
Abstract
Perihilar cholangiocarcinoma (PHCC) is an aggressive biliary malignancy originating from the epithelial cells of the bile duct, typically located in the extrahepatic biliary tree, proximal to the cystic duct. PHCC often presents with a rapid onset of jaundice. While radical surgical resection remains the only curative treatment, only a minority of patients are eligible due to early metastasis and challenges associated with preoperative evaluations. Comprehensive treatments, including chemotherapy, radiotherapy, targeted therapy, and immunotherapy, are crucial for managing PHCC. However, in advanced stages, complications such as cholestatic liver injury, malnutrition, and biliary infections pose significant obstacles to these treatments. Therefore, biliary drainage (BD) is essential in the management of PHCC. In addition to external drainage methods like percutaneous transhepatic biliary drainage (PTBD), endoscopic biliary drainage (EBD), particularly endoscopic retrograde cholangiopancreatography (ERCP), offer an effective option for internal drainage, which is more physiologically compatible and better tolerated. Furthermore, the integration of various endoscopic techniques has expanded the management of PHCC beyond mere drainage. Techniques such as radiofrequency ablation (RFA), photodynamic therapy (PDT), and endoscopic ultrasound (EUS) based methods present new therapeutic avenues, albeit with variable results. This review aims to summarize current advancements and ongoing debates in the field of endoscopic treatment for unresectable PHCC.

Introduction
Perihilar cholangiocarcinoma (PHCC), also known as Klatskin tumor, refers to cholangiocarcinoma located between the second-order bile ducts and the junction of the cystic duct. It represents the most prevalent form of cholangiocarcinoma, accounting for 40%–60% of all cases. 1 Common classification systems for PHCC include Bismuth-Corlette, AJCC, Blumgart T-staging, and Memorial Sloan-Kettering Cancer Center (MSKCC) T-staging systems. The Bismuth-Corlette classification emphasizes the tumor’s location and extent along the bile duct system. It is primarily used for preliminary endoscopic diagnosis, staging, and guiding surgical planning, and is widely applied to direct localized treatment during endoscopy. However, it lacks information on vascular invasion, metastasis, and liver lobe atrophy, which limits its predictive capability concerning resectability and prognosis2,3 (Figure 1). The Blumgart T-staging system classifies tumors based on the extent of invasion, portal vein involvement, and ipsilateral liver lobe atrophy, providing better predictive validity for resectability and the likelihood of achieving R0 resection. Nonetheless, it does not consider lymph nodes or distant metastases, which limits its prognostic value.4,5 In 2001, the MSKCC proposed a T-staging system that integrates local tumor factors, including portal vein involvement and liver lobe atrophy, demonstrating good predictive value for resectability. 6 The AJCC staging system is based on pathological findings, including vascular invasion, lymph node involvement, and distant metastases, providing improved prognostic value and guidance for postoperative treatment.7–9

The Bismuth-Corlette classification of PHCC.
The incidence of PHCC varies considerably worldwide, with a notably higher incidence in Asia, ranging from 1 to 70 per 100,000 population, and showing an increasing trend over the years. 10 Surgical resection remains the only curative treatment. However, due to the partial patency of the common bile duct in the early stage, many patients are asymptomatic or present with nonspecific symptoms. Once complete biliary obstruction occurs, patients typically exhibit symptoms such as jaundice (80%–90%), abdominal pain, dark urine, pale stools, pruritus, and often fever. Unfortunately, these symptoms usually indicate disease progression, resulting in missed surgical opportunities. Consequently, only 20%–30% of PHCC patients are candidates for R0 resection, with a median survival of 1–4 years. By contrast, only 5–9 months for those unresectable ones.10,11 Therefore, adequate biliary drainage (BD) combined with systemic treatments can significantly improve survival outcomes.
BD by endoscopic techniques
The importance and significance of BD in unresectable PHCC
In advanced PHCC, patients frequently succumb not to widespread metastasis but rather to severe cholangitis and liver failure due to biliary obstruction. Although comprehensive treatments can prolong overall survival, 12 they typically require total bilirubin levels to be maintained below 50 μmol/L for effective administration. 13 Therefore, BD serves not only as a palliation treatment but also as a prerequisite for other therapies. Unlike malignant distal biliary obstruction (MDBO), PHCC often leads to the isolation of segmental bile ducts, which complicates BD and increases the likelihood of reintervention. Thus, developing rational strategies, selecting appropriate drainage methods, and advancing new endoscopic treatments are critical areas of research.
Currently, there exists a guideline and a consensus on endoscopic treatment for hilar biliary obstruction,14,15 alongside several other guidelines and consensuses that address biliary obstruction or strictures, incorporating aspects of hilar obstruction treatments.16–19 While these guidelines universally emphasize the necessity of BD; however, they vary in their recommendations related to the types, numbers, and selection strategies for stenting in the context of PHCC. These considerations hinge not only on the critical Bismuth classification but also on the available facilities, the expertise of the center, and the individual patient’s conditions (e.g., the presence of infection or the need for subsequent treatments).
The methods for BD—EBD or PTBD?
BD can be categorized into internal and external drainage. Internal drainage includes endoscopic biliary stenting (EBS) and internal percutaneous transhepatic biliary drainage (iPTBD), while external drainage encompasses endoscopic nasobiliary drainage (ENBD) and external PTBD (ePTBD). Similar to the treatment of MDBO, internal drainage has the advantage of reconstructing the enterohepatic circulation of bile acids, which is more physiologically compatible and improves nutritional status. 20 However, high-level biliary obstructions present unique challenges, such as segment bile duct isolation and intrahepatic metastases, complicating the percutaneous BD.
The selection of appropriate drainage methods should consider factors such as the Bismuth classification, bile duct anatomy, and the overall condition of the patient, including any concurrent infections or the need for future treatments. For Bismuth type I and II PHCC, the preferred approach is the placement of an internal drainage stent via ERCP, the presence of biliary infections may necessitate a direct choice of PTBD or ENBD for external drainage. Thus, simultaneous placement of both a metal stent and ENBD may also be considered to achieve both internal and external drainage. For Bismuth type III and IV PHCC, the primary objective is to drain as many liver segments as possible. While existing guidelines do not provide definitive conclusions on this matter, there remains an ongoing debate regarding the optimal approach (Figure 2).

Graphical explanation of ERCP, PTBD, EUS-HGS, and EUS-HDS.
