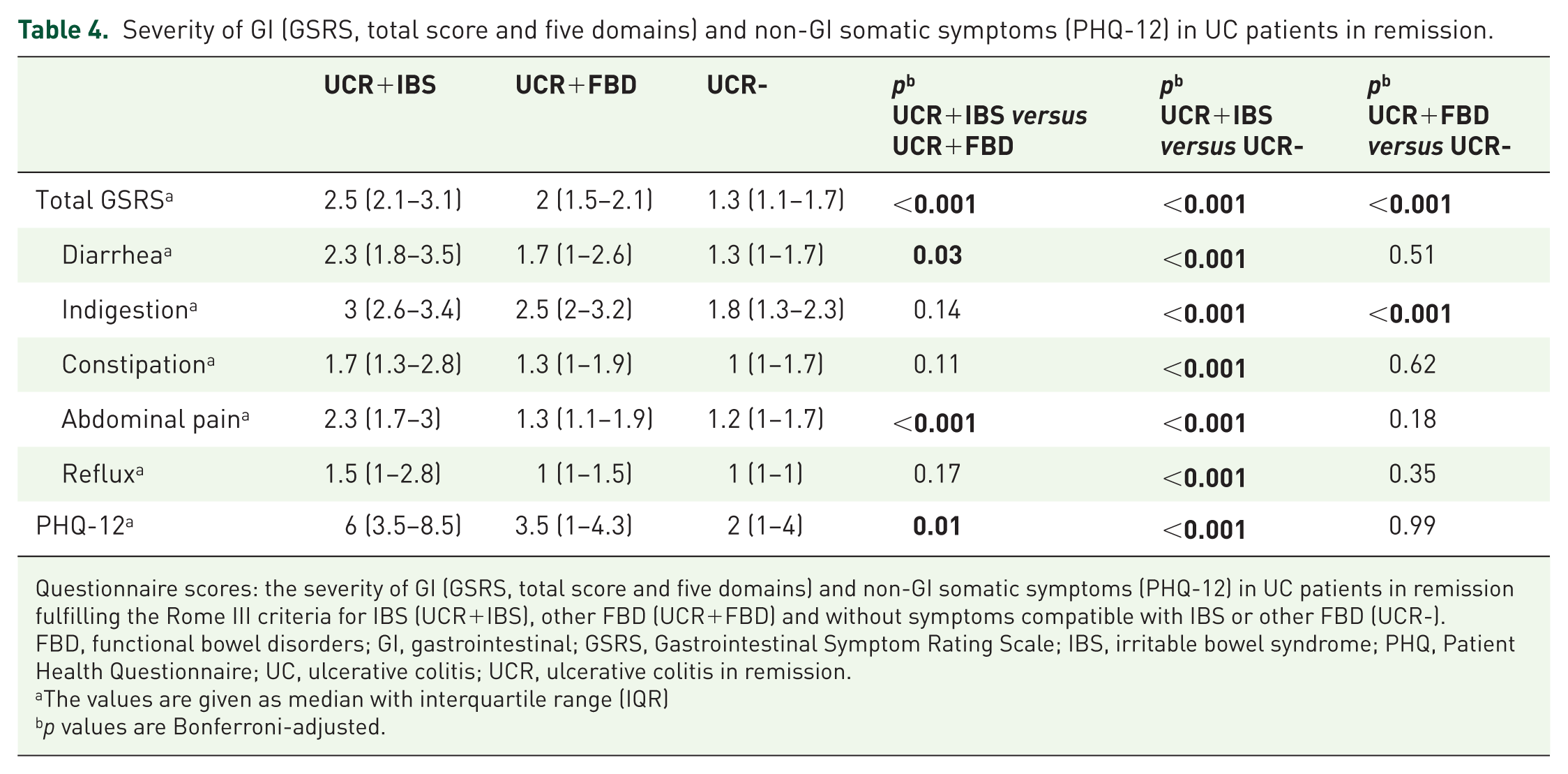
Questionnaire scores: the severity of GI (GSRS, total score and five domains) and non-GI somatic symptoms (PHQ-12) in UC patients in remission fulfilling the Rome III criteria for IBS (UCR+IBS), other FBD (UCR+FBD) and without symptoms compatible with IBS or other FBD (UCR-).
