
Abstract
Background:
Endoscopic papillary balloon dilation (EPBD) has been recommended as a potential alternative to endoscopic sphincterotomy for common bile duct stones (CBDS), due to protecting the sphincter function.
Objectives:
This retrospective study aims to evaluate the safety and efficacy of endoscopic nasobiliary drainage (ENBD) versus endoscopic retrograde biliary drainage (ERBD) after EPBD for CBDS.
Design:
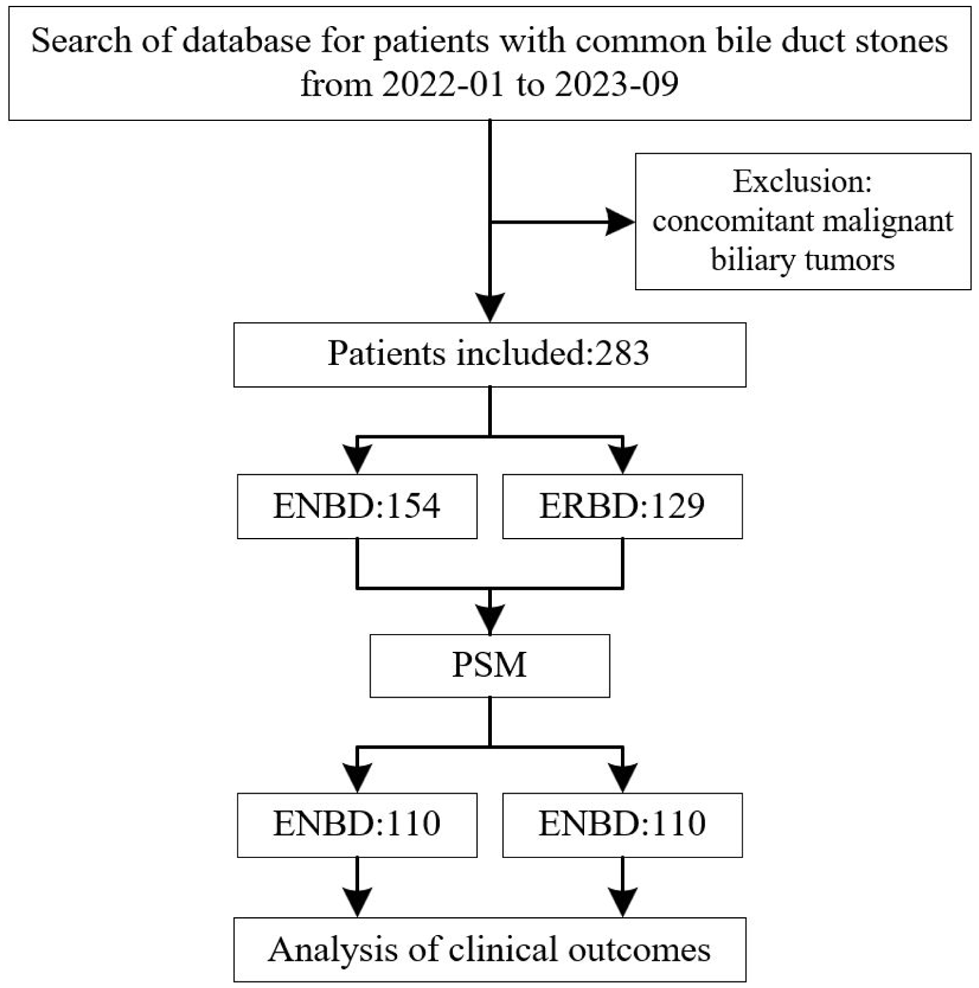
This study is a retrospective analysis of patients with CBDS who underwent EPBD followed by either ENBD or ERBD. It enrolled 283 patients, who underwent slow dilation and long-duration EPBD for CBDS with ENBD (eNbd group, n = 154) or ERBD (eRbd group, n = 129) from January 2022 to September 2023.
Methods:
Propensity score matching (PSM) was used to balance preoperative baselines and intraoperative specifics, resulting in 220 matched patients (110 patients per group). The incidence rate of post-ERCP pancreatitis (PEP) was compared between the two groups, and risk factors for PEP were analyzed.