Technical and clinical success of EBD and PTBD
Technical success refers to the successful placement of a catheter or tube within the bile duct. However, due to complex obstructions and factors such as intrahepatic metastasis, drainage tubes may fail to provide adequate drainage and may exacerbate liver function by triggering biliary infections. Thus, technical success does not translate into clinical success. Clinical success is characterized by the regression of jaundice, restoration of liver function, and improvement in nutritional status.21–24
In EBD therapy, challenges in treating MDBO differ from those encountered in PHCC. In cases of MDBO, partial tumor invasion of the papilla often alters its morphology and position, commonly resulting in a dilated common bile duct. By contrast, with PHCC obstruction, the papillary structure typically remains intact, but prolonged disuse of the common bile duct complicates cannulation. PTBD is relatively easier in MDBO since catheter placement in any area above the obstruction can yield effective drainage. If PTBD proves difficult, percutaneous transhepatic gallbladder drainage can often yield satisfactory results and is comparatively simpler to perform. However, this becomes considerably more complex in PHCC.
Few studies have reported technical success rates for PTBD and EBD, possibly because technical challenges have not been the primary focus of research. Most published studies indicated no significant difference in clinical success rates between EBD and PTBD.13,24–26 Still, some single-center retrospective studies indicated a higher rate of clinical success for PTBD. Walter et al. 27 ’s study reported a higher clinical success rate in the PTBD group compared to the EBD group (79% vs 49%, p = 0.002), with 51% of EBD patients who failed subsequently undergoing conversion to the PTBD. Paik et al. 23 ’s study, which included unresectable Bismuth types III–IV PHCC patients, compared EBS and ePTBD with self-expanding metal stent (SEMS) implantation, finding that the clinical success rate was significantly higher in the ePTBD group than that in the EBS group (92.7% vs 77.3%, p = 0.049). Lee et al. 28 ’s study demonstrated that compared to the EBD group (79.4%), both the ePTBD group (93.9%) and iPTBD group (97.1%) had higher initial success rates (p = 0.03). However, other studies generally supported the absence of significant differences in clinical success rates between the PTBD and EBS groups (Table 1).
Comparison of the clinical success rates of EBD and PTBD.
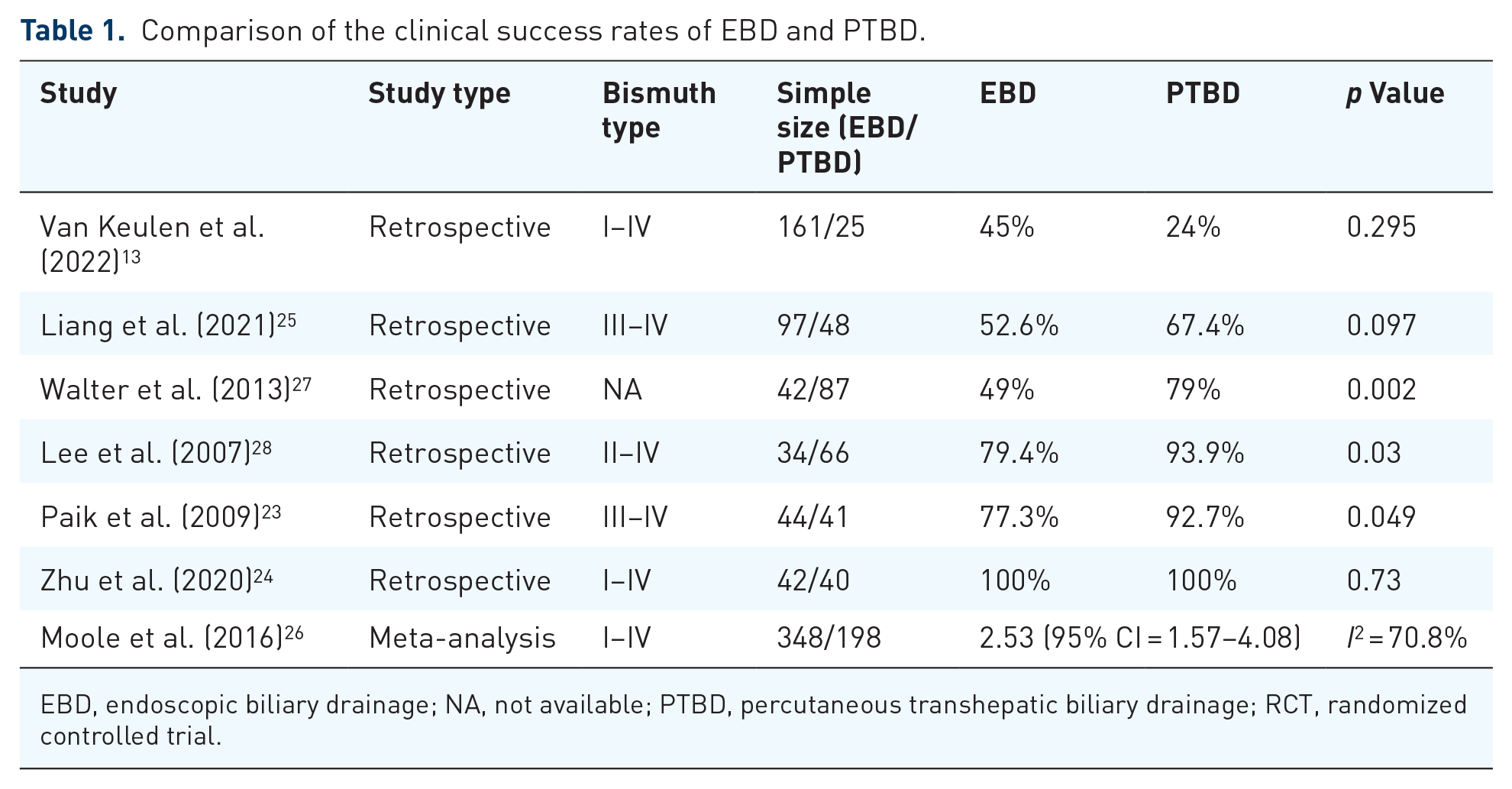
EBD, endoscopic biliary drainage; NA, not available; PTBD, percutaneous transhepatic biliary drainage; RCT, randomized controlled trial.
The observed differences may be attributed to various factors, including the type and number of stents, as well as the Bismuth type of patients in each study. In addition, PTBD includes both ePTBD and iPTBD, which may represent significant confounding factors affecting the final outcomes.
