
Abstract
Background:
If the guidewire becomes kinked by the needle, guidewire manipulation may be difficult, and can cause complications such as guidewire shearing or injury during endoscopic ultrasound (EUS)-guided hepaticogastrostomy (HGS). To overcome this matter, we have previously described a technical tip for preventing guidewire injury, termed ‘liver impaction technique’. However, its technical feasibility has been not reported in the setting of a large patient cohort.
Objectives:
The aim of study was to evaluate the clinical usefulness of the liver impaction technique during EUS-HGS.
Design:
Retrospective, single-center study.
Methods:
This retrospective study included consecutive patients who underwent EUS-HGS between April 2018 and September 2022. The primary outcome of this study was the technical success rate of guidewire insertion using the liver impaction technique.
Results:
A total of 166 patients were enrolled in this study. Initial successful guidewire insertion without using liver impaction technique was obtained in 108 patients (65.1%). Among 58 patients in whom guidewire insertion failed initially, guidewire advancement into the periphery of the bile duct was observed in 32 patients (55.2%) and into a non-interest bile duct branch was observed in 26 patients (44.8%). Liver impaction technique contributed to increasing the technical success rate of guidewire insertion from 65.1% to 95.8%. Overall, adverse events were observed in 12 patients (7.2%; bile peritonitis n = 9, cholangitis n = 3), and these adverse events were Grade I. Among patients who underwent liver impaction technique (n = 58), adverse events were observed in two patients (3.4%; bile peritonitis). Also, guidewire sharing was not observed in any patients during liver impaction technique.
Conclusions:
In conclusion, the liver impaction technique may be helpful during EUS-HGS to obtain successful guidewire insertion into the biliary tract of interest.
Keywords
Introduction
Endoscopic ultrasound (EUS)-guided biliary drainage procedures such as hepaticogastrostomy (HGS) have emerged as alternative biliary drainage techniques for patients with duodenal obstruction, surgical altered anatomy such as Roux-en-Y procedure, or failed endoscopic retrograde cholangiopancreatography (ERCP).1–4 HGS requires the following four steps: bile duct puncture, guidewire insertion, tract dilation, and stent deployment from the intrahepatic bile duct to the stomach. According to a previous Spanish study, guidewire insertion or manipulation is the most challenging of these steps. 5 If the guidewire becomes kinked by the needle, guidewire manipulation may be difficult and can cause complications such as guidewire shearing or injury. To overcome this challenge, we have previously described a technical tip for preventing guidewire injury, which is termed as ‘liver impaction technique’. 6 However, its technical feasibility has been not reported in the setting of a large patient cohort. Therefore, the aim of this retrospective study was to evaluate the clinical usefulness of the liver impaction technique during EUS-HGS.
Patients and methods
This retrospective study included consecutive patients who underwent EUS-HGS between April 2018 and September 2022. To evaluate the technical feasibility of the liver impaction technique under identical conditions, we used the same devices as in that study: a 19G needle (EZ shot 3 plus, Olympus Medical Systems Corp) and a 0.025-inch guidewire (VisiGlide 1; Olympus). Patients who underwent EUS-HGS using any other puncture needle (including a 22G needle) or guidewire were excluded from the study.
Technical tips for liver impaction technique and procedure protocol
After inserting the echoendoscope (UCT260; Olympus Optical, Tokyo, Japan) into the stomach, the left intrahepatic bile duct was identified. B3 was selected as the first choice of puncture site, but if B3 puncture was challenging, B2 was used as the alternative. The intrahepatic bile duct was punctured using a 19G needle, followed by injection of contrast medium, and insertion of a 0.025-inch guidewire into the biliary tract was then attempted through the needle.
Technical tips for the liver impaction technique are as follows. The guidewire is inserted into the biliary tract through the needle after puncture of the intrahepatic bile duct. If the guidewire is advanced into the periphery of the bile duct (Figure 1(a)), guidewire kinking and shearing of the guidewire against the needle tip can occur (Figure 1(b)). To prevent these adverse events, the needle itself is pulled into the hepatic parenchyma (Figure 1(c)). In doing so, the tip of the needle is impacted by the hepatic parenchyma and the angle between the needle and guidewire becomes obtuse; therefore, difficulties with guidewire shearing or injury cannot occur during guidewire manipulation (Figure 1(d)).