Results:
After PSM, there were no significant differences in the baseline between the eNbd group and the eRbd group. The eNbd group exhibited significantly greater reduction in serum bilirubin levels compared to the eRbd group. Before PSM, the incidence rate of PEP was 2.6% (4/154) in the eNbd group and 8.5% (11/129) in the eRbd group (p = 0.027). After PSM, the incidence rate of PEP was 2.7% (3/110) in the eNbd group and 9.1% (10/110) in the eRbd group (p = 0.045). In addition, subgroup analysis revealed that patients with multiple stones may have a higher likelihood of developing PEP.
Conclusion:
ENBD may be an optimal choice for patients with CBDS undergoing EPBD, and the presence of multiple stones may be particularly relevant when considering the risk of PEP.
Plain language summary
Keywords
Introduction
Endoscopic retrograde cholangiopancreatography (ERCP) is currently the gold standard in the diagnosis of pancreaticobiliary disease, and is considered the first choice in the treatment of common bile duct stones (CBDS).1–3 In 1974, Classen and Demling 4 and Kawai et al. 5 performed the endoscopic duodenal papillary sphincterotomy (EST), significantly improving the success rate and accomplishing a complete removal of CBDS. However, EST has a relatively high risk of short- and long-term complications. Besides bleeding and perforation, EST-induced destruction of the Oddi’s sphincter results in cholangitis, cholecystitis, the recurrence of bile duct stones, and even the occurrence of cholangiocarcinoma.6,7 In 1983, Staritz et al. 8 first introduced endoscopic papillary balloon dilation (EPBD) for the removal of CBDS while protecting sphincter function and reducing the probability of bleeding, perforation. Thus, EPBD is recognized as a potential alternative for EST.
However, EPBD is always thought to be associated with post-ERCP pancreatitis (PEP),9–11 though Fujisawa et al. 9 reviewed 13 randomized controlled trials (RCTs) comparing EPBD and EST, and found that there was no significant difference of PEP in 10 RCTs, indicated that the lower maximum pressure and shorter ballooning time might be related to PEP. Therefore, it is usually concerned to reduce the risk of PEP after EPBD. Endoscopic nasobiliary drainage (ENBD) is a simple and rapid method for biliary decompression; moreover, several studies indicated that ENBD prevented the occurrence of PEP, especially post-EPBD pancreatitis.12–15 However, the catheter of ENBD is easy to be dislodged or removed by some patients, 16 and make the patients feel nasopharyngeal discomfort, which can affect the patient’s quality of life. In contrast, indwelling stents by endoscopic retrograde biliary drainage (ERBD) cannot be removed by the patient and are relatively more comfortable than ENBD. Furthermore, ERBD is equally effective for patients with acute suppurative cholangitis caused by bile duct stones like ENBD, thus gaining application. 17 However, it is unclear the role of ERBD on preventing post-EPBD pancreatitis.
Therefore, the aim of this study is to retrospectively compare the efficacy and safety of the efficacy of ENBD versus ERBD in preventing post-EPBD PEP for CBDS.
Materials and methods
Patients
This study retrospectively analyzed the data of 283 patients who underwent ERCP with EPBD for the management of CBDS and received either ENBD or ERBD at the First Affiliated Hospital of Sun Yat-sen University from January 2022 to September 2023. According to biliary drainage, the patients were divided into two groups, eNbd group (n = 154) and eRbd group (n = 129). Patients with concurrent malignant biliary tumors or missing group variables were excluded. We collected the data on patient demographics, preoperative baseline conditions, procedure details, and postoperative complications. The baseline variables of patients were matched and imputed using k-Nearest Neighbor Imputation. After propensity score matching (PSM), 220 patients remained, including 110 per group.
