
Abstract
Background:
Crohn’s disease (CD) and ulcerative colitis (UC) are chronic inflammatory bowel diseases (IBD) that have a negative impact on patient quality of life (QOL).
Objective:
To evaluate QOL, work productivity, use of healthcare resources, and medical costs in patients with IBD from the RISE-MX trial.
Design:
RISE-MX was a non-interventional, multicentric, cross-sectional, retrospective study conducted in a Mexican population with IBD.
Methods:
The 36-item Short Form Health Survey (SF-36) and the Inflammatory Bowel Disease Questionnaire (IBDQ) were used to assess QOL. The burden of disease was analyzed using the Work Productivity and Activity Impairment Questionnaire (WPAI), healthcare resources use, and medical costs.
Results:
Of 326 subjects, 95 (29.1%) had CD, and 231 (70.8%) had UC. In patients with CD, 43 patients (45.3%) showed moderate-to-severe activity, and 42 (18.1%) had moderate-to-severe disease activity in patients with UC. In all SF-36 dimensions, a significant difference between moderate-to-severe and mild activity/in remission groups was observed in patients with UC, while in patients with CD, the difference between activity groups was significant only for physical functioning and social functioning dimensions. In patients with CD, a higher but non-significant IBDQ score difference between activity groups was observed while a statistical difference between activity groups was observed for all dimensions in UC patients. In WPAI, the total percentage for work impairment (absenteeism plus presenteeism) and the percentage of regular daily activity impairment were statistically significant between activity groups only for UC. The annual total costs (direct and indirect) per patient in CD were USD 19,757 (moderate-to-severe activity group) and USD 12,587 (mild activity/in remission group), while in patients with UC were USD 11,702 and USD 9144, respectively.
Conclusion:
Moderate-to-severe activity of disease was associated with a substantial impact on QOL, work productivity, and medical costs in Mexican patients with IBD. Total costs were higher for patients with CD than for patients with UC.

Keywords
Introduction
Crohn’s disease (CD) and ulcerative colitis (UC) are chronic inflammatory bowel diseases (IBD) that lead to inflammation and digestive symptoms. While UC causes inflammation and ulceration limited to the colon and rectum, CD may affect any part of the gastrointestinal tract from the mouth to the anus.1–6 Although CD and UC are considered idiopathic diseases, many etiological factors can be attributed to CD and UC physiopathology, including genetics, immune disorders, and environmental factors.7–9
Globally, the reported prevalence of IBD ranges from 0.2% to 1.3%.10–15 IBD prevalence has been increasing in recent decades and varies among a number of sociodemographic characteristics, including age, race/ethnicity, socioeconomic level, education level, urbanicity, and employment status.11–17 Both CD and UC affect adult men and women equally and are diagnosed more frequently in urban areas than in rural areas.10–17 In Mexico, incidence and prevalence have increased steadily in recent years.18,19 A nationwide 15-year follow-up study in Mexico determined that incidence rates were 1.83, 1.45, and 0.34 cases per 100,000-person-year for IBD, UC, and CD, respectively. 20
Classically, the purpose of treatment for IBD is to suppress inflammatory response and control symptoms. In recent years, since the introduction of biological agents, the goal of treatment has advanced from achieving simple clinical remission to achieving deep and prolonged remission.21,22 One of the main goals of IBD therapy is to improve the patient’s health-related quality of life (QOL) by reducing inflammation and clinical symptoms.23,24 QOL is substantially lower in patients with IBD than in the general population due to the negative impact of the disease on physical, emotional, psychological, and social dimensions.25–34 Furthermore, hospitalizations, surgeries, or chronic use of drugs (e.g., steroids) may have an additional impact on patients’ QOL.23–28
Health-related QOL scales are commonly used in IBD clinical trials. Patient-reported outcomes (PRO) are frequently assessed by general QOL measurements such as the Short-Form 36 questionnaire (SF-36) or by disease-specific scales such as the Inflammatory Bowel Disease Questionnaire (IBDQ).23–33 Factors that can have a further impact on QOL include work productivity, as measured by the Work Productivity Activity Impairment Questionnaire (WPAI).24,30,34
The increasing IBD incidence and prevalence represent a heavy economic burden on society.10–15 The assessment of the burden of disease and related costs of IBD is important to define public health policies, resource allocation, and better patient care.35–41 The purpose of the RISE-MX study was to collect and describe real-world data from UC and CD patients diagnosed with moderate-to-severe disease in Mexico. In the present article, we report QOL and disease burden data, including direct and indirect costs of IBD, in patients with moderate-to-severe disease activity.