Overall survival and patency time of PTBD and EBD
Theoretically, stent implantation does not alter the natural course of PHCC, and bile duct drainage should not affect survival time. However, the effectiveness of bile duct drainage is not only closely related to liver function, nutritional status, and immune system improvement, ultimately facilitating comprehensive treatments that correlate with quality of life and survival time.23,29,30
Existing studies consistently demonstrate no significant difference in overall survival between patients undergoing EBD and those undergoing PTBD (Table 2). Rather, the success of initial drainage and subsequent treatment plays a critical role in determining patient survival. Born et al. 31 ’s study indicated that among patients with successful primary drainage, the median survival was 7.5 months, whereas none of the patients with unsuccessful initial drainage survived beyond 6 months. Patients selected for adjuvant radiotherapy, chemotherapy, or both exhibited a median survival of 9 months (range 3–38 months). Liang et al. 25 ’s research revealed a survival advantage associated with successful drainage (227 vs 82 days, p < 0.001). In addition, Paik et al. 23 found that the median survival of patients with initially successful BD, regardless of procedure type, was significantly longer than that of those with failed drainage (8.7 vs 1.8 months, p < 0.001), and this was the factor most associated with long-term survival by univariate and multivariate analyses (p < 0.001). Once successful BD was achieved, median survival and stent patency duration were comparable between the two approaches.
Comparison of the overall survival and patency time of EBD and PTBD.
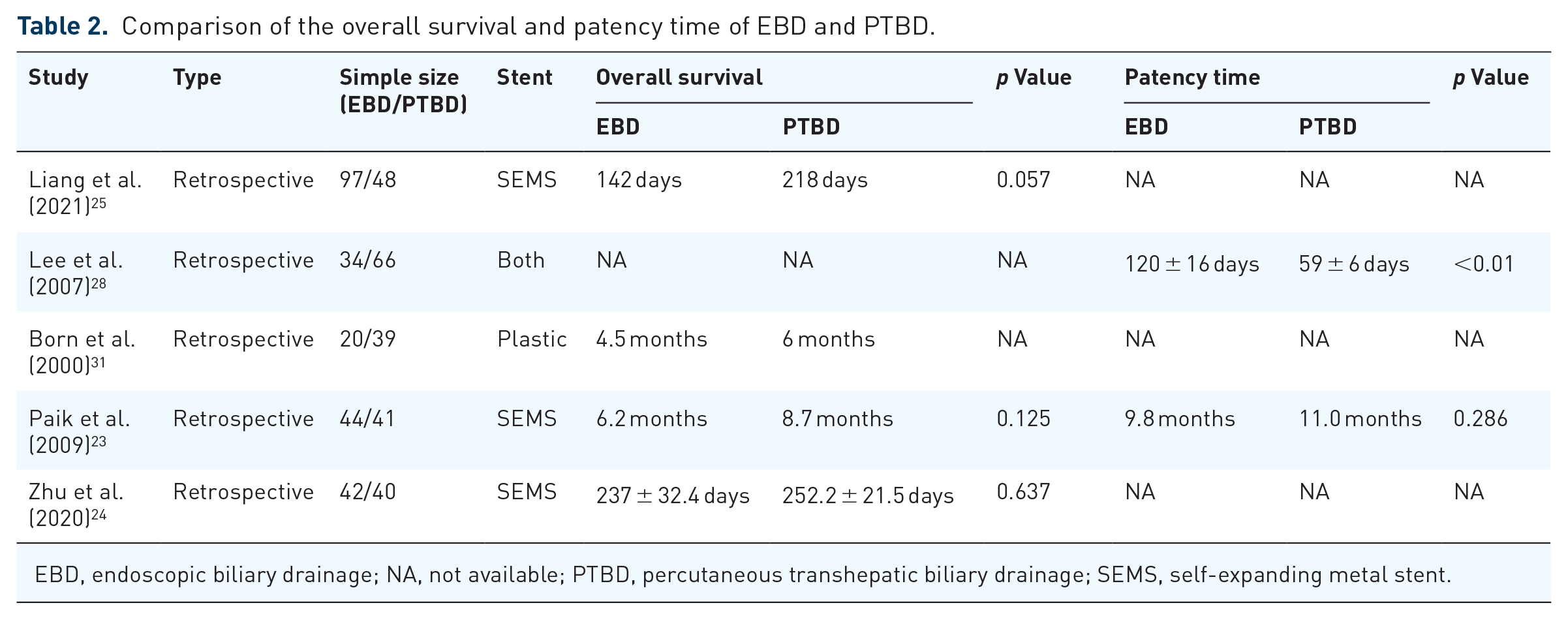
EBD, endoscopic biliary drainage; NA, not available; PTBD, percutaneous transhepatic biliary drainage; SEMS, self-expanding metal stent.
Regarding patency duration, only Lee et al. 28 ’s study reported statistically different results, in Bismuth type III PHCC, EBD and iPTBD exhibited superior patency rates compared to ePTBD (188 ± 47, 133 ± 21, and 53 ± days, respectively, p < 0.01). Cox regression analysis revealed a significant association between the type of drainage procedure and duration of patency (EBD: p = 0.01; iPTBD: p < 0.01). For patients with Bismuth type IV, the mean patency duration for iPTBD, EBD, and ePTBD were 251 ± 36, 102 ± 19, and 60 ± days, respectively (p < 0.01). However, there was no difference for Bismuth type II PHCC (Table 2).
The differences in outcomes may be attributed to factors beyond the drainage technique, as stent patency is influenced not only by the type of drainage method but also by stent characteristics, the number of stents used, and the stent placement strategy (which will be discussed later). Therefore, more rigorous clinical studies are warranted.
Postoperative complications of PTBD and EBD
Regarding postoperative complications, no significant differences were observed between the EBD and PTBD groups (Table 3). Among all complications, pancreatitis and cholangitis are the most extensively studied. Research findings diverge significantly from theoretical expectations. While none of the studies reported a statistically significant difference in the incidence of pancreatitis between the two groups, it is noteworthy that the PTBD group did not have a zero incidence, two studies indicated a higher incidence of pancreatitis in the PTBD group.23,27 Similar observations have been made concerning postoperative cholangitis. Theoretically, external drainage should reduce the incidence of postoperative cholangitis; however, apart from Zhu et al. 24 ’s study, which showed a significantly lower incidence of cholangitis in the PTBD group, other studies did not find significant differences between the two groups.
Comparison of the complications of EBD and PTBD.

EBD, endoscopic biliary drainage; NA, not available; PTBD, percutaneous transhepatic biliary drainage.