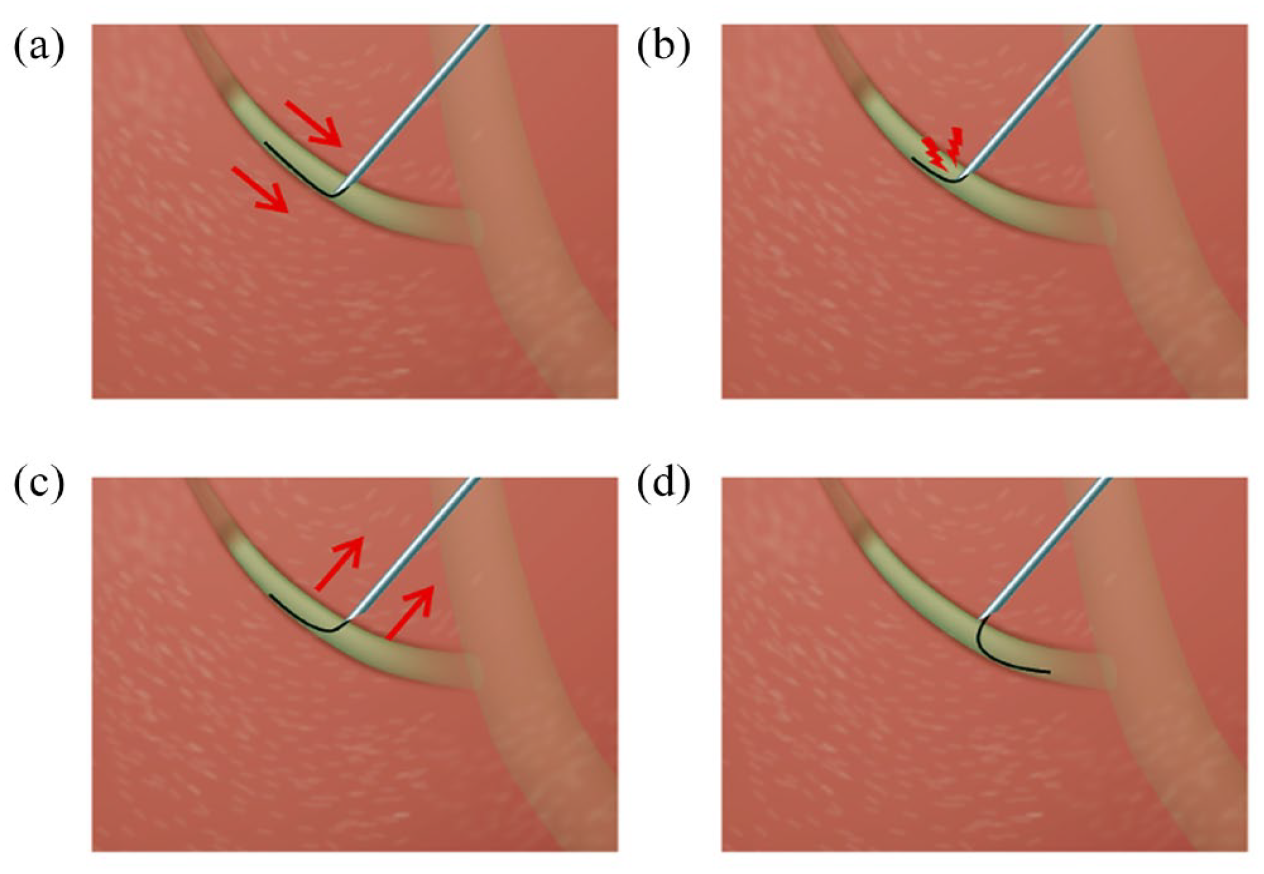
(a) The guidewire is advanced into the periphery of the bile duct, (b) guidewire kinking and shearing of the guidewire against the needle tip can occur, (c) the needle itself is pulled into the hepatic parenchyma, and (d) difficulties with guidewire shearing or injury cannot occur during guidewire manipulation.
Liver impaction technique can be applied if resistance is observed during guidewire withdrawal, during guidewire insertion into the periphery of the biliary tract (Figure 2(a)) through the needle, and also when changing direction to the bile duct of interest (Video 1) from a bile duct that is not of interest, such as B2 or other branches (Figure 2(b)). After successful guidewire insertion into the biliary tract of interest, tract dilation is performed using a 4-mm balloon catheter (REN biliary balloon catheter; KANEKA, Osaka, Japan) or ultra-tapered mechanical dilator (ES dilator; Zeon Medical Inc., Tokyo, Japan). Stent deployment is then performed from the intrahepatic bile duct to the stomach, using a plastic stent (Type IT stent; Gadelius Medical Co., Ltd., Tokyo, Japan) or partially covered self-expandable metal stent (8 or 10 mm × 10 or 12 cm, Niti-S or spring stopper stent, TaeWoong Medical, Seoul, South Korea) using the intra-scope channel release technique.