The diagnosis of CBDS was based on the results of abdominal CT, hepatobiliary ultrasound, or magnetic resonance cholangiopancreatography. Coagulation disorders were corrected before ERCP, and antibiotics were administered postoperatively if evidence of infection were present. According to our center’s clinical experience and relevant literature, 18 antibiotics or somatostatin are not routinely used prophylactically in the postoperative period; these medications are only administered when a patient is diagnosed with cholangitis or pancreatitis. The reporting of this study conforms to the Strengthening the Reporting of Observational Studies in Epidemiology (STROBE) statement. 19
Endoscopic procedure
Patients signed informed consent forms, then were placed in the prone position, were given intravenous conscious sedation and local pharyngeal anesthesia. ERCP was performed with a side-viewing duodenoscope (TJF-240, JF-260V; Olympus Co. Ltd, Tokyo, Japan) by experienced endoscopists (>1000 ERCP procedures). A duodenoscope was inserted through the mouth to the descending part of the duodenum. After cannulating the common bile duct via the duodenal papilla, cholangiography was performed to record the location, diameter, and presence of stones. Then, slow dilation and long-duration EPBD alone were performed. The balloon (Boston Scientific Corp., Natick, MA, USA) was inflated using dilute contrast and gradually expanded slowly from the smallest diameter (6–7–8 mm dilation balloon), increasing 1 ATM every 15 s. After reaching the 8 mm diameter, the larger dilation balloon (8–9–10 mm dilation balloon) was replaced until the specified size was reached according to the size of stones. After the final ATM was maintained for more than 2 min, the balloon was deflated immediately. Based on the patient’s condition, selective dilation of the stenotic segment and stone extraction using a balloon or basket were performed. After assessing the location, diameter, and length of the biliary stricture, the decision to place a plastic stent (8.5 Fr × 12 cm, or 8.5 Fr × 10 cm, or 8.5 Fr × 7 cm; Boston Scientific Corporation, Marlborough, MA, USA) or nasobiliary drainage tube (8.5 Fr × 250 cm; Boston Scientific Corporation) was made according to the physician’s experience. Following the placement of the plastic stent or nasobiliary drainage tube, another cholangiography was conducted to ensure the patency of the drainage. For patients with ENBD, daily drainage volume and symptoms were monitored, and the tube was typically removed 3–14 days after ERCP. However, for patients with ERBD, they were suggested to remove the plastic stent 1–6 months after ERCP.
Evaluation parameters and complications
Multiple stones are defined as the presence of ⩾2 stones in the common bile duct, as detected by preoperative imaging or intraoperative X-ray cholangiography. 20 The European Society of Gastrointestinal Endoscopy 2016 guidelines suggest that difficult biliary cannulation is defined as one or more of the following situations: more than five contacts with the major duodenal papilla, or attempts at cannulation exceeding 5 min after contrast injection, or more than one accidental pancreatic duct cannulation or contrast injection. 21 Those with a total procedural volume exceeding 1000 cases are considered experts, while the rest are considered fellows. A small papilla is often flat, with a diameter not bigger than 3 mm. Literature indicates that patients with small papillae have a higher incidence of postoperative complications. Therefore, our study categorized papilla types into small papilla and other papilla. 22
PEP is diagnosed when there is a new onset (or increase) of pain in the upper abdomen, an elevation in pancreatic enzymes to at least three times the upper limit of normal 24 h after the procedure, and a hospital stay of at least two nights.23–25 The severity of PEP is classified as mild, moderate, or severe. If serum amylase levels are elevated without abdominal pain after ERCP, it is diagnosed as hyperamylasemia. Post-ERCP cholangitis is defined by fever (>38°C), leukocytosis, and abdominal pain attributed to biliary causes, in the absence of evidence for acute cholecystitis. Post-ERCP bleeding is defined as the occurrence of melena or hematemesis accompanied by a hemoglobin (Hb) decrease of at least 2 g/dL or requiring transfusion. Perforations include retroperitoneal or intestinal wall perforations documented by any radiological technique. The incidence of ERCP-related complications, including PEP, hyperamylasemia, perforation, bleeding, and cholangitis, was closely monitored.
Propensity score-matched analysis
To minimize potential confounders, we employed PSM using logistic regression on demographic and clinical characteristics. We performed 1:1 greedy nearest neighbor matching with the caliper of 0.45, using the R package MatchIt. This method assigned control units one by one without optimizing an overall criterion, ensuring that observed differences were attributable to the treatments rather than confounding factors. Each row corresponds to a specific covariate, with columns showing the mean or proportion values for each group, as well as the p-value before and after matching. The notable change in p-value after matching indicates that PSM effectively improved the covariate balance between the two treatment groups. This improvement allows for a more reliable comparison of treatment effectiveness by minimizing the potential influence of confounding factors.