These results may be influenced by various factors. First, most studies did not differentiate between iPTBD and ePTBD. Second, the types and numbers of stents utilized in EBD procedures varied. In addition, factors such as sample size and biases inherent in retrospective studies may also affect the results. Furthermore, some studies have combined PTBD with internal drainage via percutaneous biliary stenting.13,24 This approach leverages the strengths of both approaches while mitigating their weaknesses. Liu et al. 32 reported that combining ENBD and EBS reduces cholangitis rates and improves liver chemistries. Similarly, in our center, we often employ a simultaneous approach using plastic stenting and ENBD tube for Bismuth II/III/IV PHCC to evaluate the effect of BD and liver function recovery. If the drainage effect is satisfactory, the ENBD can be severed for stent transformation via an endoscopic scissor. This two-step technique not only allows for ex vivo assessment but also enhances patient tolerance and psychological outcomes. Our experience indicates that maintaining an ENBD tube can significantly reduce postoperative infections and facilitate ongoing monitoring of bile duct patency through cholangiography.
In summary, there currently exists insufficient evidence to definitively determine where PTBD or EBD has a relative advantage. Only one guideline recommends using ERCP for Bismuth type I and II obstructions while suggesting PTBD or a combination of PTBD and ERCP for type III and IV. 16 Other guidelines and some studies advocate for PTBD due to its similar clinical success and patency duration as compared to EBD, though concerns about the higher incidence of cholangitis and technical challenges associated with EBD exist.14,33,34 Conversely, other researches highlight the potential drawbacks of PTBD, such as its association with peritoneal metastasis,35,36 as well as the discomfort and psychological distress it may impose on patients, subsequently increasing the nursing burden. Therefore, the choice between PTBD and EBD should be guided by the experience of local centers, patient preferences, and the specific clinical context.
The selection of stents in EBD
The selection of stents is closely tied to advancements in material science, particularly regarding their patency. In managing unresectable PHCC, the focus shifts from operative area adhesions and edema—critical factors in resectable cases—to the efficacy of drainage procedures. Currently, plastic stents and SEMS are widely employed in the EBD approach. Plastic stents offer various length options and can be trimmed using an ENBD tube to suit clinical needs. By contrast, while SEMS exhibit superior drainage efficiency due to their larger inner diameters, their placement in narrow anatomical spaces poses significant challenges. However, existing researches indicate that the technical success rate in the SEMS group is not lower than that in the plastic stent group, and in some studies, it even surpasses.37,38 Clinical success rates are predictably higher in the SEMS group, although some studies show no statistically significant differences, a trend favoring metallic stents persists (Table 4).
Comparison of the technical success and clinical success rates of plastic and metallic stents.

NA, not available; RCT, randomized controlled trial.
A body of research (Tables 4 and 5) has demonstrated that SEMS yield better outcomes regarding stent dysfunction, re-intervention rates, and median survival times. For example, Sawas et al. 47 confirmed that SEMS had a lower 30-day occlusion rate compared to plastic stents (odds ratio (OR) 0.16; 95% confidence interval (CI): 0.04–0.62), and a lower long-term occlusion rate in the context of hilar malignant obstruction (OR 0.28; 95% CI: 0.19–0.39). Therapeutic failure was more likely with plastic stents (13%) than with SEMS (7%; OR 0.43; 95% CI: 0.27–0.67). Furthermore, SEMS required fewer reinterventions compared to plastic stents (mean difference, 0.49; 95% CI: 0.8–0.19), and the incidence of cholangitis was statistically lower with SEMS (8% vs 21%; OR 0.41; 95% CI: 0.22–0.76). A randomized controlled trial (RCT) conducted by Sangchan demonstrated a higher successful drainage rate in the SEMS group compared to the plastic stent group (70.4% vs 46.3%, p = 0.011), with a median survival time of 126 days in the SEMS group versus 49 days in the plastic stent group (p = 0.002). 38
Comparison of survival time, stent patency, and reintervention of plastic and metallic stents.
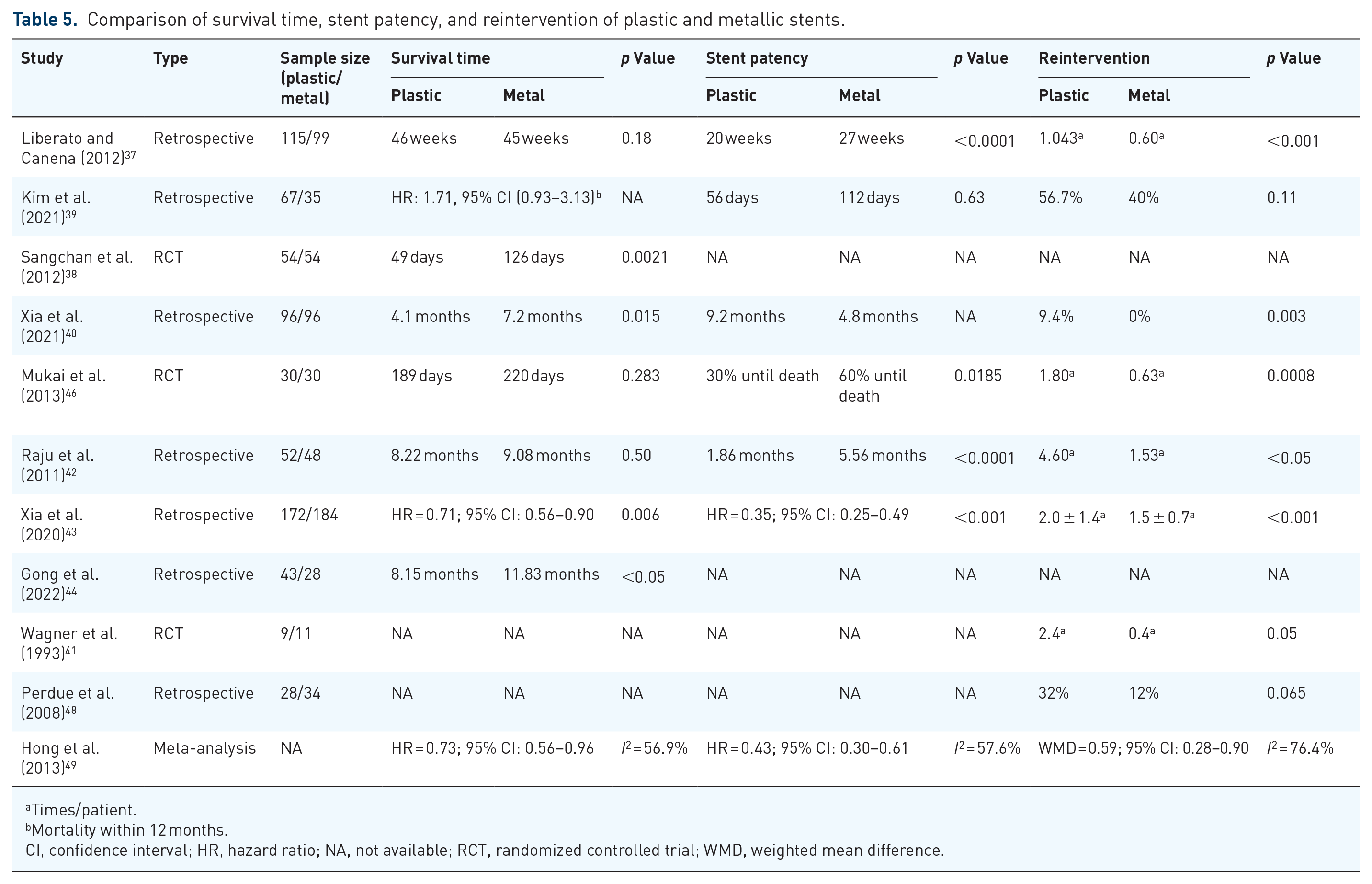
Times/patient.