(a) Situation of guidewire insertion into the periphery of the biliary tract and (b) situation of guidewire insertion into non-interest bile duct, such as B2 or other branches.
Definitions and statistical analysis
The primary outcome of this study was the technical success rate of guidewire insertion using the liver impaction technique. Technical success of the liver impaction technique was defined as successful guidewire advancement into the left hepatic bile duct or common bile duct without guidewire shearing or injury. We used this definition because when inserting a dilation device or deploying a metal stent, a guidewire of sufficient length should be deployed into the biliary tract. The secondary outcome was the types of adverse events associated with the liver impaction technique. Procedure time was measured from echoendoscope insertion to successful stent deployment. Intraoperative bleeding event was defined as puncture-site hematoma, with continuous bleeding that required endoscopic and/or intravenous and/or surgical hemostasis around the puncture site. Bile peritonitis was diagnosed in the case of fever, elevated inflammatory markers on blood examination, and abdominal pain observed within 1 day after EUS-HGS, or based on the findings of bile leak or peritonitis around the HGS stent on computed tomography performed the day after EUS-HGS. Adverse events associated with EUS-HGS procedures were evaluated according to the severity grading system of AGREE classification. 7 Descriptive statistics are presented as the mean ± standard deviation (SD) or median and range for continuous variables and as the frequency for categorical variables.
Results
Table 1 lists the patient characteristics. A total of 166 patients (median age 76 years; 109 males and 57 females) were enrolled in this study. The primary diseases were mainly pancreatic cancer (n = 59) and cholangiocarcinoma (n = 24). EUS-HGS was also mainly performed in case of duodenal obstruction (n = 84) or surgical altered anatomy (n = 75). B3 was selected more frequently (n = 152) as the initial puncture site of the intrahepatic bile duct compared with B2 (n = 14). Mean diameter of the intrahepatic bile duct was 4.5 mm, and mean procedure time was 14.1 min.
Patient characteristics.

ERCP, endoscopic retrograde cholangiopancreatography; HGS, hepaticogastrostomy; SD, standard deviation.
Figure 3 shows the clinical results of liver impaction technique used in the present study. Among a total of 166 patients, initial successful guidewire insertion was obtained in 108 patients (65.1%). Among 58 patients in whom guidewire insertion failed initially, guidewire advancement into the periphery of the bile duct was observed in 32 patients (55.2%) and into non-interest bile duct branch was observed in 26 patients (44.8%). In all cases of guidewire advancement into a bile duct branch not of objective site, guidewire insertion into the left hepatic bile duct or common bile duct was successfully performed using liver impaction technique. However, in the case of guidewire advancement into the periphery of the bile duct, guidewire insertion failed in seven patients despite application of the liver impaction technique. These seven patients underwent EUS-HGS using a 22G needle or changed to another puncture site, followed by successful guidewire insertion in five patients. But bile duct puncture itself was failed in two patients. As a result, among 58 patients who were failed guidewire insertion, guidewire insertion was successfully performed in 51 patients after application of liver impaction technique. Therefore, liver impaction technique contributed to increasing the technical success rate of guidewire insertion from 65.1% to 95.8%. Finally, EUS-HGS was successfully performed in 164 patients (98.8%). Among successful EUS-HGS, partially covered metal stent was deployed in 144 patients, and plastic stent was in 20 patients. Overall, adverse events were observed in 12 patients (7.2%; bile peritonitis n = 9, cholangitis n = 3), and these adverse events were Grade I. Among patients who underwent liver impaction technique (n = 58), adverse events were observed in two patients (3.4%; bile peritonitis). Finally, guidewire sharing was not observed in any patients during liver impaction technique.

Flow chart in the present study.
Discussion
Technical tips for interventional EUS such as pancreato-biliary drainage or pseudocyst drainage commonly address the following: puncture, guidewire insertion, tract dilation, and stent or drainage tube deployment. Among these steps, guidewire insertion or manipulation may be the most limiting step. A Spanish national survey was performed regarding initial clinical experience in EUS-guided drainage. 5 Interestingly, in 125 enrolled patients who underwent EUS-guided drainage, the procedure was performed only by non-expert hands (experience of <20 procedures). They reported technical failure in 41/125 patients, which was the inability to manipulate the guidewire inside the duct in 28 patients. On this basis, they concluded that intraductal manipulation of the guidewire was the most difficult stage of the procedure. Therefore, to increase the technical success rate of EUS-HGS, several techniques are required to improve guidewire manipulation or to use a dedicated guidewire.