FBD, functional bowel disorders; GI, gastrointestinal; GSRS, Gastrointestinal Symptom Rating Scale; IBS, irritable bowel syndrome; PHQ, Patient Health Questionnaire; UC, ulcerative colitis; UCR, ulcerative colitis in remission.
The values are given as median with interquartile range (IQR)
p values are Bonferroni-adjusted.
Quality of life (IBD-Q, total score and four domains) in UC patients in remission.

Questionnaire scores: quality of life (IBD-Q, total score and four domains) in UC patients in remission fulfilling the Rome III criteria for IBS (UCR+IBS), other FBD (UCR+FBD) and without symptoms compatible with IBS or other FBD (UCR-).
The values are given as median with interquartile range.
p values are Bonferroni adjusted.
FBD, functional bowel disorders; IBD, inflammatory bowel disease; IBD-Q, IBD Questionnaire; IBS, irritable bowel syndrome; UC, ulcerative colitis; UCR, ulcerative colitis in remission.
Factors associated with symptoms compatible with FBD other than IBS
Anxiety/depression scores (HADS) and perceived stress (PSS-14) were similar among UCR+FBD and UCR- patients (Table 6). Also f-cal, hs-CRP and serum cytokines analyses showed no differences between the UCR+FBD and UCR- groups (Supplementary Table 1).
Anxiety and depression (HADS) and perceived stress (PSS-14) in UCR+FBD and UCR- patients.

Questionnaire scores: anxiety and depression (HADS) and perceived stress (PSS-14) in UC patients in remission fulfilling the Rome III criteria for other FBD (UCR+FBD) and without symptoms compatible with IBS or other FBD (UCR-).
The values are given as median with interquartile range (IQR).
FBD, functional bowel disorder; GI, gastrointestinal; HADS, Hospital Anxiety/Depression Scale; IBS, irritable bowel syndrome; PSS-14, Perceived Stress Scale; UC, ulcerative colitis; UCR, ulcerative colitis in remission.
Stability of symptoms compatible with IBS/other FBD and impact on the UC course
A total of 171 patients completed the follow up [58.4% response rate; Figure 1(b)]. Table 7 shows demographics, disease characteristics and treatment at enrollment for patients participating in the follow up and those who were lost to follow up. Patients who did not participate in the follow up were younger and more likely to be on thiopurines and TNF blockers, but otherwise did not differ significantly in other baseline characteristics from the patients who completed the follow-up assessment.
Demographic data, disease characteristics and current medical treatment of the patients who completed the whole study versus patients who completed only the cross-sectional part.