Methods
We used the Strengthening the Reporting of Observational Studies in Epidemiology (STROBE) statement guidelines to report this study. The STROBE checklist can be seen in Supplemental Material.
Study design and population
RISE-MX was a non-interventional, cross-sectional, retrospective, multicenter study conducted on IBD patients from 12 different sites in Mexico. A total of 335 patients were expected to be included regardless of the type of IBD (UC or CD). In the absence of information about the rate of UC or CD control in Mexico, it was assumed that 50% reflects the rate of inadequate disease control (i.e., the proportion of patients with moderate to severe disease). Therefore, a total of 318 patients with IBD (UC or CD) were estimated to provide results with a 95% confidence interval (CI) and a margin of error of less than 5.5%. The study had a cross-sectional evaluation (index date) to provide real-world data on disease activity, treatment patterns, burden of disease, and QOL in patients with moderate-to-severe UC or CD. The cross-sectional evaluation was conducted between 2021 August and May 2022. The study also included an additional retrospective review of medical records from the previous 3 years to describe IBD treatments and healthcare resource use. 4
Male or female patients were included if they were 18 years or older at the time of diagnosis of IBD. Diagnosis of IBD (UC or CD), according to Montreal classification,6,8 based on clinical, endoscopic, or imaging criteria, should have been established at least 6 months prior to the index date. Patients were excluded if they had indeterminate or unclassified colitis, disability due to mental illness, unwillingness to participate, or had participated in a clinical trial within the last 3 years. Patients with language barriers precluding adequate understanding or cooperation with the study were excluded.
Written consent according to the Declaration of Helsinki was obtained before the start of the study. The study was approved by the Local Ethics Committee of each site according to national regulations and was registered in clinicaltrial.gov (ID NCT04873700).
Study variables
Data were collected from patient’s medical records at the site. Sociodemographic characteristics QOL and burden of the disease questionnaires were collected at the Index date. Comorbidities, extraintestinal manifestations, previous treatments, surgeries, hospitalizations, medical appointments, calprotectin levels, colonoscopies, and follow-up studies (imaging and laboratory testing) were also collected considering retrospective data within the last 3 years.
CD activity was classified using the Harvey Bradshaw Index (HBI) 42 and/or the Crohn’s Disease Activity Index (CDAI).43,44 Moderate-to-severe CD was defined as patients with an HBI ⩾8 or a CDAI ⩾220, while mild or no activity (in remission) was determined by an HBI <8 or a CDAI <220.42–44 UC disease activity was determined using the partial Mayo score (pMayo score). Moderate-to-severely active UC was defined as pMayo ⩾5, and mild/in remission UC was defined as pMayo <5. 45
QOL and burden of disease
QOL and burden of disease were assessed using general and disease-specific questionnaires.
36-Item Short Form Health Survey (SF-36)24,25,30 is a general QOL questionnaire, which evaluates 8 health dimensions: physical functioning, bodily pain, role physical (limitations due to physical problems), role emotional (limitations due to personal or emotional problems), mental health, social functioning, vitality, and general health perceptions. Based on these eight dimensions, two weighted scores are generated: the physical component summary score and the mental component summary score. Scores range between 0 and 100, with higher scores indicating a better QOL. The mean score of each component (physical and mental) was used.
IBDQ23,24 is a disease-specific questionnaire with 32 items that measure 4 dimensions: bowel function, emotional status, systemic symptoms, and social function. Within dimensions, each question presents seven possible answers/points. Each domain score is the sum of eight responses each ranging from 1 to 7, where 1 indicates the worst function and 7 the best. The sub-score ranges from 8 to 56 and thus the total score ranges from 32 to 224, where a higher score indicates better QOL.