Laboratory parameters
Key indicators, including red blood cell count (RBC), Hb, white blood cell count (WBC), platelet count (PLT), aspartate aminotransferase (AST), alanine aminotransferase (ALT), total bilirubin (TB), direct bilirubin (DB), as well as amylase and lipase, were analyzed in the comparison between the two groups. Pre-ERCP test indicators were derived from the most recent blood test before ERCP, while post-ERCP test indicators were taken from the first blood test on the day following ERCP.
Statistical analysis
Statistical analyses were conducted using SPSS (version 26.0; SPSS, Chicago, IL, USA) and R (version 4.2.2; R Foundation, Vienna, Austria). PSM was employed to address potential biases introduced by baseline characteristics. Categorical data were analyzed using Chi-squared tests or Fisher’s exact tests, while continuous data were assessed with Student’s t tests or Mann–Whitney U tests. For continuous variables with a normal distribution, means ± standard deviations (SD) were reported, whereas median (interquartile range) was used for skewed distributions.
Results
In this study, we retrospectively analyzed the medical records of 283 patients who underwent ERCP and EPBD with ENBD or ERBD for CBDS. The overall baseline characteristics of these 283 patients were presented in Table 1, including the eNbd group with ENBD (n = 154) and eRbd group with ERBD (n = 129). We found that some parameters showed imbalance between the two groups, such as gender, preoperative laboratory parameters (WBC, TB, DB, and PT), and acute cholangitis. To enhance baseline comparability and reduce confounding factors, we applied PSM. After matching, the balanced baseline characteristics were achieved (p > 0.05), and the sample size was reduced to 220 patients, with 110 patients per group, as shown in Figure 1.
Baseline characteristics of the eNbd and eRbd groups before and after PSM.

ALT, alanine aminotransferase; AST, aspartate aminotransferase; DB, direct bilirubin; eNbd, endoscopic nasobiliary drainage; eRbd, endoscopic retrobiliary drainage; Hb, hemoglobin; PLT, platelet count; PSM, propensity score matching; RBC, red blood cell count; SD, standard deviation; TB, total bilirubin; WBC, white blood cell count.
The enrolled patients’ demographics.
Intraoperative details of ERCP were meticulously documented, incorporating several indicators identified in guidelines as potential risk factors for ERCP-related complications, such as stone size, procedure time, intubation time, multiple stones, difficult cannulation, guidewire insertion into the pancreatic duct, balloon dilatation size, mechanical lithotripsy, with gallbladder stones, operator experience, papilla type, the presence with diverticulum and incomplete stones extraction, as shown in Table 2. The results demonstrated similar intraoperative conditions between the two groups before or after PSM.
ERCP procedure details of the eNbd and eRbd groups before and after PSM.

ERCP, endoscopic retrograde cholangiopancreatography; eNbd, endoscopic nasobiliary drainage; eRbd, endoscopic retrobiliary drainage; PSM, propensity score matching; SD, standard deviation.
On the first postoperative day, laboratory parameters were collected, including ALT, AST, TB, and DB, as shown in Table 3. We calculated the change in values by subtracting the preoperative levels from the postoperative levels in two groups, and analyzed their significant differences to evaluate the efficacy of these two drainage methods for the recovery of patients. Interestingly, we observed that the reduction level of serum TB in the eNbd group was significantly greater than that in the eRbd group (−17.0 ± 66.34 vs −7.4 ± 61.58 µmol/L, p = 0.008). Similarly, the change in DB of eNbd group was also remarkably greater than that of ERBD DB levels (−13.6 ± 67.97 vs −12.1 ± 77.02 µmol/L, p = 0.021). Moreover, the length of total hospital stay and post-ERCP hospital stay in the eNbd group were both shorter than those in the eRbd group (6.6 ± 4.42 vs 7.6 ± 4.58 days, p = 0.136; 3.6 ± 3.05 vs 4.2 ± 3.60 days, p = 0.251); however, no marked difference was found. In addition, the changes in ALT (eNbd −48.2 ± 128.29 U/L vs eRbd −37.8 ± 83.04 U/L, p = 0.507), AST (eNbd −45.2 ± 133.93 U/L vs eRbd −34.2 ± 78.99 U/L, p = 0.482) also showed no significant differences between the two groups.