If the guidewire is advanced into the periphery of the bile duct from the puncture site or into a bile duct branch that is not of interest during EUS-HGS, it is necessary to withdraw the guidewire to change its direction. Withdrawal can cause injuring or shearing of the wire. To prevent this adverse event and improve the technical success rate, knuckle guidewire insertion may be a useful technique8,9 in the case of guidewire advancement into the periphery of the bile duct. If this adverse event occurs, a pushing force is applied to form the guidewire into a loop, after which it can be advanced into the hepatic hilar site while remaining in the loop shape. However, this technique has several limitations. First, there is a potential risk that the guidewire can penetrate the bile duct due to the pushing force required to form the loop. Although this adverse event is usually treated by conservative treatment, bile leakage can occur. 10 Second, the diameter of the intrahepatic bile duct must be wide enough to allow the guidewire to form a loop. Therefore, this technique can be challenging unless the intrahepatic bile duct is sufficiently dilated. Third, this technique is highly dependent on guidewire characteristics such as flexibility and stiffness, as reported in our previous experimental study. 11 Moreover, shearing or injury can occur when this technique is performed. 12 As an alternative technique, advancement of the guidewire to the desired site using an uneven double lumen catheter (UDLC) has been reported.9,13,14 The UDLC has two separate lumens: one at the tip that allows 0.025-inch guidewire insertion, and an additional side lumen through which a 0.035-inch guidewire can be inserted. Therefore, after this catheter is inserted, the guidewire can be manipulated and insertion can be attempted through another lumen if the guidewire is advanced into a bile duct that is not of interest. Although this technique can be useful, the UDLC catheter itself should be inserted into the biliary tract. Therefore, if the intrahepatic bile duct is difficult to access, this technique might be challenging. From the viewpoint of the needle used, a steerable access device for EUS-guided biliary drainage is available. 15 This novel puncture needle has a blunt-tipped access catheter that has a predetermined curvature (90° or 135°) and is fully totable. Therefore, wire shearing can be theoretically prevented because of the blunt tip and the coaxial orientation of the wire relative to the catheter tip. However, as the usefulness of this device is still unclear, further evaluation study is needed.
To improve the technical success rate of guidewire insertion, we previously evaluated the angle between the needle and echoendoscope during EUS-HGS. 16 The influence of this angle on failure of guidewire insertion was assessed using receiver-operating characteristic (ROC) curves. Area under the ROC curve was 0.86 [95% confidence interval (CI) 0.00–0.76], and an angle of 135° offered 88.0% sensitivity and 82.9% specificity for predicting successful guidewire insertion. Also, several authors have described the clinical importance of various angles, such as that between the needle and the intrahepatic bile duct,14,17 for inserting devices without tract dilation.
We should pay attention to the angle before bile duct puncture to improve the technical success rate of EUS-HGS; however, in clinical practice, adjusting to the appropriate angle before bile duct puncture can be challenging because of factors such as variation in anatomy, tumor size, and intervening vessels.
In contrast, the liver impaction technique can be performed without specialized devices or patient-dependent factors such as underdilation of the intrahepatic bile duct. Indeed, the technical success rate of guidewire deployment into the bile duct of interest increased from 65.1% to 98.8% in this study, without adverse events associated with the liver impaction technique. Compared with other methods, the liver impaction technique has several benefits. First, it can be applied in the case of nondilated intrahepatic bile duct, which increases the difficulty of forming the guidewire into a loop. Second, no adverse events are associated with this technique. Third, it is a cost-saving technique because another device is not needed. However, guidewire manipulation in the liver impaction technique must be performed by an experienced assistant or controlled by the physician. 18 Finally, this study has several limitations, including its single-center design and retrospective nature. It is necessary to conduct a further prospective comparison study with another technique.
In conclusion, the liver impaction technique may be helpful during EUS-HGS to obtain successful guidewire insertion into the objective biliary tract. These results should be further evaluated in a prospective randomized controlled trial.
Footnotes
References
Supplementary Material
Please find the following supplemental material available below.
For Open Access articles published under a Creative Commons License, all supplemental material carries the same license as the article it is associated with.
For non-Open Access articles published, all supplemental material carries a non-exclusive license, and permission requests for re-use of supplemental material or any part of supplemental material shall be sent directly to the copyright owner as specified in the copyright notice associated with the article.