Work Activity Impairment Questionnaire (WPAI)24,30,34 assesses the impact of IBD on work productivity and daily activities over the previous 7 days. The WPAI includes 6 questions: 1 (if currently employed); 2 (hours missed due to disease); 3 (hours missed due to other reasons); 4 (hours actually worked); 5 (degree disease affected productivity while working); and 6 (degree disease affected regular activities). WPAI generates four component scores: percentage of work time missed (absenteeism); percentage of impairment while working (presentisms); percentage of overall work impairment (absenteeism and presentisms combined); and percentage of activity impairment. Scores for WPAI range from 0% to 100%, where 0% indicates no impairment and 100% is the total loss of work productivity/activity. Only employed participants were evaluated with this outcome measure.
Burden of disease and medical costs
The burden of disease and medical costs were evaluated based on comorbidities, extraintestinal manifestations, previous treatments, surgeries, hospitalizations, medical appointments, calprotectin levels, colonoscopies, and follow-up studies (imaging and laboratory testing). Comorbidities, extraintestinal manifestations, and previous treatment were previously published. 4
The calculation of direct costs was carried out using a micro-cost analysis that involved multiplying the use of resources by the relevant unit costs. A cross-sectional (human capital/income) analysis by proportional hours of absence/productivity (based on WPAI score) was used to determine indirect costs. Mexican reliable administrative databases from institutional sources were used to calculate unit costs. Data were collected from Groups Related to the Diagnosis (GRD-IMSS), updated with the National Institute of Statistics, Geography and Informatics (INEGI) expansion factor 2022, and the Mexican Institute of Social Security (IMSS) Unit Costs 2022. The Mexican Annual Program of Acquisitions, Leases, and Services, updated to September 2022, was used to estimate the price of the drugs. 4
Statistical analysis
Descriptive statistics (mean, median, standard deviation (SD), and minimum-maximum) were used to analyze sociodemographic, clinical, and treatment-related variables. Student’s t-test for independent samples or the Mann–Whitney test was used to compare CD and UC patients regarding continuous variables. Fisher’s exact test and the Chi-square test were used for categorical variables. All statistical tests were two-tailed, with a significance level of 0.05. SAS software (version 9.4; SAS Institute Inc., Cary, NC, USA) was used for all analyses. The analysis was designed to use complete cases, and missing data were not replaced with imputed values.
Results
Here we present the results of the RISE-MX study regarding QOL and the burden of disease. Briefly, of 335 enrolled IBD patients, 326 formed the analyzable population. Nine patients were excluded since they did not specify the IBD type or did not meet the criteria to evaluate disease activity. Of these 326 subjects, 95 (29.1%) received a CD diagnosis and 231 (70.8%) were diagnosed as UC. In the CD group, 43 patients (45.3%) had moderate-to-severe activity and 52 (54.8%) presented either mild activity or were in remission. In the UC group, 42 subjects (18.1%) showed moderate-to-severe activity while 189 (81.9%) reported mild activity or were in remission. Table 1 presents a summary of the main demographic characteristics of the patient population (N = 326).
Summary of the main demographic characteristics of patients with a diagnosis of an IBD (N = 326).

IBD, inflammatory bowel disease.
Regarding QOL assessment, Table 2 and Figure 1 present a summary of the SF-36 for CD and UC, where information about general health, physical functioning, bodily pain, role physical, role emotional mental health, social functioning, and vitality was collected at Index Date. The statistical difference for all these variables was significant for moderate-to-severe disease activity versus mild/in remission for UC (p = 0.0003; p = 0.0073; p = 0.0089; p = 0.0001; p = 0.0045; p = 0.0341; p = 0.0380; p = 0.0328, respectively; Figure 1(b)), but only for physical functioning (p = 0.0209), social functioning (p = 0.0382), and vitality (p = 0.0311) in the case of CD (Figure 1(a)).
Summary of SF-36 survey for CD and UC patients by Disease Activity at Index date.

Obtained from Chi-square/Fisher’s exact or Mann–Whitney/t-test.
Direct question from SF-36 questionnaire.
CD, Crohn’s disease; SF-36, 36-item short form; UC, ulcerative colitis.

Assessment of general health in the SF-36 for CD and UC patients by Disease Activity at Index date. (a and b) Outcomes of the eight domains and total score by disease activity group in CD and UC patients, respectively. (a) CD patients. (b) UC patients.