Comparison of laboratory parameters measured on day 1 after ERCP between the eNbd and eRbd groups.

Data are expressed as mean (SD).
p < 0.05.
ALT, alanine aminotransferase; AST, aspartate aminotransferase; CI, confidence interval; DB, direct bilirubin; ERCP, endoscopic retrograde cholangiopancreatography; eNbd, endoscopic nasobiliary drainage; eRbd, endoscopic retrobiliary drainage; LS, least squares; TB, total bilirubin.
In the assessment of ERCP-related postoperative complications, as shown in Table 4, we present the results before and after PSM. Before PSM, among the 283 ERCP procedures, 15 patients (5.30%, 15/283) underwent PEP, including 4 cases (2.6%, 4/154) in the eNbd group and 11 cases (8.5%, 11/129) in the eRbd group. The difference between two groups was remarkable, p = 0.027. In addition, all cases belonged to mild pancreatitis. No significant differences were observed in other complications, such as hyperamylasemia, cholangitis, bleeding, and perforation. After PSM, there were 13 cases of PEP (5.91%, 13/220) among the 220 ERCP procedures, including 3 cases (2.7%, 3/110) in the eNbd group and 10 cases (9.1%, 10/110) in the eRbd group. The difference in PEP incidence between the two groups remained significant (p = 0.045). Similarly, other complications still showed no significant differences.
Incidence of ERCP-related adverse events between the eNbd and eRbd groups.

p < 0.05.
eNbd, endoscopic nasobiliary drainage; eRbd, endoscopic retrobiliary drainage; ERCP, endoscopic retrograde cholangiopancreatography; PEP, postendoscopic retrograde cholangiopancreatography pancreatitis.
The exploratory subgroup analyses for PEP occurrence, as shown in Table 5, reveal significant differences in ERBD and the presence of multiple stones. Specifically, ERBD and the presence of multiple stones was associated with a significantly higher risk of PEP in the eRbd group compared to the eNbd group, with an odds ratio (OR) of 3.50 (95% confidence interval (CI): 1.09–11.26, p = 0.036) and 2.12 (95% CI: 0.21–20.94, p = 0.043). Other factors such as gender, diabetes, acute cholangitis, acute pancreatitis, acute cholecystitis, chronic cholecystitis, difficult cannulation, guidewire insertion into the pancreatic duct, gallbladder stones, mechanical lithotripsy, operator experience, and incomplete stone extraction did not show significant differences in PEP occurrence between the two groups. These findings suggest that ERBD and the presence of multiple stones may be particularly relevant when considering the risk of PEP after EPBD for CBDS. Subsequently, we conducted a multivariate regression analysis and found that ERBD was still significantly associated with an increased risk of PEP, with an OR of 3.29 (95% CI: 1.02–10.66, p = 0.047), while the presence of multiple stones did not show a significant difference.
Exploratory subgroup analyses and multivariate analyses for PEP occurrence.

p < 0.05.
CI, confidence interval; eNbd, endoscopic nasobiliary drainage; eRbd, endoscopic retrobiliary drainage; Inf, infinity; PEP, postendoscopic retrograde cholangiopancreatography pancreatitis.
Discussion
This is the largest sample size study to date that evaluates and reveals the safety and efficacy of nasobiliary drainage versus stent drainage in patients with CBDS. Although this is a retrospective study, the preoperative patient baseline and intraoperative details were well-balanced and comparable after PSM. Upon comparison, we found no significant differences between the two groups in terms of liver function indicators, hospital stay duration, or complications such as hyperamylasemia, cholangitis, and bleeding. However, a significant difference in the incidence of PEP was observed. This finding may help enhance endoscopists’ understanding of drainage method selection after EPBD for CBDS and potentially promote further contemplation and advancement in endoscopic practice.