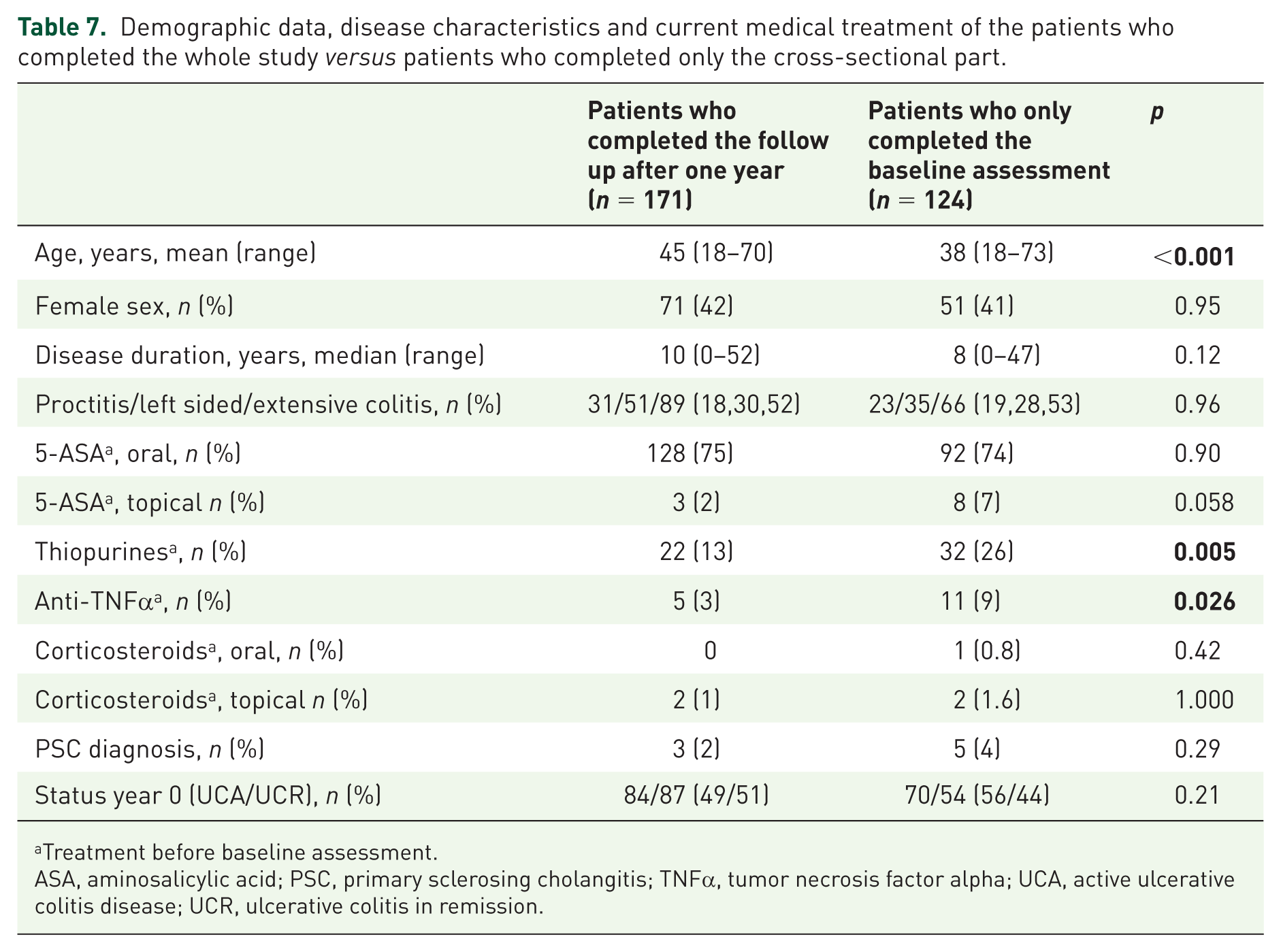
Treatment before baseline assessment.
ASA, aminosalicylic acid; PSC, primary sclerosing cholangitis; TNFα, tumor necrosis factor alpha; UCA, active ulcerative colitis disease; UCR, ulcerative colitis in remission.
Both UC activity and the presence of symptoms compatible with IBS/other FBD in remission fluctuated over time. However, the prevalence of these symptoms at the two timepoints was similar [IBS: 18.2% year 0 versus 18.5% year 1 (p = 0.96), other FBD; 18% year 0 versus 26.1% year 1 (p = 0.16)]. Out of the patients meeting the UCR+FBD criteria at enrollment, 31% still reported symptoms compatible with FBD when in remission at follow up. For cases meeting the UCR+IBS criteria at enrollment, 36% still met IBS criteria when in remission at follow up (Figure 3).

The over-1-year stability of FBD in the cohort of UC patients.