Table 3 and Figure 2 show the results of the IBDQ for CD and UC, measuring four dimensions (bowel function, emotional status, systemic symptoms, and social function). In all IBDQ dimensions, a lower score was observed in moderate-to-severe activity groups compared to mild activity/in remission groups, and statistical difference for all these variables was observed only for UC (p = 0.0000; p = 0.0066; p = 0.0124; p = 0.0000, respectively). The mean bowel function score was 47.5 in the moderate/severe activity group versus 52.4 in the mild activity/in remission group in the CD component, while it was 43.5 in the moderate-to-severe group and 54.3 in the mild/in remission group for the UC patients.
Summary of IBDQ for CD and UC patients by Disease Activity at Index date.

Obtained from Mann–Whitney or t-test.
CD, Crohn’s disease; IBDQ, inflammatory bowel disease questionnaire; UC, ulcerative colitis.

IBDQ for Crohn’s disease (a) and UC (b) patients by Disease Activity at Index date. (a) Health outcomes of the IBDQ in CD patients. (b) Health outcomes of the IBDQ in UC patients.
The emotional status score was 53.5 in the moderate/severe activity group, 57.1 in the mild activity/in remission group for those with CD, 53.0 in the moderate/severe activity group, and 59.5 in the mild activity/in remission group for those with UC. Systemic symptoms were rated as 19.8 in the moderate/severe activity and 22.2 in the mild activity/in remission group in patients with CD, and 20.6 in the moderate/severe activity versus 23.5 in the mild activity/in remission group of those with UC. The social function was rated as 24.3 in the moderate/severe activity group, 27.3 in the mild activity/in remission group in patients with CD, and 23.1 in the moderate/severe activity versus 28.5 in the mild activity/in remission group in patients with UC. That yielded a total score of 144.8 in the moderate/severe activity group versus 159 in the mild activity/in remission group in patients with CD, and 140.2 in the moderate/severe activity group versus 165.7 in the mild activity/in remission group of patients with UC.
Table 4 presents the results of the surveys for work productivity and activity using the Work Productivity and Activity Impairment (WPAI) Questionnaire. Considering work hours lost due to problems related to the disease, patients with CD presented a greater number of lost hours, absenteeism, and presenteeism compared to patients with UC. The absenteeism in CD patients was 19.9% for the moderate-to-severe activity of the disease and 17.3% for remission or mild activity. In UC patients, the results were 9.8% for moderate-to-severe disease activity and 10.6% for remission or mild activity. The total percentage for work impairment (absenteeism + presenteeism) and the percentage of regular daily activity impairment were statistically significant for moderate/severe versus mild/remission groups only for UC (p = 0.0360 and p = 0.0009, respectively).
Summary of WPAI questionnaire for CD and UC patients by Disease Activity at Index date.

Obtained from Chi-square/Fisher’s exact or Mann–Whitney/t-test.
In reference to the last 7 days.
CD, Crohn’s disease; UC, ulcerative colitis; WPAI, Work Productivity and Activity Impairment.
Regarding previous surgeries in the IBD population, the most frequent event is the “Fistulectomy/anal fistulectomy,” which was performed in 4.7% of patients with moderate-to-severe activity and 3.8% in the mild activity/in remission group of the CD component, and “Other type of surgeries” were reported in 4.7% of patients in the moderate-to-severe activity, and 3.8% in the mild activity/in remission group, in the same CD component. In the UC component, the most frequent surgery was “Total proctocolectomy with ileal pouch-anal anastomosis” in 2.4% of patients with moderate-to-severe activity and “Drainage of anorectal abscess” in 1.1% of patients with the mild activity/in remission group (Supplemental Tables 1–5).
Other outcomes such as hospitalizations, medical appointments, calprotectin levels, and laboratory results are presented in Supplemental Tables 1–5.
Finally, Table 5 summarizes estimations of direct and indirect medical costs. Direct and indirect costs in both activity disease groups were higher in patients with CD compared to patients with UC. Considering comorbidities, extraintestinal manifestations, previous treatments, medical appointments, hospitalizations, and other medical procedures, the annual direct costs per patient in CD were USD 19,026 (moderate-to-severe) and USD 12,127 (mild activity/in remission). In patients with UC, the direct costs were USD 11,516 (moderate-to-severe) and USD 8953 (mild activity/in remission).