Based on our center’s clinical experience, papillary edema may occur after EPBD, which can promote the occurrence of postoperative complications. Moreover, the study by Zhang et al. 26 suggests that endoscopic biliary drainage by nasobiliary tube or biliary stent insertion is a simple and quick method for biliary decompression, especially for ENBD. In addition, with the continuous development of stents and delivery systems and advancements in technology, the placement of nasobiliary drainage tubes or biliary stents under ERCP has become a common method for biliary drainage after CBDS extraction. 27 ENBD is a surgical procedure for draining bile and relieving biliary obstruction, facilitating bile cytology examination and cholangiography. 28 Zhang et al. 29 indicated that preoperative ENBD effectively reduced hospital stay and prevented from postoperative bile leakage and duodenal papilla damage after laparoscopic cholecystectomy. However, throat discomfort can hinder ENBD as an initial drainage method. Compared to ENBD, biliary stents are easier to replace and can significantly improve patient comfort and adherence, thus are widely used. Additionally, some reports indicate that long-term stent placement can effectively reduce the size of difficult stones, facilitating mechanical lithotripsy.30,31 However, it is undeniable that patients with plastic stents placed during ERCP generally require another ERCP or gastroscopy procedure for stent removal after 3–6 months. This can lead to a higher incidence of complications and decreased patient comfort. The primary drawbacks of plastic stents also include poor biocompatibility, small diameter, and a propensity for blockage, leading to recurrent jaundice and pruritus. 32 Thus, the two procedures are both very effective biliary drainage with their own shortcomings.
In terms of efficacy, we found that there were significant differences in the reduction of the TB (eNbd −17.0 ± 66.34 vs eRbd −7.4 ± 61.58 µmol/L, p = 0.008), and DB (eNbd −13.6 ± 67.97 vs eRbd −12.1 ± 77.02 µmol/L, p = 0.021). However, no significant differences were observed between the two groups in terms of the reduction of AST, ALT, and length of hospital stay, or complications such as hyperamylasemia, cholangitis, and bleeding. The role of ENBD in emergency biliary drainage has been recognized. A retrospective study by Huang et al. 15 found that ENBD was superior to ERBD in terms of biliary drainage effectiveness, and the incidence of drainage tube occlusion associated with cholangitis was significantly higher in the eRbd group than in the eNbd group. This is consistent with our study results. Considering that ENBD drains through a nasobiliary tube, it may be more effective in dealing with bile that is highly viscous or infected, which could be the reason for its better performance in reducing the obstruction of drainage tubes. Furthermore, the eNbd group can undergo flushing through the nasobiliary drainage tube, diluting and aspirating the obstructions, thus resolving most cases of tube occlusion, whereas patients in the eRbd group may require additional ERCP procedures to replace the drainage tube or even emergency surgery.
In terms of safety, PEP is one of the most severe and common complications after ERCP, particularly after EPBD for CBDS.33,34 In terms of preventing PEP, ENBD is reported to block the occurrence of PEP effectively, while there is no ERBD-related literature for PEP after CBDS extraction. In a retrospective study comparing biliary strictures caused by benign and malignant diseases involving 1136 patients, plastic biliary stent placement was superior to self-expandable metallic stents in preventing PEP,35,36 because the latter might impede pancreatic juice outflow. Hence, we focus on the safety and efficacy of ENBD versus ERBD in preventing PEP after EPBD in patients with CBDS. In this study, we utilized the maximum sample size of data among single-center studies to analyze, and found that the total incidence of PEP was only 5.30% after simple slow dilation and long duration EPBD, which is lower than that in the current reported data. The results may be related to our experience: no sphincterotomy, slow dilation, and long duration EPBD, and biliary drainage. We further compared eNbd group with eRbd group, noticed that ENBD decreased the incidence of PEP from 8.5% to 2.6%, the difference was significant, p = 0.027. Then, we applied PSM to enhance baseline comparability and reduce confounding factors, and still observed that ENBD decreased the incidence of PEP from 9.1% to 2.7%; the difference was still significant, p = 0.045. The results supported that ENBD is superior to ERBD in preventing PEP after EPBD for CBDS.