Mortality within 12 months.
CI, confidence interval; HR, hazard ratio; NA, not available; RCT, randomized controlled trial; WMD, weighted mean difference.
Several guidelines recommended SEMS as the preferred choice for endoscopic palliation.15,16 However, some literature suggested that advancements in chemotherapy, immunotherapy, and targeted therapy may allow the survival of unresectable PHCC patients to exceed the patency duration of SEMS.50,51 This raises concerns regarding the challenges of endoscopic re-intervention for SEMS, potentially increasing the need for PTBD. And some guidelines suggest that plastic stents might be more appropriate for patients responding to adjuvant therapy. 14 Nevertheless, we disagree with this viewpoint, as reinserting plastic stents or fully covered SEMS into patients is feasible in our center. Due to the increased use of peroral cholangioscopy (POCS) and endoscopic ultrasound (EUS), the difficulties of re-intervention have substantially decreased. Notably, as locoregional therapies continue to evolve, including radiofrequency ablation (RFA) and photodynamic therapy (PDT), which will be discussed in detail subsequently, plastic stents emerge as a commendable alternative. However, when it comes to EUS treatments (as discussed later), metallic stents are primarily preferred.
The strategy of BD in unresectable PHCC
As previously discussed, BD in unresectable PHCC presents significant challenges due to the isolation of segmental bile ducts and the tumor’s location. Consequently, a single stent may not provide sufficient or durable drainage. A well-thought-out strategy is therefore essential.
Debate continues over the benefits of unilateral versus bilateral drainage in managing PHCC. Some studies and one guideline 15 suggest that bilateral drainage may offer advantages over unilateral drainage. Specifically, Lee et al. 52 ’s multicenter, prospective, randomized study revealed the bilateral group had a significantly longer patency duration (252 vs 139 days, p < 0.01), higher clinical success rates (95.3% vs 84.9%, p = 0.047), and lower re-intervention rates (42.6% vs 60.3%, p = 0.049) compared to the unilateral group. Xia et al. 43 demonstrated that bilateral stent placement resulted in higher clinical success rates (p = 0.024), increased stent patency (p = 0.018), and improved overall survival (p = 0.040) compared to unilateral stenting. Although this study included some non-PHCC patients. Another retrospective study by Liberato and Canena 37 found that the cumulative patency of bilateral SEMS or plastic stents was significantly superior to that of unilateral deployment (p < 0.01) and was the only independent prognostic factor associated with stent patency. In addition, the primary re-intervention rate in the bilateral group was lower than that in the unilateral group (42.6% vs 60.3%, p = 0.049).
Conversely, a substantial body of research, including three meta-analyses,53–55 suggests that unilateral drainage is not inferior to bilateral drainage in terms of clinical efficacy and safety, with no significant differences in survival rates between the two groups. An RCT by De Palma et al. 56 argued against the routine insertion of multiple stents, as the success rates for drainage, median survival, complication rates, and mortality did not differ significantly between the two groups. Another RCT conducted by Hakuta et al. 57 found no differences in transient re-obstruction rates and overall survival between the two groups (p = 0.11 and p = 0.78, respectively), and the bilateral SEMS groups experienced a higher incidence of early adverse events (5.3% vs 28%; p = 0.11). A recent meta-analysis led by Wang et al. 53 indicated no significant differences in the technical success rates (OR = 0.93; 95% CI: 0.34–2.54, p = 0.88), clinical success rates (OR = 1.03; 95% CI: 0.49–2.15, p = 0.94), stent dysfunction (OR = 1.47; 95% CI: 0.91–2.39, p = 0.12), or survival rates (hazard ratio (HR) = 0.85; 95% CI: 0.50–1.42, p = 0.53) between the groups. The complication rate was notably lower in the unilateral group (OR = 0.34; 95% CI: 0.13–0.88, p = 0.03; Table 6).
Comparison of the overall survival and patency time patency of unilateral and bilateral.

Bil, bilateral; CI, confidence interval; HR, hazard ratio; NA, not available; OR, odds ratio; RCT, randomized controlled trial; SEMS, self-expanding metal stent; Uni, unilateral.
The discrepancies among these studies can be attributed to variations in disease types, stages, Bismuth classification, liver volume, the types of stents, and the expertise in each center. Current guidelines do not offer specific recommendations regarding unilateral versus bilateral stenting for unresectable PHCC. Nonetheless, they highlight the necessity of adopting a departmental drainage strategy paradigm in clinical practice and future research. And the latest perspectives suggest that the goal of drainage should be to achieve at least 50% liver volume drainage, without overemphasizing the choice between unilateral or bilateral approaches.14,16–18 Vienne et al. 69 reported in 2010 that drainage of at least 50% liver volume yields better outcomes, longer survival, and fewer instances of cholangitis compared to drainage of less than 50%. Furthermore, a retrospective study by Caillol et al. 70 in 2019 highlighted the advantages of higher liver drainage ratios, showing that maximal drainage greater than 80% was associated with longer survival compared to drainage of less than 80% (HR = 2.46; 95% CI: 1.16–5.23, p = 0.02).