Summary of direct and indirect medical costs for CD and UC by Disease Activity at Index date.
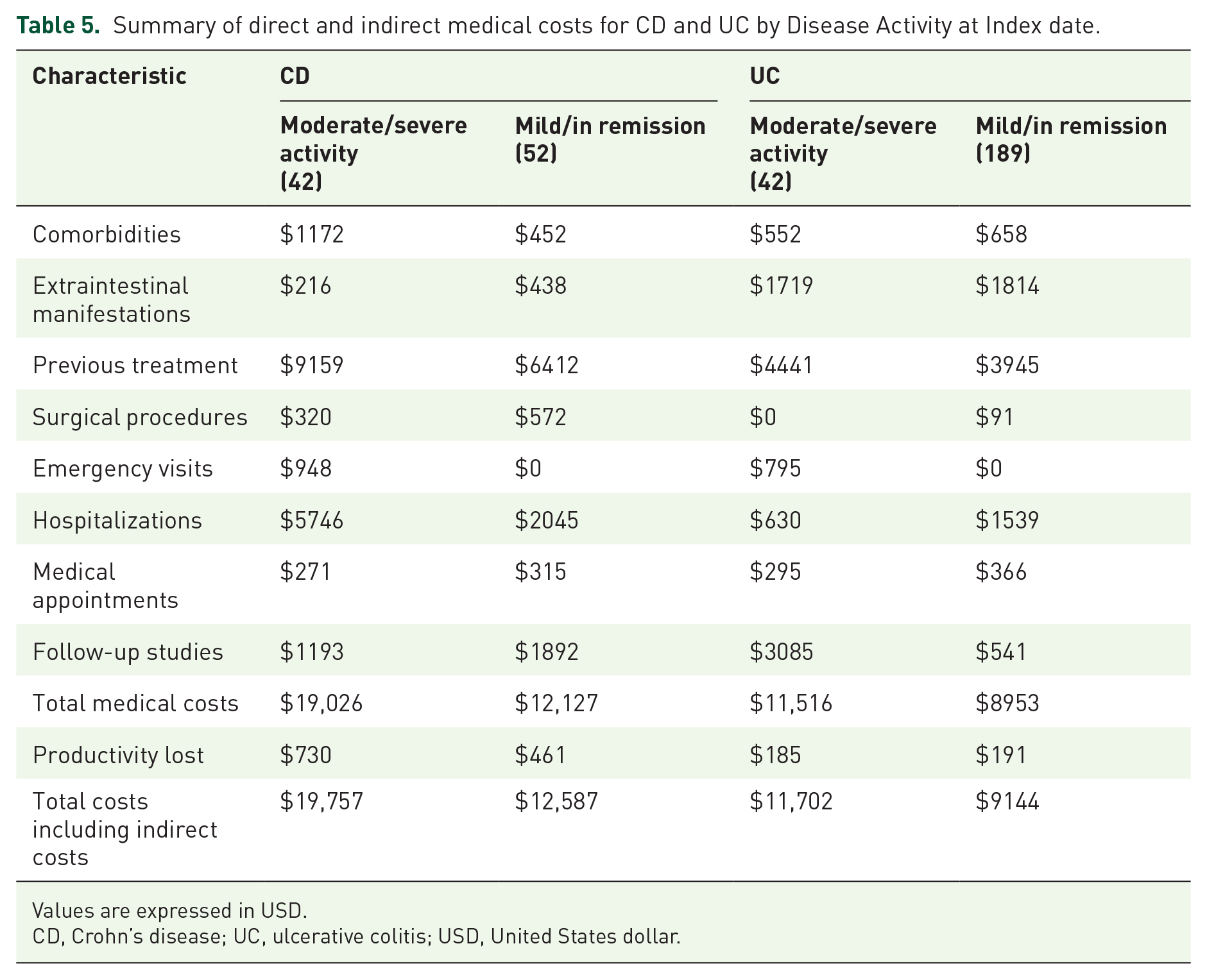
Values are expressed in USD.