The UCR+IBS/FBD group (n = 29) when compared with the UCR- (n = 52) had similar modified Mayo score [0 (Q1 = 0, Q3 = 1) versus 0 (Q1 = 0, Q3 = 0), p = 0.21], and f-cal [66 (Q1 = 29, Q3 = 247) versus 53 (Q1 = 31, Q3 = 142), p = 0.95] at follow up. Additionally, the number of flares during follow up was similar [0 (Q1 = 0, Q3 = 1) versus 0 (Q1 = 0, Q3 = 0), p = 0.47]. Furthermore, the proportion of patients with active disease at follow up did not differ between the UCR+IBS, UCR+FBD and UCR- groups, as defined at the time of inclusion (Figure 3).
Discussion
We report that 18% of patients with quiescent UC demonstrated symptoms consistent with FBD other than IBS. Taking into consideration the previously reported 18% prevalence of IBS-like symptoms in this cohort, 12 we conclude that 36% of these patients suffer from symptoms compatible with FBD. Moreover, 45% had subthreshold symptoms compatible with FBD. The burden of GI symptoms in patients with symptoms compatible with FBD other than IBS during remission was higher than in patients without FBD symptoms and had negative impact on their QoL. However, patients with IBS-like symptoms reported the most intense GI symptoms and the largest reduction in QoL. Psychological distress was not correlated with symptoms compatible with FBD other than IBS and they were not linked to systemic immune activity or subclinical colonic inflammation. Finally, symptoms compatible with FBD, including IBS during remission, were not a risk factor for clinical UC relapse during follow up.
To the best of the authors’ knowledge, this is the first study characterizing the prevalence of symptoms compatible with FBD other than IBS using both inflammatory markers and endoscopy to define remission. Among published studies defining FBD with Rome III criteria, Bryant and colleagues 27 reported a 34.4% prevalence for FBD, including IBS, in inactive IBD. This finding is confirmed by our study.
UCR+FBD patients, as compared with UCR-, had more severe GI symptoms overall, whereas non-GI symptoms were similar. However, UCR+IBS patients had the most intense GI and non-GI symptomatology. This suggests that the well-described association of bowel symptoms with non-GI conditions in IBS, 28 is weaker for symptoms compatible with other FBD. In addition, the overall QoL of UCR+FBD patients was impaired when compared with UCR-. However, the only IBD-Q subscore where UCR+FBD patients scored lower was for bowel symptoms. This indicates that it is primarily the increased total burden of GI symptoms that has a negative impact on their QoL.
Interestingly, UCR+FBD patients did not differ from UCR- in terms of psychological comorbidities. Bryant and colleagues 27 showed an association between FGID in IBD and higher anxiety/depression rates, which may be explained by the fact that all FGID diagnoses, including IBS, were evaluated in their study. Likewise, in our cohort, UCR+IBS patients had higher psychological distress than UCR-. Thus, psychological distress, which is proposed as exacerbating pain experience and other GI symptoms in the case of IBS-like symptoms in IBD, 29 may not contribute to the same degree to the generation of symptoms compatible with other FBD. Local factors in the gut, not measured in this study, for example, intestinal immune response, may be important. This notion is also supported by the finding that no elevated markers of systemic immune activity were observed in UCR+FBD patients in contrast to UCR+IBS. 12
Whether functional GI symptoms in inactive UC reflect low-grade UC activity is under debate.7,8,30 We found no evidence for colonic inflammation in UCR+IBS 12 or UCR+FBD patients measured by f-cal and these patients did not have a higher risk of UC flare. We should, however, acknowledge that subtle inflammation may not be detected by traditionally used markers like f-cal, especially if unrelated to neutrophil/macrophage activation.
With regard to the progress of symptoms compatible with FBD over time, it is noteworthy that roughly a third of these patients were still in remission and reported symptoms of the same type at the follow up. This implies that only a proportion of patients are vulnerable to symptoms compatible with FBD in remission. Risk factors to identify this group at the UC diagnosis time remain to be determined. In addition, it emphasizes the importance of investigating the origin of the symptoms in UC patients to decide on the most effective personalized therapeutic regimens, that is, escalation of anti-inflammatory, or treating FBD-like, symptoms.