In addition to bilateral drainage, the optimal between stent-in-stent and side-by-side remains unclear. Published studies are limited, resulting in low evidence quality. An RCT performed by Lee et al. 71 revealed no significant differences between these two approaches regarding clinical success, complications, stent dysfunction, or overall survival. And two other meta-analyses reached the same conclusion.72,73 It is noteworthy that some studies have explored the use of smaller metallic stents (6 mm) for multisite drainage like plastic stents.74,75
Regarding suprapapillary and transpapillary approaches, Borges et al.’s 76 study found that while technical success, occlusion rates, reintervention rates, adverse events, and 30-day mortality were similar between the two techniques, the 90-day mortality and postoperative infection indicators were higher in the transpapillary group. Based on our center’s experience, transpapillary procedures are relatively straightforward, with convenient stent retrieval; however, this approach increases the risk of reflux. By contrast, suprapapillary stenting carries a higher risk of stent migration.
In conclusion, developing a comprehensive drainage strategy is more critical than merely selecting the materials or quantity of the drainage tubes itself.
The role of EUS techniques in PHCC
First, EUS can also be utilized as a diagnostic tool for PHCC. Although ERCP brush cytology is the standard method for diagnosing malignant biliary strictures, it has a relatively low sensitivity. In cases of negative ERCP brush cytology, EUS-guided fine-needle aspiration biopsy can achieve higher sensitivity and specificity77,78 and has gradually become a first-line diagnostic method for hilar strictures. 79 And with advancements in artificial intelligence (AI) and image analysis systems, the integration of AI into EUS significantly simplifies for endoscopists. 80
In addition to BD, EUS-BD has emerged as a viable alternative, particularly in patients who have failed ERCP or surgically altered anatomy.81–84 EUS-BD may even outperform PTBD in certain scenarios,17,85,86 and one study indicates that patients show a preference for EUS-BD over PTBD 87 (Figure 2), (Table 7).
Success rates, complications, patency time, and survival time of EUS-BD.
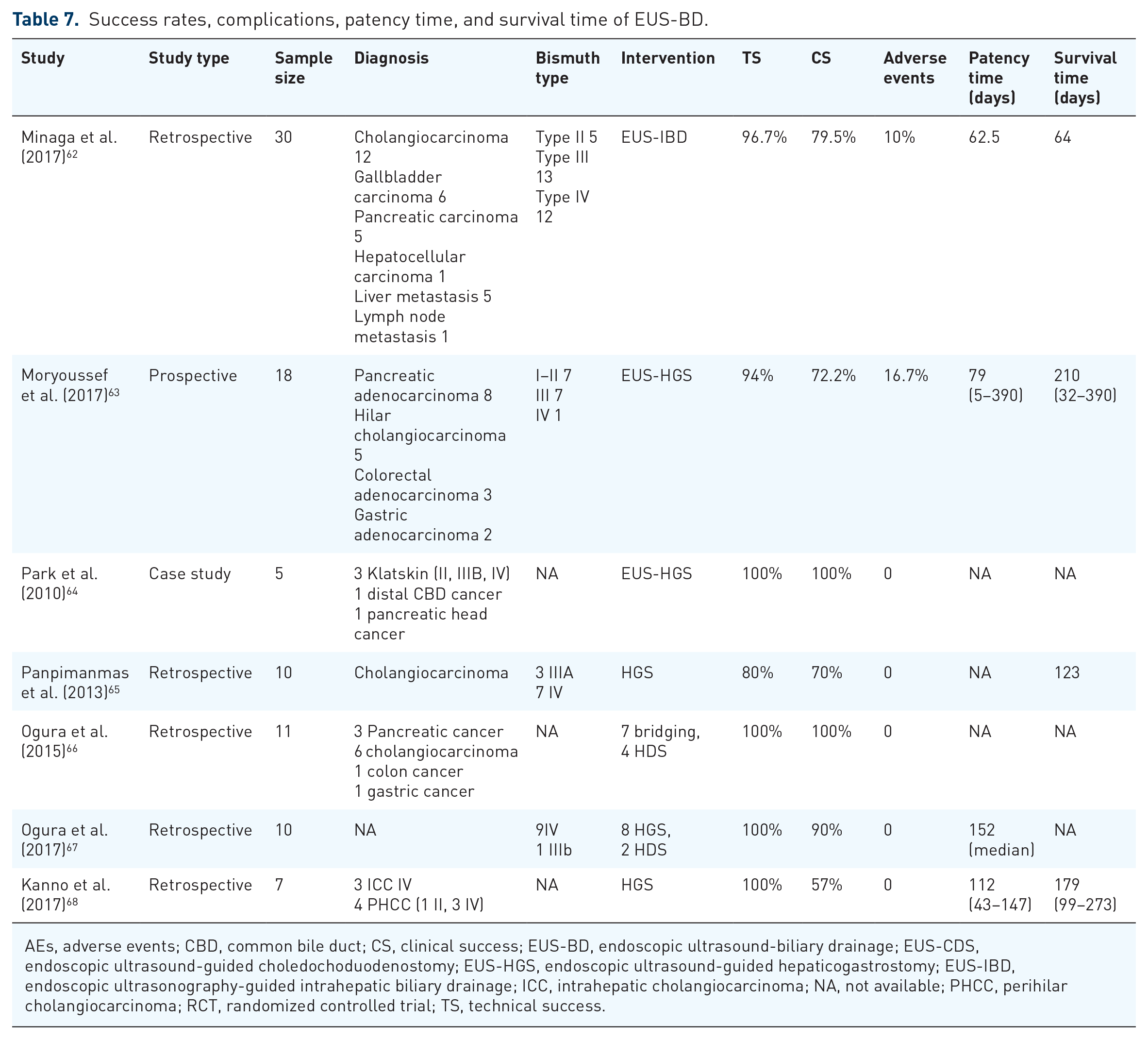
AEs, adverse events; CBD, common bile duct; CS, clinical success; EUS-BD, endoscopic ultrasound-biliary drainage; EUS-CDS, endoscopic ultrasound-guided choledochoduodenostomy; EUS-HGS, endoscopic ultrasound-guided hepaticogastrostomy; EUS-IBD, endoscopic ultrasonography-guided intrahepatic biliary drainage; ICC, intrahepatic cholangiocarcinoma; NA, not available; PHCC, perihilar cholangiocarcinoma; RCT, randomized controlled trial; TS, technical success.