CD, Crohn’s disease; UC, ulcerative colitis; USD, United States dollar.
The annual total costs per patient in CD were USD 19,757 (moderate-to-severe) and USD 12,587 (mild activity/in remission). In patients with UC, the total costs were USD 11,702 (moderate-to-severe) and USD 9144 (mild activity/in remission group).
In this analysis, the costs were calculated with information available on clinical records at the Index date. Due to the retrospective nature of the analysis, the use of healthcare resources may have differed among participating sites. In addition, due to activity change in moderate-to-severe patients, there could have been changes in patients’ journeys that resulted in higher costs at some point in this 3-year retrospective analysis. Considering that QOL was measured and sorted by activity on the Index date, it is not meaningful to associate specific costs with QOL outcomes. Total medical costs show consistency with disease activity measured at the Index date, also showing that CD involves higher costs than UC.
Discussion
In our study, 326 adult patients with CD (95 patients; 29.1%) or UC (231; 70.9%) were included. The evaluation of disease activity at index date (primary objective) showed that in the UC group, 189 (81.8%) patients had remission/mild activity and 42 (18.2%) had moderate-to-severe activity. In the CD group, 52 (54.2%) patients had remission/mild activity, and 43 (44.8%) had moderate-to-severe activity.
QOL is a broad, multidimensional concept that includes subjective evaluations of both positive and negative aspects of life.22–27 QOL is impaired to varying degrees in every patient with IBD, and many patients constantly live with decreased QOL. As observed in our study and other previous ones, IBD affects adults at a time in their lives when they are most likely to strive for education, employment, family planning, and personal achievements. Achieving these life milestones is often hindered by the debilitating symptoms, psychological comorbidities or consequences (anxiety, depression, sleep disorders), and social discomfort that are associated with IBD.27–30 Disease severity is the most significant predictor of disability and impact on daily activities. Measuring the disability associated with IBD and the impact of IBD on a person’s QOL is essential to understand the hidden burden of IBD for patients and society.30–36 Our results describe the impact of IBD severity in QOL, productivity, and indirect and direct costs reporting a higher burden in severe/moderate patients than mild/in remission patients.
We found that the IBDQ score in severe/moderate IBD patients is below 170 which corresponds with the score of patients with active disease 32 and it is lower than patients with mild/in remission activity which emphasizes the burden in the Mexican population. A systematic review of 45 observational studies reported the burden of IBD in the Spanish population from 2011 to 2021. 40 Authors reported lower QOL in IBD patients compared to the general population. IBD symptomatology was also associated with high levels of anxiety, depression, and stress. The use of healthcare resources included emergency department visits, hospitalization, surgery, and biologics. As we found in our study, these researchers concluded that CD and UC represent a great disease burden that leads to higher use of healthcare resources and negatively impacts patients’ QOL. 40
The SF-36 is an instrument commonly used to evaluate health-related QOL in patients with IBD. The SF-36 measures eight domains: physical functioning, role physical, bodily pain, vitality, role emotional, mental health, social functioning, and general health. This tool has demonstrated good cross-cultural adaptability, validity, and reliability.10–15,25 In our study, the difference between the moderate-to-severe activity group and the mild activity/in remission group was significant for all dimensions in UC patients, and only for physical functioning, social functioning, and vitality in patients with CD. The different number of patients in CD and UC groups may have influenced the statistical significance of domain results. For the perception of QOL in Mexican patients, the domain results with statistical significance may be considered the most relevant. The absence of statistical significance may be due to the fact that the impact of disease on QOL may be independent of the activity level.
In IBDQ, bowel function, emotional status, systemic symptoms, and social functioning were assessed.24–26,34 In our study, a higher score with no statistical significance was observed for all dimensions in moderate-to-severe activity compared to mild activity/in remission in patients with CD. Again, the absence of statistical significance is related to the fact that QOL may be affected independently of the activity level. Significant statistical difference was observed for all dimensions in patients with UC.