To explore whether there are independent risk factors for the difference in the incidence of PEP between the eRbd group and the eNbd group, we conducted a subgroup analysis. Our subgroup analysis revealed that ERBD and multiple stones may be independent risk factors for PEP, with an OR of 3.50 (95% CI: 1.09–11.26, p = 0.036) and 2.12 (95% CI: 0.21–20.94, p = 0.043), respectively. Biliary stones have long been recognized as a risk factor for pancreatitis. 37 A study by Niels G Venneman et al. 38 found that patients with pancreatitis more frequently had sludge-like stones and multiple stones, which is consistent with our findings. The reason may be that the greater the number of stones, the higher the chance of them becoming impacted in the ampulla. In addition, the regular passage of stones can cause damage to the common channel and increase the pressure in the pancreatic and biliary ducts, further promoting the occurrence of pancreatitis. To further control for potential confounding factors, we conducted a multivariate regression analysis. The results indicated that ERBD remains an independent risk factor for the occurrence of PEP (multivariate analysis OR = 3.29, p = 0.047), while multiple stones did not show significant differences in the multivariate analysis. Our findings underscore the importance of ERBD or ENBD in the occurrence of PEP in patients with CBDS. Although multiple stones did not show significant differences in the multivariate analysis, their significance in the univariate analysis suggests that we cannot ignore their potential impact. This may imply that, in certain situations, multiple stones might influence the risk of PEP through other confounding factors that are not fully controlled by the multivariate model.
To analyze the reasons for better safety and efficacy of ENBD, we speculated that there were several factors. First, ENBD can more effectively drain bile, reducing bile accumulation in the bile ducts and thereby decreasing the chance of pancreatic irritation. Second, continuous drainage reduces bacterial growth in the bile ducts, helping maintain a low-pressure state in the biliary system and lowering the risk of bile reflux into the pancreas due to increased biliary pressure. In addition, the placement of ENBD is relatively simple and is less prone to blockage compared to biliary stents. Besides, ENBD can be combined with negative-pressure drainage, which can more effectively drain bile, alleviate biliary inflammation, reduce the damage and spasm of the pancreaticobiliary sphincter that may trigger PEP, and thereby decrease the incidence of PEP. Biliary stents may become obstructed due to biliary sludge or bacterial biofilm formation, leading to recurrent obstruction and subsequent inflammation and pancreatitis. Furthermore, biliary stents can exert continuous mechanical irritation on the bile duct walls, whereas ENBD tubes are typically thinner and softer, causing less irritation to the bile duct walls and thus reducing the risk of pancreatitis. Moreover, Sato et al. 12 speculated that ENBD may prevent pancreatic duct obstruction caused by residual stones or papillary edema.
This study primarily investigates the safety and efficacy of ENBD versus ERBD after EPBD in patients with CBDS. Compared to other studies, our study boasts the largest sample size among single-center studies. Moreover, our study incorporated factors that may increase the risk of pancreatitis or other complications during the procedure, as outlined in guidelines and literature, which many other studies have not included. This reduces the impact of confounding factors and allows for a more accurate focus on the differences between ENBD and ERBD. However, it is undeniable that this is a single-center retrospective study, and its results may be influenced by the specific medical environment, technical expertise, and patient population of the center, potentially limiting the generalizability to other medical settings. Therefore, multicenter, prospective RCTs are necessary to validate the generalizability and robustness of our findings.
In summary, the results of this study indicate that ENBD not only prevents post-EPBD pancreatitis but also provides better biliary drainage. Therefore, it is recommended to routinely place an ENBD catheter, rather than a plastic stent, after EPBD for CBDS extraction.
Conclusion
ENBD results in a significantly lower incidence of PEP after EPBD for CBDS, with a remarkably greater reduction of bilirubin, compared to ERBD. Therefore, ENBD may be an optimal choice for patients with CBDS undergoing EPBD.
Supplemental Material
sj-docx-1-tag-10.1177_17562848251365025 – Supplemental material for Endoscopic nasobiliary drainage is superior to biliary stent placement in preventing postendoscopic papillary balloon dilation pancreatitis
Supplemental material, sj-docx-1-tag-10.1177_17562848251365025 for Endoscopic nasobiliary drainage is superior to biliary stent placement in preventing postendoscopic papillary balloon dilation pancreatitis by Junlong Lin, Baifeng Qian, Zhichao Li, Jialin Chen, Kai Gao, Jianpeng Cai and Yunpeng Hua in Therapeutic Advances in Gastroenterology
Footnotes
References
Supplementary Material
Please find the following supplemental material available below.
For Open Access articles published under a Creative Commons License, all supplemental material carries the same license as the article it is associated with.
For non-Open Access articles published, all supplemental material carries a non-exclusive license, and permission requests for re-use of supplemental material or any part of supplemental material shall be sent directly to the copyright owner as specified in the copyright notice associated with the article.