In contrast to MDBO, where the obstruction is typically located lower and often accompanied by significant dilation of the common bile duct and intrahepatic bile ducts, EUS-BD can be effectively performed via puncture drainage from the duodenum or stomach, yielding generally positive outcomes.88,89 However, the complexity of EUS-BD significantly increases when addressing PHCC due to anatomical constraints, making puncturing the right liver lobe particularly challenging. In Bismuth type I, drainage can be effective, as the right and left hepatic ducts are interconnected, resulting in outcomes comparable to ERCP. Thus, EUS-guided hepaticogastrostomy (EUS-HGS) serves as a viable alternative when ERCP fails. In Bismuth type II, although the primary bile duct branches are involved, it is still possible to navigate a guidewire through the narrowed segment and position a multi-side hole stent, facilitating drainage of both liver lobes. Similarly, for type IIIA, EUS-HGS can effectively drain the left liver lobe, particularly if the left lobe is dominant and the drainage volume exceeds 50%, which leads to satisfactory results. 63 However, for types IIIB and IV, the difficulty of puncture is significantly increased, and single-lobe drainage often proves insufficient for effective drainage. 62 Nonetheless, Ogura et al. 67 demonstrated that among 10 patients who failed ERCP-guided reintervention (nine with type IV and one with type IIIB), EUS-BD was carried out with a technical success rate of 100%, and no adverse events were reported. To preserve as much viable liver parenchyma as possible, Kongkam et al. 90 first proposed the CERES approach (EUS-HGS with right biliary SEMS via ERCP or EUS-HDS with left biliary self-expanding stent via ERCP). The same team conducted a multicenter, open-label, observational study comparing the CERES technique with PTBD for MHBO, which included 33 cases of Bismuth type III or IV PHCC and some other cancers. This study demonstrated similar technical success, clinical success, and complication rates between the two methods. The rates of recurrent biliary obstruction and reintervention were significantly lower in CERES groups (26.7% vs 88.2% within 3 months and 22.2% vs 100% in 6 months, p < 0.05). In addition, the median drainage patency period was longer in the CERES group compared to the PTBD group (92 vs 40 days, p = 0.06). 90 However, it is worth noting that this technique involves a higher degree of difficulty. 91
While ERCP-BD remains the standard drainage approach for PHCC, EUS-BD is primarily utilized in patients who have failed or impossible ERCP. There is a noticeable lack of reports comparing initial EUS-BD versus ERCP-BD for PHCC.14,81 Current studies have predominantly focused on MDBO.88,89,92 Consequently, high-quality RCTs are needed to address the comparison of initial EUS-BD versus ERCP-BD in patients with PHCC.
The applications of POCS in unresectable PHCC treatment
POCS can significantly enhance the diagnostic efficiency for indeterminate biliary strictures (IDBS) through direct visualization and targeted multi-site biopsy sampling.93–97 And a recent meta-analysis demonstrated the high sensitivity and specificity of POCS in the visual interpretation of IDBS and malignancies. 98
Another important application of POCS is in guiding direct visual biliary selection cannulation. Conducting these procedures solely under digital subtraction angiography guidance can be challenging, and “false passages” may occur even during guidewire selection, exacerbating potential complications. Utilizing POCS in this context reduces the occurrence of stent-related complications and enhances the drainage efficacy of multiple stents during ERCP. 99
Furthermore, POCS allows for a visual assessment of local treatment effects of PHCC, such as RFA and PDT. A study by Talreja et al. 100 included 45 PHCC patients, consisting of Bismuth Type I–IV, who underwent PDT treatment guided by either ERCP or POCS. The results indicated that the median survival time in the ERCP group was lower (200 days) compared to the POCS group (386 days), although this difference was not statistically significant (p = 0.45). In addition, POCS significantly reduced fluoroscopy time, with averages of 21.1 min for ERCP compared to 11.1 min for POCS (p < 0.0001).
In recent years, AI has demonstrated great potential in the endoscopic assessment and management of biliary cancer, with several studies exploring its application in diagnosing biliary malignancies. For example, Saraiva et al. 101 developed a convolutional neural network (CNN)-based system in 2022 that accurately detects and differentiates malignant strictures in benign biliary diseases. Similarly, Marya et al. 102 developed a CNN model in 2023 that exhibited greater accuracy for biliary stricture classification compared to traditional ERCP-based sampling techniques.
RFA and PHCC treatment
Current status of RFA in cholangiocarcinoma treatment
RFA through two primary mechanisms in tumor treatment. First, it induces thermal damage that directly destroys tumors through coagulative necrosis and cell death. Second, the release of intracellular components can activate both local and systematic anti-tumor immunity. Percutaneous RFA has been routinely employed in various malignancies, including hepatocellular carcinoma, liver metastases, intrahepatic cholangiocarcinoma, and non-small-cell lung cancer. The advent of flexible catheters, such as Habib HPB-RF probe (Boston Scientific, America) and ELRA RF catheter (Taewoong, Korea), has made endoscopic RFA procedures feasible103–106 (Table 8).
Efficacy and safety of endoscopic radiofrequency ablation.

CI, confidence interval; NA, not available; OS, overall survival; SEMS, self-expanding metal stent; PEP, post-operative pancreatitis.
Stent alone versus RFA plus stent treatment in PHCC
In addition to inducing tumor necrosis and immune activation, RFA has demonstrated a synergistic effect when combined with BD via stent implantation. Survival rates associated with RFA combined with stenting are generally superior to those of stenting alone. A large cohort study by Xia et al. in 2021 121 demonstrated that combined RFA significantly improves overall survival in extrahepatic cholangiocarcinoma compared to stenting alone (9.5 vs 6.1 months, p < 0.01). A multi-center RCT conducted by Gao et al. 115 revealed that combined endoscopic RFA significantly improved overall survival (14.3 vs 9.2 months, p < 0.01) and quality of life, although this study included some distal cholangiocarcinoma cases. Additional research supported the notion that combining RFA with stent implantation can prolong overall survival and stent patency (Table 9). Despite discrepancies in results across different studies, the therapeutic effect of RFA combined with stenting shows potential advantages in diverse contexts, particularly among specific patient populations. Future studies should further explore the applicability of different types of stents to optimize treatment strategies. 116
Comparison of the overall survival and stent patency of RFA plus stent and stent alone.

BPS, bilateral plastic stent; CI, confidence interval; MD, mean difference; RCT, randomized controlled trial; RFA, radiofrequency ablation; SEMS, self-expanding metal stent; NR, not reported.