IBD has been associated with a negative impact on work productivity compared to the general population. 34 In our study, we found a total percentage of regular daily activity impairment in moderate/severe patients of 45.7% (CD) and 44.0% (UC), while the total percentage of work impairment in the same population was 20.3% (CD) and 24.2% (UC) which show the impact of IBD in Mexican workers. A multicenter cross-sectional study conducted on 407 IBD patients in Brazil found that moderate-to-severe activity was significantly associated with lower QOL. 34 Activity impairment was 30%, and it was considerably higher among patients with moderate-to-severe activity compared to those with mild or no disease activity. Median work productivity impairment was 20% and 5% for CD and UC patients, respectively. Parameters associated with a QOL decrease were female gender, being unemployed, a lower educational level, and low income. 34
WPAI, an important PRO for measuring QOL and burden of disease, showed in our study that more than half of patients were working in the last 7 days. In patients with CD, absenteeism, a rate of time work missed, did not reveal a significant difference between moderate-to-severe activity compared to mild activity/in remission. Presenteeism, that is, working while being sick despite having reduced productivity, did not show a significant difference between moderate-to-severe activity compared to mild activity/in remission in patients with CD. In patients with UC, absenteeism and presenteeism did not show a significant difference between moderate-to-severe activity compared to mild activity/in remission. The total percentage of work impairment, considering absenteeism and presenteeism together, was significant for UC patients for moderate-to-severe activity versus mild activity/in remission (24.2% vs 17.7%), but not for patients with CD (20.3% vs 21.2%, respectively).
In our study, the disability rate (absenteeism) of CD was 19.9% for moderate-to-severe activity and 17.3% for mild activity /in remission, comparable to the overall IBD disability rate reported in the IBSEN study (18.8%) 46 and the ECCO-EpiCom data (20% in the United States to 34% in Europe). 47 Burden of disease and costs were calculated based on comorbidities, extra-intestinal manifestations, previous treatments, previous medical appointments and emergency visits, and hospitalizations and other medical procedures. A total of 26.3% (25/95) of disease-related hospitalizations were reported in CD patients and 15.6% (36/231) for UC patients. The mean hospitalization duration was 26.7 days for patients with moderate-to-severe CD and 2.7 days for patients with moderate-to-severe UC. Hospital admission was a highly demanded service (26.3% for CD patients and 15.6% for UC patients) and represented a high percentage of costs. It is important to note that biological agents have been proven to reduce inflammation, the need for surgery, hospitalization, and most of the complications that characterize IBD.21,25,30
Considering comorbidities, extraintestinal manifestations, previous treatments, medical appointments, hospitalizations, and other medical procedures, the total annual costs (direct and indirect) per-patient impact in CD was USD 19,757 (moderate-to-severe) and USD 12,587 (mild/in remission). In patients with UC, the total cost (direct and indirect) was USD 11,702 (moderate/severe) and USD 9144 (mild/in remission). Therefore, a substantial difference was observed between the CD and UC groups, with total costs being considerably higher for patients with CD, as was also reported in previous studies. 35
In Canada, Kuenzig et al.37,38 calculated direct and indirect costs for patients with IBD. Direct costs of illness were based on the costs of medical services and treatments paid for by public and private payers, including hospital care, outpatient consultations, medications, diagnostic testing, and programmed home care. They estimated that the direct cost of caring for people with IBD in 2018 was approximately $4731 CAD (Canadian dollars) per patient, and the direct cost of caring for people living with IBD was estimated to be close to $1.28 billion CAD in 2018. 37 These authors affirm that IBD patients cared for by gastroenterologists have better outcomes than decades before, including lower risks of surgery and hospitalization. The rates of hospitalizations and major abdominal surgeries have been decreasing in IBD patients over the past two decades, possibly due to the increasing use of biologic agents and advances in patient management. 37 These authors also defined indirect cost as the portion of human capital that is missed due to lost productivity of patients and their caregivers (unemployment, absenteeism, and presenteeism) and the out-of-pocket healthcare expenses paid directly by patients. They calculated that the total annual indirect cost of IBD in Canada in 2018 was $4781 CAD per patient with IBD. The total indirect health-related cost of IBD in Canada in 2018 was estimated to be $1.29 billion CAD. 38 However, this may be an underestimation because costs related to presenteeism, reduced performance, and caregiver burden could not be assessed and were excluded from this estimate. 38