A strength of this study is the large patient number and that we defined remission by using objective markers like endoscopy and f-cal. We also present evidence on symptoms compatible with FBD in quiescent UC over time. There are some limitations too. It is possible that we overestimated the prevalence of FBD because patients without any clinical visits during the recruitment period were not included in the study, and it seems reasonable to assume that most symptom-free patients do not seek healthcare relative to patients with ongoing symptoms. Moreover, a 1-year follow-up period may be too short when evaluating the development of symptoms compatible with FBD over time and we may also have failed to capture disease activity in the intervening time between the enrollment and follow up. Finally, the response rate at follow up was rather low (58.4%) and we did not use endoscopy but only PROs and f-cal to define UC remission at follow up.
Conclusion
To conclude, symptoms compatible with FBD other than IBS are as common as IBS-like symptoms in UC remission. Special attention should be paid to their recognition, as the GI symptom burden influences patients’ QoL negatively. FBD-like symptoms might also be difficult to distinguish from symptoms related to UC activity leading to unnecessary escalation of anti-inflammatory treatment. However, ongoing low-grade inflammation does not seem to be the cause of them and they do not seem to influence the UC disease course.
Supplemental Material
Supplementary_Material – Supplemental material for Symptoms compatible with functional bowel disorders are common in patients with quiescent ulcerative colitis and influence the quality of life but not the course of the disease
Supplemental material, Supplementary_Material for Symptoms compatible with functional bowel disorders are common in patients with quiescent ulcerative colitis and influence the quality of life but not the course of the disease by Georgios Mavroudis, Magnus Simren, Börje Jonefjäll, Lena Öhman and Hans Strid in Therapeutic Advances in Gastroenterology
Footnotes
Acknowledgements
We would like to thank Dr Antal Bajor, Dr Per Hedenström, Dr Björn Lindkvist (Sahlgrenska University Hospital, Gothenburg), Dr Anders Lasson (Södra Älvsborg Hospital, Borås) and Dr Dietrich Ahlhausen, Dr Eszter Benyei (Norra Älvsborg Hospital, Trollhättan) for participating in patient recruitment, as well as Maria Sapnara and Stefan Isaksson, Department of Microbiology and Immunology, University of Gothenburg, for conducting the immunological analyses.
Funding
This work was supported by the Swedish Medical Research Council (grants 13409, 21691 and 21692), the Health & Medical Care Committee of the Regional Executive Board Region in Västra Götaland (119011), the Göteborg Medical Society and Foundation of Elin and Carl Linder (GLS-406621), the Swedish Society of Medicine (SLS-329111), and the Faculty of Medicine, University of Gothenburg.
Conflict of interest statement
GM has served as a consultant/advisory board member for Abbvie, Tillotts and Pfizer, and as a speaker for Ferring Pharmaceuticals and Takeda. MS received unrestricted research grants from Danone and Ferring Pharmaceuticals and served as a consultant/advisory board member for AstraZeneca, Danone, Nestle, Almirall, Allergan, Albireo, Glycom and Shire, and as a speaker for Tillotts, Menarini, Takeda, Shire, Allergan and Almirall. BJ has served as consultant/advisory board member and speaker for MSD, Abbvie, Tillotts, MEDA and Takeda. LÖ received unrestricted research grants from AstraZeneca and served as consultant/advisory board member for Genetic Analysis, and as a speaker for Takeda and Abbvie. HS has served as a consultant/advisory board member for Takeda, Abbvie, Ferring Pharmaceuticals, Tillotts, Pfizer, Janssen and MSD, and as a speaker for Takeda, Abbvie, Ferring Pharmaceuticals, Tillotts, MSD and Shire.
Supplemental material
Supplemental material for this article is available online.
References
Supplementary Material
Please find the following supplemental material available below.
For Open Access articles published under a Creative Commons License, all supplemental material carries the same license as the article it is associated with.
For non-Open Access articles published, all supplemental material carries a non-exclusive license, and permission requests for re-use of supplemental material or any part of supplemental material shall be sent directly to the copyright owner as specified in the copyright notice associated with the article.