RFA plus chemotherapy/targeted therapy/immunotherapy in PHCC treatment
Limited studies have explored the combination of RFA with other therapies for PHCC. A retrospective study by Gonzalez-Carmona et al. 127 compared conventional RFA combined with first-line chemotherapy (gemcitabine plus platinum derivatives) for advanced extrahepatic biliary tract cancer. The results revealed that the combination group significantly improved overall survival (17.3 vs 8.6 months, p = 0.004) and progression-free survival (12.9 vs 5.7 months, p = 0.045). Another retrospective study by Inoue et al. 109 evaluated the efficacy of RFA combined with gemcitabine plus cisplatin for unresectable extrahepatic biliary tract cancer, showing longer periods of biliary obstruction recurrence (10.7 vs 5.2 months, p = 0.048) and higher overall survival (23.1 vs 16.6 months, p = 0.032) for locally advanced tumors, with no significant difference in the incidence of various toxicities between the groups. An RCT by Yang et al. 128 demonstrated that RFA combined with the novel drug S-1 resulted in significantly longer overall survival (16.0 vs 11.0 months, p < 0.001), stent patency time (6.6 ± 1.5 vs 5.6 ± 0.1 months, p = 0.014), and higher Karnofsky Performance Status scores at 9 months (51.6 ± 17.0 vs 40.4 ± 16.4, p = 0.012) and 12 months (35.2 ± 18.3 vs 23.9 ± 11.4, p = 0.014) compared to RFA alone, with no significant difference in ERCP-related complications. Gou et al. 129 conducted a multi-center retrospective cohort study comparing the efficacy and safety of RFA combined with hepatic arterial infusion chemotherapy (oxaliplatin and 5-fluorouracil) and stent placement against stent placement alone for treating advanced biliary tract cancer with biliary obstruction. The results showed that the combination therapy group had a significantly longer stent patency time (8.2 vs 4.3 months, p < 0.001) and overall survival (13.2 vs 8.5 months, p < 0.001) compared to the stent-alone group, with no statistically significant difference in the incidence of procedure-related adverse events between the two groups. Further studies are needed to evaluate the efficacy of combining RFA with chemotherapy, immunotherapy, and targeted therapy for PHCC.
Endoscopic PDT in PHCC treatment
PDT was first demonstrated by Ortner et al. 130 in 1998 as an effective method for restoring BD, improving quality of life, and prolonging survival in patients with unresectable cholangiocarcinoma. In a subsequent prospective randomized study conducted in 2003, which included 39 patients with unresectable Bismuth types II–IV PHCC, it was shown that PDT significantly extended the median survival time (493 vs 98 days, p < 0.0001) while also enhancing BD and quality of life 131 . A RCT conducted by Zoepf et al. 132 in 2005 involved 31 patients with unresectable Bismuth type IV cholangiocarcinoma and 1 patient with type II lymph node involvement. This study found that the combination of stent placement and PDT significantly improved overall survival (21 vs 7 months, p = 0.01). In addition, the PDT group exhibited a notable reduction in bilirubin levels (decreasing from an average of 2.75 to 1.3 mg/dL), with no significant difference in adverse events between the two groups. A large retrospective study by Dolak et al. 133 in 2017 included 88 patients who underwent a total of 150 PDT procedures. Among these patients, 79 had Klatskin tumors (including 4 Bismuth type I, 3 type II, 15 type III, and 57 type IV). The results indicated that the median duration of stent patency was 246 days (95% CI: 203–289), with median survival from the first PDT being 12.4 months (95% CI: 9.7–14.9). Cox regression analysis identified the number of PDT treatments as the only independent prognostic factor for survival in multivariate analysis (p = 0.048). Notably, among these patients, 24 received chemotherapy and 9 underwent curative liver surgery. A meta-analysis conducted by Moole et al. 134 in 2017, compared the outcomes of PDT combined with biliary stenting versus biliary stenting alone. The results indicated that the PDT group achieved better BD, with an OR of 4.39 (95% CI: 2.35–8.19), and prolonged survival, as well as higher Karnofsky scores compared to the stenting alone group, alongside a lower incidence of cholangitis (OR = 0.57, 95% CI: 0.35–0.94), although this analysis exhibited higher heterogeneity. Other studies have also supported the notion that combining PDT with stenting can prolong survival, improve quality of life, and restore BD without increasing adverse events. While PDT may cause phototoxicity, no fatal events have been reported, and most side effects can be managed locally (Tables 10 and 11).
Efficacy and safety of photo dynamic therapy.

CI, confidence interval; NA, not available; PDT, photodynamic therapy; TB, total bilirubin.
Comparison of the overall survival of PDT plus stent and stents alone.

CI, confidence interval; PDT, photodynamic therapy; RCT, randomized controlled trial; TB, total bilirubin.
In comparison, RFA offers advantages such as lower cost and no phototoxicity but requires direct access to lesions for effective ablation. PDT, conversely, allows for repeated interventions and can target peripheral or inaccessible lesions, making it a potential downstaging therapy prior to surgery or transplantation. Overall, both RFA and PDT have demonstrated efficacy in improving survival outcomes for patients with unresectable PHCC. 145 Some guidelines recommend both RFA and PDT for patients with PHCC.14,17 But limitations exist, their use may not be permitted in certain countries as off-label treatments; for example, France does not recommend their implementation outside of clinical trial settings 18 and PDT may not be FDA approved.
Conclusion
The continuous advancement of endoscopic technology has increasingly underscored its pivotal role in the diagnosis and treatment of PHCC. In terms of diagnosis, combining traditional ERCP imaging and cytological brushing with POCS-guided biopsy and EUS-guided puncture sampling can significantly enhance the diagnostic yield for PHCC. In treatment, bile duct drainage remains the primary therapeutic approach for PHCC, as it is essential for improving liver function and paving the way for chemotherapy and targeted therapies. Contrary to common belief, PTBD does not show a clear advantage over endoscopic internal drainage techniques in reducing the incidence of biliary infections, according to multiple studies. However, PTBD carries a risk of complete bile loss, which can adversely affect digestion and absorption, thereby significantly impacting survival and treatment outcomes. By contrast, endoscopic bile duct drainage more effectively aligns with physiological needs by reconstructing the enterohepatic circulation of bile acids. When combined with ENBD, it can reduce the risk of infection. If necessary, this approach can be converted to a biliary stent in a secondary procedure or performed alongside a biliary stent in a single procedure to balance the benefits of internal and external drainage. Furthermore, ERCP can safely and effectively place multiple stents to improve liver function when conducted under direct endoscopic visualization using POCS.
In cases where ERCP fails, EUS-BD serves as a viable supplementary technique. Beyond bile duct drainage, integrating endoscopic with catheter-based RFA, PDT, and systemic treatments can further prolong stent patency and overall survival. The emergence of innovative endoscopic diagnostic and therapeutic techniques has significantly expanded treatment options for unresectable PHCC patients. Nevertheless, further large-scale RCTs are necessary to validate the therapeutic efficacy of these techniques in the context of unresectable PHCC.