A questionnaire-based study among 3687 adult patients with IBD was performed to compare indirect costs of IBD between 12 European countries. 39 A significant difference in informal care and productivity loss was observed between countries. For example, the mean annual cost of absenteeism varied from €1253 in Bulgaria to €7915 in Spain; the cost of presenteeism ranged from €2149 (Bulgaria) to €14,524 (Belgium), and the cost of informal care varied from €1729 in Poland to €12,063 in Italy. Patients with IBD in remission showed a significantly lower indirect cost than those with active disease. 39
A recent study assessed the burden and cost of IBD from a societal perspective in Portugal and found that the average yearly cost (direct healthcare and non-healthcare costs) per IBD patient was EUR 6075, where 60% was related to CD and 40% to UC. 35
An interesting qualitative study recently conducted by Schoefs et al. 27 assessed unmet needs in IBD management according to patients’ preferences. The possible need for surgery or an ostomy, the effectiveness of their medication, and the long-term effects of medications were reported as the main worries for patients. For example, patients long-term treated with corticosteroids may experience a variety of physical changes such as moon face, hair loss, developing facial hair, and weight fluctuations, which have a negative impact on their QOL. Patients also stressed the emotional impact of IBD and their need for psychological guidance, support, and improved communication and information regarding the disease. In this study, some goals were identified as most important for patients. These included preventing surgery, achieving long-term clinical remission, improving QOL, and achieving an improvement in both the frequency and severity of gastrointestinal symptoms. Finally, reducing fatigue, while increasing energy levels and work capacity, was also considered of vital importance for patients. 27
Our study has some limitations owing to its non-interventional, cross-sectional, retrospective design. Information was based on a review of medical records that were originally not designed to collect data for research, and therefore some information may be missing. Self-assessment when using questionnaires or surveys may be unreliable and threatened by self-reporting bias. Recall bias at index date may also affect the results. The multicenter nature of the study may add some bias, especially considering that all clinical centers were located in major cities in Mexico, and in IBD some differences between urban and rural patients have been reported.
Conclusion
In our study, most patients presented UC diagnosis, and a considerable portion of patients presented moderate-to-severe activity, particularly in CD (45.3%). In SF-36, the difference between the moderate-to-severe activity group and the mild activity/in remission group was significant for all dimensions in UC patients, and only for physical functioning, social functioning, and vitality in patients with CD. In IBDQ, statistical difference was observed in all dimensions for UC, while a non-significant higher score was observed in moderate-to-severe activity groups compared to mild activity/in remission groups for CD patients.
The moderate-to-severe activity also caused work productivity impairment and was associated with an increased burden of disease and high medical costs, both direct and indirect. A notable difference was observed between CD and UC patients, with total costs being considerably higher for CD patients. Overall, these findings underscore the need to improve access to advanced therapies and a personalized approach to treatment to achieve optimal disease control and enhance the QOL of patients with IBD in Mexico.
Supplemental Material
sj-docx-1-tag-10.1177_17562848251318032 – Supplemental material for Quality of life and burden of disease in a Mexican population with inflammatory bowel disease: an analysis of the RISE-MX trial
Supplemental material, sj-docx-1-tag-10.1177_17562848251318032 for Quality of life and burden of disease in a Mexican population with inflammatory bowel disease: an analysis of the RISE-MX trial by Rosa M. Miranda-Cordero, Francisco J. Bosques-Padilla, Manuel Alejandro Martínez-Vázquez, Cristian Barajas-Maldonado, Mauricio M. Rodriguez-Mendoza and Jesús K. Yamamoto-Furusho in Therapeutic Advances in Gastroenterology
Footnotes
Acknowledgements
Editorial assistance, under the authors’ guidance, was provided by Content Ed Net (Madrid, Spain). Reprints Unlimited Mexico has performed editorial management and was funded by Takeda Mexico, S.A. de C.V.
Declarations
Supplemental material
Supplemental material for this article is available online.
References
Supplementary Material
Please find the following supplemental material available below.
For Open Access articles published under a Creative Commons License, all supplemental material carries the same license as the article it is associated with.
For non-Open Access articles published, all supplemental material carries a non-exclusive license, and permission requests for re-use of supplemental material or any part of supplemental material shall be sent directly to the copyright owner as specified in the copyright notice associated with the article.